Received: February 21, 2012, Revised: June 22, 2012, Accepted: December 27, 2012 ISSN 1598-4478 (Print) / ISSN 2233-7679 (Online)
†
Correspondence to: Sung Yoon Bae
Department of Management and Graduate School of Public Health, Inje University, #801, College of Medicine Building, 75, Bokji-ro, Busanjin-gu, Busan 614-735, Korea Tel: +82-51-890-8742, Fax: +82-51-894-6876, E-mail: [email protected]
Copyright © 2013 by the Korean Society of Dental Hygiene Science
Effects of Oral Health Knowledge and Practices on Decayed, Missing and Filled Teeth Index and Quality of Life -Path Analysis Using Structural Equation Modeling-
Young-Soo Lee, Sung Yoon Bae 1† and Jae-Hoon Ji 2
Department of Dental Surgery, Inje University Pusan Paik Hospital, Busan 614-735, 1 Department of Management and Graduate School of Public Health, Inje University, Busan 614-735, 2 Department of Medical Administration, Dong-Eui Institute of Technology, Busan 614-715, Korea
구강보건 지식과 실천이 우식경험치아와 삶의 질에 미치는 영향 -구조방정식을 이용한 경로분석을 중심으로-
이영수ㆍ배성윤
1†
ㆍ지재훈2
인제대학교 부산백병원 치과,
1인제대학교 경영학부 및 보건대학원,
2동의과학대학교 의무행정과
This study aims to measure oral health knowledge and practice level among dental clinic patients, and examine their relationships with decayed, missing and filled teeth (DMF) index and the oral health-related quality of life (QOL). Empirical data have been collected from 311 patients through structured questionnaires and dental examinations conducted in Busan area. According to the analysis of causal relationship, oral health knowledge turned out to have a direct effect on oral health practices, which exerted both direct and indirect effects on DMF index and oral health-related QOL.
While DMF index directly affected the oral health-related QOL, oral health knowledge proved to have only an indirect effect on DMF index and oral health-related QOL, mediated by oral health practices. Considering all these findings, effective oral health education and other intervention programs should focus on motivating people to participate in the active practices of desirable oral health behaviors, which will lead to the prevention of oral diseases and the subsequent improvement in the QOL.
Key Words: Decayed, missing and filled teeth index, Health Knowledge, Attitudes, Practice, Oral Health, Quality of Life
Introduction
As improved standard of living from the rapid eco- nomic growth and the advance of medical technologies have increased the public's life expectancy and the subsequent interest in the quality of life (QOL), many researchers and scientists in the healthcare sector are
paying more attention to the aspect of health-related QOL, not merely focusing on the aspect of physical health when they treat various diseases. Oral health problems are not exceptional from this trend, and more research topics of many scientists are increasingly centered around measu- ring the effect of oral health problems on the patients' daily functioning and their QOL.
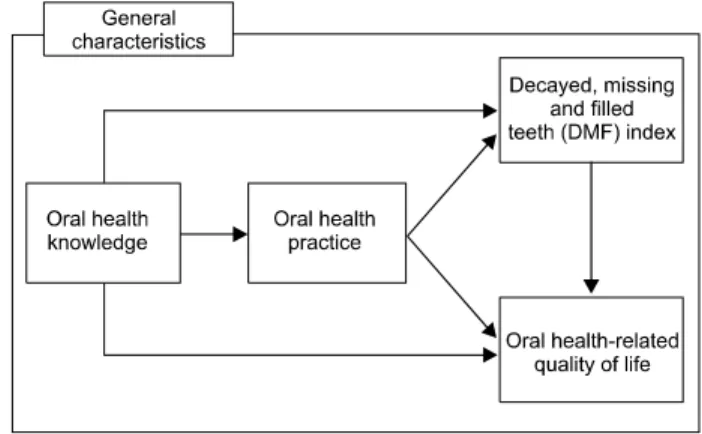
Fig. 1. Study model.
In a recent survey to the general public, however, the proportion of respondents who answered that the oral health was the most important factor among other health problems turned out to be higher in older populations
1)
. This result suggests that oral health is increasingly perceived indis- pensable for maintaining the QOL at a higher level.While most oral health problems are gradually progressed over the long period, many of them are rarely recovered to the previous conditions even after the successful treatment
2)
. In particular, ranked at the fourth most frequently treated outpatient health condition, dental caries is one of the major oral diseases in Korea3)
. While dental caries can be prevented or easily treated through early detection, it often remains untreated because it does not cause acute pain or discomfort in the early stage.Upon recognizing the importance of individual know- ledge and healthy practices to prevent dental caries, Korean public health authorities implemented various education programs. For example, public health centers developed oral health education programs for students and the population at risk, while launching public campaigns.
Many dental clinics also developed similar education programs for their patients.
