INTRODUCTION
Long head of biceps brachii (LHBB) is an anatomical site in which a lot of anatomical variants exist the most common being a third head LHBB. Conversely, an extra
articular origin of LHBB has rarely been reported [1-5].
The clinical importance or relevance of these variants are yet unclear [1-4]. Thus, without more knowledge of these anatomical variants it is difficult to accurately diagnose lesions of the biceps through magnetic resonance imaging (MRI) [5]. We found and treated a case of an extraarticular origin of the LHBB that was attached firmly to the rotator cuff with laminated tear.
CASE REPORT
A 57yearold woman presented with spontaneous pain and weakness in the left shoulder 8 months prior to the hospital visit. The symptoms aggravated 3 weeks prior to the visit when she fell on her left hand. Physical examination showed tenderness on the lateral aspect and on the bicipital groove of the shoulder joint. Range of passive motion was normal, whereas, active flexion and
abduction motions were decreased from normal. The patient showed positive scores for the Neer’s impingement test, Hawkin’s impingement test, empty can test, and full can test, and negative scores for the Speed test, Yergason test, and instability test.
Simple Xray films showed no abnormal findings;
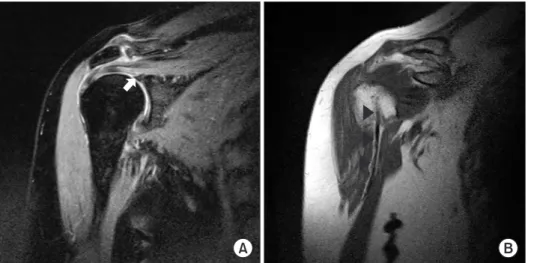
therefore further radiological checks were made through MRI. MRI revealed a 20 × 19 mm sized full thickness rotator cuff tear that crossed from the rotator interval to the infraspinatus tendon including the supraspinatus tendon. The LHBB could be traced along the bicipital groove, but not in the intraarticular area. The origin of the LHBB was absent on the superior labrum (Fig. 1).
The patient was diagnosed with a full thickness rotator cuff tear. During the arthroscopic operation, we found that the glenohumeral joint com municated into the subacromial space through a large rotator cuff tear. The torn rotator cuff was laminated and the upper tissue of the laminated rotator cuff was retracted more medially than the lower tissue. We found that the LHBB did not originate from the superior labrum but panned out at its end to merge with the inferior aspect of the lower tissue of the torn supraspinatus tendon, which was assumed The long head of biceps brachii contributes to the stability of glenohumeral joints. Its pathologic changes can cause pain in the shoulders independent of or in combination with other structures. Various anatomical variations of the long head of biceps brachii have been reported, but an extraarticular origin of the long head of biceps brachii has rarely been reported. Here, we report a case of an extraarticular origin of the long head of biceps brachii that was firmly attached to the rotator cuff.
Keywords: Shoulder; Long head of biceps brachii; Anatomic variant; Arthroscopy
Extra-articular origin of long head of biceps brachii that is attached to the rotator cuff
Woo-Jin Yi, Jin-Hyoung Son
Department of Orthopaedic Surgery, Seoul Red-Cross Hospital, Seoul, Korea
Copyright © 2014 Korean Arthroscopy Society and Korean Orthopedic Society for Sports Medicine. All rights reserved.
CC This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/3.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received January 16, 2014; Revised February 18, 2014; Accepted February 26, 2014
Correspondence to: Woo-Jin Yi , Department of Orthopaedic Surgery, Seoul Red-Cross Hospital, 9 Saemunan-ro, Jongno-gu, Seoul 110-747, Korea. Tel: +82-2-2002-8390, Fax: +82-2-2002-8398, E-mail: [email protected]
Arthroscopy and Orthopedic Sports Medicine
AOSM
to be the capsule. The attachment of the LHBB to the lower tissue of the torn rotator cuff was so firm that the torn rotator cuff moved together with the LHBB when the
LHBB glided. There was no pathologic abnormality on the superior labrum except for the absence of the origin of LHBB (Figs. 2, 3).