But, the operational effectiveness of these health education programs in Korean population has not been well tested until recently. And few studies, if any, have provided adequate empirical data on the degree that oral health knowledge changes behaviors and that this behavioral change has positive effect on oral health condition and its related QOL. For example, many researchers, including Kim et al.
4)
, Jang et al.5)
, Song and Kim6)
, and Kim and Min7)
, studied oral health or its relation with QOL, but none of them related people's knowledge and practices to their effects on oral health- related QOL as well as clinical conditions such as decayed, missing and filled teeth (DMF) index in a comprehensive way.Therefore, this study is intended to measure oral health knowledge and practices among dental clinic patients, and relate them to both an important clinical indicator of oral health such as DMF index and the oral health-related QOL, believing that the successful identification of cau- sality among these factors will provide some insights for
the development of effective intervention programs for oral health improvement.
Materials and Methods
1. Study materials
Empirical data has been collected through a survey using self-administered, structured questionnaires given to 350 ambulatory patients who visited at the department of dentistry of a general hospital, a dental hospital and six dental clinics located in Busan area. The survey was conducted for one month, from March 16 through April 17, 2010 for the assessment of general characteristics of the survey respondents, their oral health knowledge and practices, and the oral health impact profile (OHIP-14). A total of 311 patients (89%) responded to the survey. In addition to the survey, oral examination has been conducted by eleven dentists to identify the number of decayed, missing and filled teeth. Dentists used a dental mirror and explorer to examine 28 permanent teeth except for third molars.
2. Study model
As depicted in Fig. 1, this study is intended to examine the relationship among knowledge, practices, DMF index and oral health-related QOL. Our study model was based on the theoretical models from Fishbein and Ajzen
8)
and Mitchell and Larson9)
, which tried to explain the conceptual relationship among perception, attitude and specific action.Variable Category Item Scale Reference Cronbach's
αOral health
knowledge
Fluoride & eating habits Toothbrushing
Dental hygiene products Dental caries
Periodontal disease & scaling Others
4 6 3 4 7 6
Yes (1 pts) No (0 pts)
Lee
10)Lee et al.
11)Paik
12)Lee
13)Chang and Song
14), Son
15)Gwon and Yang
16), Kim
17)0.738
Oral health practices
Fluoride & eating habits Toothbrushing
Dental hygiene products Dental caries
Periodontal disease & scaling Others
3 8 4 2 2 3
Likert 5-point Lee
10)Paik
12)Chang and Song
14)Son
15)Gwon and Yang
16), Kim
17)Cho and Choi
18)0.839
Oral health -related QOL
Limited functioning Physical pain
Psychological discomfort Reduced physical functioning Reduced psychological functioning Reduced social functioning Social disadvantage
2 2 2 2 2 2 2
Likert 5-point OHIP-14
Slade and Spencer
19)Slade
20)0.930
DMF index No. of decayed teeth No. of missing teeth No. of filled teeth
1 1 1
Observed number WHO recommendation
21)-
Others Gender, age, education, monthly household income, occupation, marital status, religion, smoking, oral health education, perceived oral- health status, interest in oral health
11 Various - -
Total 80
QOL: quality of life, DMF: decayed, missing and filled teeth.
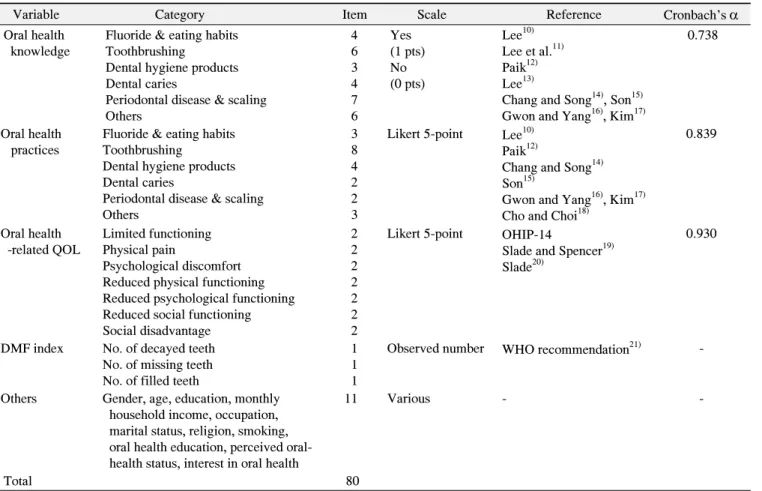
Table 1. Study Instruments and Questionnaires
Based on our study model, we have set and tested the following six hypotheses:
H1. If patients have higher level of oral health know- ledge, they will also have higher level of oral health practices.
H2. If patients have higher level of oral health knowledge, they will have lower level of DMF index.
H3. If patients have higher level of oral health knowledge, they will also have higher level of oral health-related QOL.
H4. If patients have higher level of oral health practices, they will have lower level of DMF index.
H5. If patients have higher level of oral health practices, they will also have higher level of oral health-related QOL.
H6. If patients have lower level of DMF index, they will have higher level of oral health-related QOL.
Further details on major instruments and other questionnaires will be discussed in the following section.
3. Instruments
Self-administered questionnaire was used to survey major responses, and they consisted of 77 items in four areas, which included oral health knowledge and prac- tices, oral health-related QOL, and general characteristics of the survey respondents (Table 1).
However, DMF index was calculated by eleven dentists, who used a dental mirror and explorer under the natural light aided by artificial lighting to examine 28 permanent teeth except for third molars. In specific, dentists followed the criteria recommended by the WHO to identify decayed teeth, missing teeth and filled teeth, and then they calculated DMF index by summing up all those three figures.
Five-point Likert scale was used to measure oral health practices of the survey respondents and their oral health-related QOL (OHIP-14), assigning one point when respondents “strongly disagreed” to each of the state-
Variable N (%) Gender
Male 115 (37.0)
Female 196 (63.0)
Age group
<20 21 (6.8)
20~29 146 (46.9)
30~39 72 (23.2)
40~49 38 (12.2)
50≤ 34 (10.9)
Education
High school or lower 86 (27.7)
2-year diploma holders 114 (36.7)
4-year college graduates 97 (31.2)
Postgraduates 14 (4.5)
Monthly household income (million KRW)
<2 73 (23.5)
2≤ and <3 85 (27.3)
3≤ and <4 62 (19.9)
4≤ and <5 39 (12.5)
5≤ 52 (16.7)
Marital status
Unmarried 190 (61.1)
Married 121 (38.9)
Religion
No 141 (45.3)
Yes 170 (54.7)
Occupation
Student 65 (20.9)
Homemaker 31 (10.0)
Professional 98 (31.5)
Technician 20 (6.4)
Service worker 19 (6.1)
Self-employer 16 (5.1)
Office worker 30 (9.6)
Unemployed 12 (3.9)
Others 20 (6.4)
Smoking
Yes 53 (17.0)
Never 236 (75.9)
Quitted 22 (7.1)
Oral health education received
Yes 99 (31.8)
Never 212 (68.2)
Perceived oral health status
Not healthy 108 (34.7)
Fair 147 (47.3)
Healthy 56 (18.0)
Interest in oral health
None 131 (42.1)
Low 71 (22.8)
High 109 (35.0)
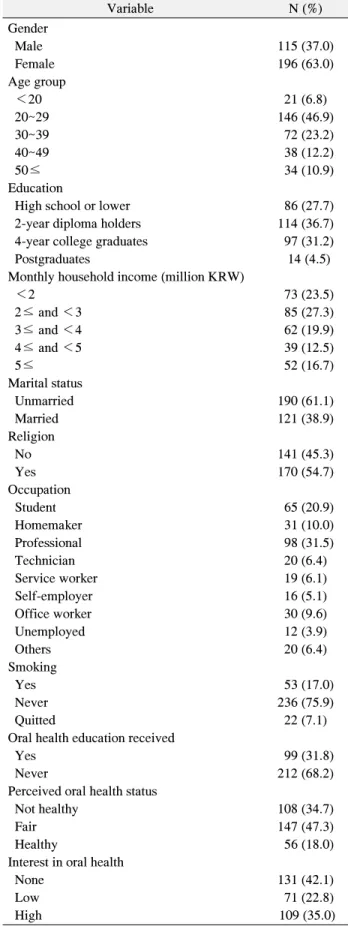
Table 2. General Characteristics of the Survey Respondents
ments, three-point for their “neutral” responses, and five- point when they “strongly agreed.”
Reliability for the instruments measuring oral health knowledge, oral health practices and oral health-related QOL has been tested with Cronbach's α value, which exceeded 0.7 in all three measurements. Instrument- specific Cronbach's α values were 0.738 for oral health knowledge, 0.839 for oral health practices, and 0.930 for oral health-related QOL, respectively.
Detailed information on the instruments and question- naires used in our study is summarized in Table 1.
4. Data analysis
IBM SPSS Amos ver. 18.0 (IBM Co., Armonk, NY, USA) as structural equation modeling tool and PASW Statistics ver. 18.0 (IBM Co., Armonk, NY, USA) were used for the analysis of data in our study. Specific methods of data analysis are as follows. First, General characteristics of the survey respondents were presented in frequencies and percentages. Second, reliability analysis was performed to test internal consistency of the instru- ments. Third, t-test and ANOVA test were used to analyze the variations of oral health knowledge and practices, DMF index, and oral health-related QOL by general characteristics of the survey respondents. Duncan’s test (multiple comparison test) was used to determine the significant differences between group means in an analysis of variance setting, and Pearson correlation analysis to examine the correlation among major va- riables. Fourth, path analysis was conducted to identify causality among knowledge, practices, DMF index and QOL, and to determine the mediating effect of two variables, oral health practices and the DMF index.
Results
1. General characteristics of survey respondents
General characteristics of a total of 311 survey respon- dents are presented in Table 2. Among survey respondents 63% was female, and twenties in their ages accounted for 46.9% of our study population. 36.7% and 31.5% of the respondents were two-year diploma holders and pro- fessionals, respectively. About one-third (27.3%) wasVariable Oral health knowledge Oral health practice DMF index Oral health- related QOL Gender
Male 17.99±4.15 3.00±0.51 7.21±5.43 3.95±0.78
Female 19.20±3.32 3.22±0.52 7.10±3.99 4.15±0.73
t (p) -2.660 (0.008) -3.642 (0.000) 0.184 (0.855) -2.219 (0.027)
Age group
<20 17.67±3.45 2.97±0.41 4.95±4.03 4.11±0.71
20~29 18.80±3.24 3.14±0.54 7.08±4.16 4.14±0.77
30~39 18.83±4.26 3.10±0.49 7.35±4.22 4.14±0.73
40~49 19.29±2.75 3.23±0.50 7.42±5.70 3.95±0.69
50≤ 18.44±5.08 3.18±0.61 8.00±5.60 3.79±0.81
F (p) 0.729 (0.573) 0.961 (0.429) 1.597 (0.175) 1.875 (0.115)
Education
High school or lower 17.56±4.43
a3.09±0.56
a6.81±4.89 4.04±0.72
2-year diploma holders 19.61±3.03
b,c3.20±0.52
a7.61±4.48 4.05±0.78
4-year college graduates 18.47±3.42
a,b3.05±0.48
a6.97±4.51 4.16±0.76
Postgraduates 21.00±2.86
c3.47±0.57
b6.57±3.65 3.87±0.73
F (p) 7.423 (0.000) 3.589 (0.014) 0.656 (0.580) 0.873 (0.456)
Monthly household income (million KRW)
<2 19.12±3.10 3.19±0.58 7.36±4.93 4.00±0.81
2≤ and <3 18.07±4.65 3.03±0.48 7.52±4.17 4.01±0.78
3≤ and <4 18.74±3.25 3.13±0.44 6.90±4.67 4.15±0.68
4≤ and <5 18.69±3.54 3.09±0.58 7.46±5.15 4.10±0.74
5≤ 19.40±3.21 3.27±0.55 6.27±4.09 4.19±0.74
F (p) 1.323 (0.261) 1.819 (0.125) 0.746 (0.561) 0.786 (0.535)
Marital status
Unmarried 18.56±3.39 3.12±0.52 6.79±4.21 4.13±0.75
Married 19.05±4.12 3.16±0.54 7.69±5.04 3.99±0.76
t (p) -1.134 (0.258) -0.527 (0.598) -1.683 (0.093) 1.630 (0.104)
Religion
No 18.57±3.68 3.15±0.55 6.93±4.36 4.10±0.78
Yes 18.90±3.70 3.12±0.51 7.32±4.74 4.05±0.74
t (p) -0.774 (0.440) 0.558 (0.577) -0.746 (0.456) 0.594 (0.553)
Occupation
Student 17.92±3.44
a,b2.99±0.44
a,b6.69±4.42 3.97±0.86
Homemaker 19.61±3.66
b,c3.21±0.59
b,c8.97±4.05 3.97±0.58
Professional 19.94±3.40
c3.27±0.53
c6.85±4.10 4.20±0.71
Technician 18.70±3.45
a,b,c2.95±0.51
a7.45±5.90 4.07±0.74
Service worker &
self-employer
17.29±4.20
a2.91±0.46
a6.40±4.17 3.90±0.80
Office worker 18.03±3.58
a,b3.24±0.50
b,c7.67±5.29 4.25±0.76
Unemployed & others 18.28±3.78
a,b,c3.22±0.58
b,c7.31±5.31 4.03±0.73
F (p) 3.925 (0.001) 4.120 (0.001) 1.247 (0.282) 1.385 (0.220)
Smoking
Yes 18.32±3.47 2.85±0.51
a8.91±5.48
a3.91±0.70
Never 18.93±3.71 3.20±0.52
b6.86±4.08
a4.10±0.77
Quitted 17.91±4.00 3.16±0.39
b5.91±6.05
b4.22±0.70
F (p) 1.206 (0.301) 10.122 (0.000) 5.349 (0.005) 1.784 (0.170)
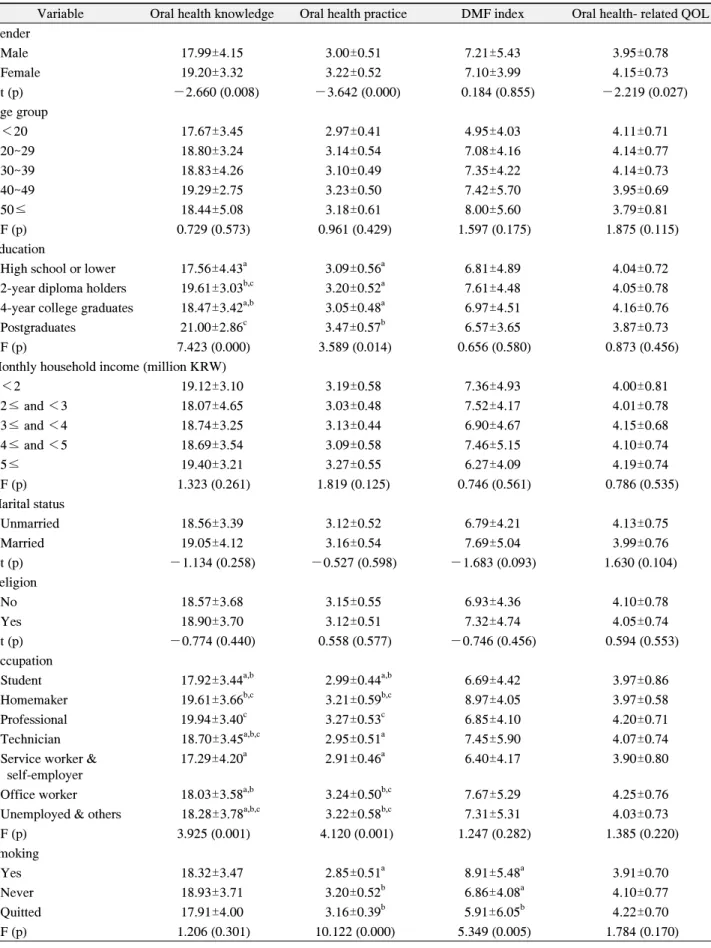
Table 3. Distribution of Major Responses by General Characteristics
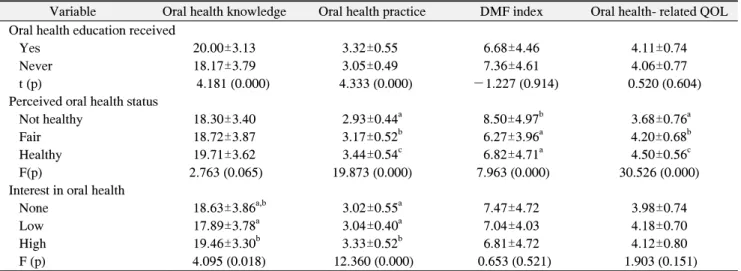
Variable Oral health knowledge Oral health practice DMF index Oral health- related QOL Oral health education received
Yes 20.00±3.13 3.32±0.55 6.68±4.46 4.11±0.74
Never 18.17±3.79 3.05±0.49 7.36±4.61 4.06±0.77
t (p) 4.181 (0.000) 4.333 (0.000) -1.227 (0.914) 0.520 (0.604)
Perceived oral health status
Not healthy 18.30±3.40 2.93±0.44
a8.50±4.97
b3.68±0.76
aFair 18.72±3.87 3.17±0.52
b6.27±3.96
a4.20±0.68
bHealthy 19.71±3.62 3.44±0.54
c6.82±4.71
a4.50±0.56
cF(p) 2.763 (0.065) 19.873 (0.000) 7.963 (0.000) 30.526 (0.000)
Interest in oral health
None 18.63±3.86
a,b3.02±0.55
a7.47±4.72 3.98±0.74
Low 17.89±3.78
a3.04±0.40
a7.04±4.03 4.18±0.70
High 19.46±3.30
b3.33±0.52
b6.81±4.72 4.12±0.80
F (p) 4.095 (0.018) 12.360 (0.000) 0.653 (0.521) 1.903 (0.151)
Values are presented as mean±SD.
DMF: decayed, missing and filled teeth, QOL: quality of life.
a~c
Values are significantly different using the Scheffe method.
Table 3. Continued
earning less than three million Korean won for their monthly household income. 61.1% was unmarried, and 45.3% had no religion. 75.9% of the respondents has never smoked while 68.2% of them has never received oral health education before. About half (47.3%) of the respondents answered ‘fair' to the question asking how they perceived their oral health status, but only 18% said that they were healthy. However, about one-third (35%) of respondents showed higher interest in their oral health, while 42.1% said that they had no interest in their oral health at all.
2. Distribution of major responses by general characteristics
Differences of oral health knowledge, practices, DMF index and oral health-related QOL by general character- istics of our survey respondents are shown in Table 3.
First, the level of oral health knowledge was signi- ficantly different by gender, education, occupation, exposure to oral health education programs, and interest in oral health. In specific, higher level of oral health knowledge was found among women, more educated people, those with higher interest in their oral health, and those who received oral health education. Per occupation, professionals showed the highest level of oral health knowledge while service workers and self-employers were
ranked the lowest. For specific differences of oral health knowledge between groups, refer to the results from Duncan’s test shown in Table 3.
Second, oral health practices were of significant difference by some general characteristics, which include gender, education, occupation, smoking, exposure to health education programs, perceived level of oral health status and interest in oral health. For example, higher level of oral health practices was prevalent among women, more educated patients, non-smokers, and those who received oral health education, who reported that they were healthy in terms of oral health, and who had higher interest in oral health. For specific differences of oral health practices between groups, also refer to the results from Duncan’s test shown in Table 3.
Third, the DMF index, an objective measurement for oral health condition, among our survey respondents showed statistical difference by smoking habits and perception on their oral health condition. According to the results from Duncan’s test, those who quitted smoking showed significantly lower level of DMF index, while those who had negative perception on their oral health had higher level of DMF index.
Fourth, oral health-related QOL of the sample popul- ation was statistically different depending on how they perceived their oral health: those who perceived their oral
Fig. 3. Modification model. DMF: decayed, missing and filled teeth, QOL: quality of life.
Fig. 2. Basic model. DMF: decayed, missing and filled teeth, QOL:
quality of life.
Variable Oral health knowledge
Oral health practice
DMF index Oral health
practices
0.361**
DMF index 0.010 -0.111
Oral health-
related QOL 0.043 0.151** -0.133*
DMF: decayed, missing and filled teeth, QOL: quality of life.
*p<0.05, **p<0.01.
Table 4. Correlation among Major Factors
health positively showed higher level of oral health-related QOL.
3. Correlation of major variables
As presented in Table 4, the correlation analysis revealed that our target variable, oral health-related QOL, proved to be positively correlated with oral health practices, but it had negative relationship with the number of DMF index, a presumably mediating variable in our study model.
4. Path analysis
Fig. 2 depicts our basic model to identify the presum- able causality among oral health knowledge and practices, DMF index, and oral health-related QOL, thereby exami- ning the mediating effect of oral health practices and DMF index on the relationship between oral health knowledge and oral health-related QOL.
In our basic model, the exogenous variable (oral health
knowledge) and the endogenous variable(oral health practices) are modeled as having both direct and indirect effects (through DMF index) on oral health-related QOL.
In most real model, the endogenous variables are also affected by factors outside the model (including measurement error). The effects of such extraneous variables are depicted by the “e” (or error terms) in the model as shown in both Fig. 2 and Fig. 3.
1) Goodness-of-fit analysis
Because the basic model is a saturation model, whose goodness-of-fit cannot be evaluated properly, we focused on the significant paths based on each of modification indices to induce the modification model (Fig. 3), on which then its goodness-of-fit was tested. To test the goodness-of-fit of our model, we conducted a path analysis using Amos 18.0 version.
The result of model fit analysis is summarized in Table 5, and based on the model fit indices we concluded that our model estimation reflects the study data adequately.
For example, one of absolute model fit indices, x² value 0.889 (degree of freedom=2, p=0.641), and most of other indices also satisfied general criteria for the model acceptance.
2) Analysis of causality
Path analysis is used to describe the directed depen- dencies among a set of variables. Through this structural equation modeling, we examined causal relationships bet- ween major factors, calculating the path coefficients for
Direction of causality Estimate SE CR p Oral health practices
DMF index
Oral health-related QOL Oral health-related QOL
←
←
←
←
Oral health knowledge Oral health practices Oral health practices DMF index
0.361
-0.111 0.138
-0.117
0.008 0.49
0.081 0.009
6.795
-1.958 2.449
-2.083
0.000 0.049 0.014 0.037 SE: standard error, CR: critical ratio, DMF: decayed, missing and filled teeth, QOL: quality of life.
Table 6. Causal Relationships between a Set of Factors
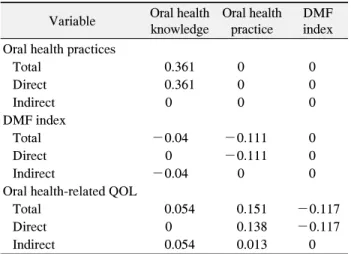
Variable Oral health knowledge
Oral health practice
DMF index Oral health practices
Total 0.361 0 0
Direct 0.361 0 0
Indirect 0 0 0
DMF index
Total -0.04 -0.111 0
Direct 0 -0.111 0
Indirect -0.04 0 0
Oral health-related QOL
Total 0.054 0.151 -0.117
Direct 0 0.138 -0.117
Indirect 0.054 0.013 0
DMF: decayed, missing and filled teeth, QOL: quality of life.
Table 7. Decomposed Effect of Each Variable
p d.f. x² RMR GFI AGFI NFI RFI IFI TLI CFI
0.641 2 0.889 0.264 0.999 0.993 0.985 0.955 1.019 1.063 1
d.f.: degree of freedom, RMR: root mean-squared residual, GFI: goodness of fit index, AGFI: adjusted GFI, NFI: normed fit index, RFI:
relative fit index, IFI: incremental fit index, TLI: Turker-Lewis index, CFI: comparative fit index.
Table 5. Modification Model Fit Index
each set of variables (Table 6).
According to the results of our analysis, oral health knowledge had significant influence on oral health practices in a positive way (p<0.001), which had a negative effect on the DMF index while having a positive effect on oral health-related QOL. The DMF index, however, exerted negative influence on oral health-related QOL.
3) Decomposing the effects of each factor
Table 7 reveals the decomposed effect of each variable, labeled as either direct or indirect. Oral health knowledge turned out to have a direct effect on oral health practices while having only an indirect effect on DMF index and oral health-related QOL. Oral health practices had a direct effect on DMF index, but they had both direct and indirect
effects on oral health-related QOL. DMF index, however, had only a direct effect on oral health-related QOL.
Discussion
As more scientists and researchers have increasingly focused on health and its impact on the QOL, oral health-related QOL also received more attention from them, and the public's recognition of the importance of oral health provoked the burst of education programs and other interventions, both public and private. Despite all these recent efforts, still we don't have solid empirical data on the degree that oral health knowledge changes behaviors and how much effect these behaviors or oral health practices have on oral health conditions and the QOL.
Therefore, we tried to hypothesize and evaluate the causal relationships among knowledge, practices, health problems, and the QOL in the area of oral health, providing with the reliable reference data which would contribute to the development of effective oral health education programs and further interventions. We tested our hypotheses with the empirical data collected from 311 ambulatory patients who visited at the department of dentistry of a general hospital, a dental hospital, and six dental clinics located in Busan area. Major findings are discussed below.
In regard to the distribution of responses to major variables by general characteristics of our study popula- tion, significantly higher level of oral health knowledge
was found among women, professionals, more educated people, those who received oral health education, and those with higher interest in their oral health. Similar responses were observed for oral health practices, except that its higher level was also prevalent among non- smokers and those who reported that they were healthy in terms of oral health. These results are consistent with those from previous studies. For example, higher level of oral health knowledge and practices was found among women in the study conducted by Lee
13)
, among more educated people in the research conducted by Chang and Song14)
, and among those who received oral health education in Son’s study15)
. It is not surprising that the higher level of oral health knowledge and practices was found among those who reported that they were healthy in terms of oral health and those who had higher interest in their oral health.However, the higher level of DMF index was observed among smokers and those who reported that they were not healthy in terms of oral health in our study. Higher level of DMF index can be partly attributed to the fact that smoking is reportedly correlated with the alveolar bone defects and tooth loss
22,23)
. Presumably most of those who received periodontal treatment are smokers in our study population. This result suggests that smoking cessation program could be a part of important interventions to enhance oral health. It is natural that the higher level of DMF index was observed among those who answered that they were not healthy because most people would perceive that they were unhealthy if they had subjective symptoms due to their oral diseases18)
. In our study, higher level of oral health- related QOL was found among women and those who had positive perception on their oral health, which is consistent with the results from previous studies4,7)
.Results from the path analysis for major variables of our interest can be summarized in four parts as follows.
First, oral health knowledge turned out to have a direct effect on oral health practices in a positive way, which is consistent with the results from previous studies reporting positive relationship between two variables
14,24)
. This implies that oral health knowledge, if provided properly and adequately through effective oral health education,could guide desirable changes in oral health practices.
Second, oral health practices had a direct but negative effect on the DMF index in our study. In other words, the level of DMF index decreased as the level of oral health practices increased. Similar results are also found in some previous researches, each of which focused on different populations. For example, Oliveira et al.
25)
found in their study that the lower level of oral health knowledge and preventive practices were significantly correlated with poor oral health conditions and higher incidence of dental caries among the third grade school children. Gwon and Yang16)
reported that the elderly showing higher level of oral health behaviors had lower level of DMF index. This suggests that the effective education program should help people understand the importance of preventive practices for their oral health, not merely providing oral health knowledge, but it should be designed around motivating them to make actual changes of their behaviors in a desirable way.Third, our study result shows that oral health practices had a positive effect on oral health-related QOL, both directly and indirectly, which is consistent with the result of a previous study conducted by Kim and Min
7)
. What can be implied from this direct effect of oral health practices on the DMF index and oral health-related QOL is that the active practices of desirable health behaviors could contribute to the improvement of oral health-related QOL in the end.Fourth, the DMF index proved to exert a direct effect on oral health-related QOL in our study, and similar results have also been found in the previous researches. For example, Kushnir et al.
26)
reported that many oral health conditions were correlated with the oral health- related QOL, and Robinson et al.27)
found in their study that the higher incidence of dental caries decreased the level of oral health-related QOL through deteriorating tooth function. In fact, dental caries, if left untreated, would lead to tooth loss, which in turn allows undesirable migration of other teeth, and in the end can cause the subsequent oral health problems such as malocclusion and temporo- mandibular joint disorder. Therefore, it is essential to maintain healthy oral health conditions for improving oral health-related QOL.In summary, our study results showed that all of oral health knowledge, preventive oral health practices and oral health problems affected the oral health-related QOL, either directly or indirectly. In particular, the significant importance of oral health practice should not be ignored because it has both direct and indirect effects on oral health-related QOL. It is necessary that the development of effective oral health education and other intervention programs focus on how to help people understand the importance of preventive practices and motivate them to participate in the active practices of desirable oral health behaviors so that all these efforts can lead to the pre- vention of oral diseases and the subsequent improvement in the QOL.
Finally, despite all our efforts to provide scientifically robust data, our research had a few inevitable challenges, disclosure of which we believe will guide the future researches on this subject.
First, interpretation of our study results to the general population should be done cautiously because our study sample is small and includes disproportionately higher percentage of younger population. Reliability of our study results could be validated through further researches for more representative population with larger sample size.
Second, our study model might not be comprehensive.
For example, oral health-related QOL could be influenced by factors other than we considered in our study. More comprehensive study design and multi-faceted analysis would be helpful to identify other factors and understand the better picture of their relationships with oral health and the QOL.
Summary
This study was intended to identify the level of oral health knowledge, preventive practices and DMF index as one of important indicators of poor oral health conditions, and to determine their effects on the oral health-related QOL. For this study, structural questionnaires were distributed to 311 patients who visited at dental hospitals or dental clinics located in Busan area, and their oral health conditions have been examined by eleven dentists to calculate the DMF index. Major findings of our study
can be summarized as follows.
First, significantly higher level of oral health knowledge was found among women, professionals, more educated people, those who received oral health education, and those with higher interest in their oral health. Similar responses were observed for oral health practices, except that its higher level was also found among non-smokers and those who reported that their oral conditions were healthy. The level of DMF index was higher among smokers and those who reported that their oral conditions were unhealthy. However, higher level of oral health-related QOL was prevalent among women and those who had positive perception on their oral health.
Second, according to the analysis of causal relationship among major factors, oral health knowledge turned out to have a direct effect on oral health practices, which exerted both direct and indirect effects on the DMF index and oral health-related QOL. While DMF index directly affected the oral health-related QOL, oral health knowledge proved to have only an indirect effect on DMF index and oral health-related QOL, mediated by oral health practices.
Considering all these research findings, it is essential that the effective oral health education and other intervention programs should be developed, focusing on how to help people understand the importance of prevention, and invite them to the active practices of desirable oral health behaviors. All those efforts, at both individual and population levels, can lead to the prevention and timely treatment of oral diseases, and the subsequent improvement of the QOL in the end.
요 약
삶의 질에 대한 관심이 증가함에 따라 건강과 관련된 삶 의 질 향상에 대한 관심도 증가하고 있다. 구강건강의 관점 에서도 구강질환이 삶의 질을 저하시키며, 구강질환의 예방 이 삶의 질을 향상시킨다. 본 연구에서는 구강보건지식과 구강보건실천 정도, 구강건강상태, 그리고 구강건강 관련 삶의 질의 관계를 알아보고자 하였다.
부산지역에 소재한 종합병원 치과, 치과병원 및 치과의원 에 내원한 환자 311명을 대상으로 2010년 3월 16일부터 한 달간 구조화된 자기기입식 설문지를 사용하여 대상자의 일 반적 특징 및 구강보건지식, 구강보건실천, 구강건강관련
삶의 질(OHIP-14) 등에 대한 자료를 수집하였으며, 치과의 사 11명이 치경과 탐침으로 사랑니를 제외한 28개의 치아를 대상으로 우식경험치아수(DMF index)를 확인하였다.
분석결과, 구강보건지식은 구강보건실천에, 구강보건실 천은 우식경험치아수와 구강건강관련 삶의 질에 직접적인 영향을 미치는 것으로 나타났고, 우식경험치아수도 구강건 강관련 삶의 질에 유의한 변수임을 알 수 있었다. 그러나 구 강보건지식은 우식경험치아수와 구강건강관련 삶의 질에 직접적인 영향요인이 아니라, 구강보건실천의 매개를 통해 간접적으로 영향을 미치는 것으로 나타났다.
이러한 연구결과는 구강건강관련 삶의 질을 높이기 위해 서는 직접적인 효과를 가지고 있는 구강보건실천 수준과 우 식경험영구치아수를 적절히 관리할 수 있도록 하는 방안마 련이 절실히 요구됨을 말해주고 있다. 즉 우식경험치아수는 구강보건실천에 직접적으로 영향을 받는 변수이므로 단순 히 구강건강관련 지식만을 전달하기보다는 태도의 변화와 실천 행동을 유도할 수 있는 구강보건교육 프로그램을 개발 함으로써 구강질환의 예방과 조기치료로 이어지도록 해야 할 것이다.