We performed acromioplasty and then tenodesis of the LHBB to the upper end of the bicipital groove. Lastly, we repaired the lower tissue of the rotator cuff on the footprint just lateral to the articular surface, and then repaired the upper tissue on the lateral area of the repaired lower tissue using a double row suture bridge technique.
DISCUSSION
The LHBB has many kinds of anatomical variants, but the attachment between LHBB and the rotator cuff is not commonly encountered in daily practice. Normally, the LHBB originates from the posterior part of the superior labrum and the supraglenoid tubercle. From its origin, it travels to the intraarticular space over the humeral head, passes out of the joint capsule, and runs down along the bicipital groove.
Fig. 2. (A) The arthroscopic view from the posterior portal shows the upper tissue (arrows) and the lower tissue (arrowheads) of laminated rotator cuff tear that is firmly attached to the long head of biceps brachii (LHBB). (B) When the LHBB is pushed down, the panning out of the LHBB is clearly seen. The lateral margin of the lower tissue of the rotator cuff (arrowheads) can be distinguished from the LHBB.
Fig. 3. The arthroscopic view from posterior portal shows the non
intraarticular origin of the long head of biceps brachii on the superior labrum (arrow). SSc, subscapularis tendon; G, glenoid surface.
Fig. 1. (A) A oblique coronal view of a pre
operative magnetic resonance imaging (MRI) shows a full thickness rotator cuff tear (black arrow). And an absence of the long head of biceps brachii (LHBB) in the intraarticular space and in the superior labrum (white arrow). (B) Another oblique coronal view of a preoperative MRI shows a normal intact LHBB (arrowheads) in the bicipital groove.
Functionally, the LHBB contributes to the stability of shoulder joints. Clinically, the pathologic changes in LHBB may cause pain with or without collateral patho
logic changes in other structures. Further, during an arthroscopic operation, understanding the anatomical structure and anatomic variants of LHBB may aid surgeons to distinguish between an actual pathology and a rare anatomical property. Thus, the need for a set of standards to differentiate between pathologic changes and anatomic variants of the LHBBs is very important [4,6,7].
Although some investigators suggest that LHBB does not have any specific function in shoulder joints, it is generally accepted that LHBB contributes to the stability of the glenohumeral joint by pushing down the humeral head and placing it on the glenoid surface [4,6,8,9]. In fact, many investigators emphasize the correlation between LHBB and anterior instability. Based on the studies that anterior instabilities are commonly found in the patients with LHBB variants, and other studies that electrical activities of the LHBs on electromyography tests are increased in the pitchers with anterior instabilities.
Numerous anatomic variants of LHBBs have been previously reported. Two seminal studies have syste
matically classified intraarticular variants of LHBBs by reviewing many cases. Dierickx et al. [1] classified variants of the intraarticular LHBBs into 4 major families and into 12 subgroups by analyzing 3,000 arthroscopic findings from retrospective reviews. Kanatli et al. [7] classified variants of intraarticular LHBBs into 7 types by analyzing 671 arthroscopic findings.
But with regard to our case, the classification of Kanatli et al. [7] suggests only one type, the complete synovial tunnel, for the cases that LHBBs are not observed in the
intraarticular spaces. Therefore, it doesn’t include absence of the LHBB or the extraarticular origin from joint capsule or rotator cuff as in our case. The classification of Dierickx et al. [1] does not differentiate the extraarticular origin of LHBB, originating from the joint capsule or rotator cuff, from the complete synovial tunnel, which is described by Kanatli et al. [7] and reported by Hammond and Bryant [10].
The characteristic of synovila tunnel making distinction from our case is that a pristine LHBB of the intraarticular space is completely encased by a a synovial envelope, and thus it is not the true BARC (biceps adhesion to the rotator cuff) complex. So taking this distinction into con
sideration, we reviewed the cases where the LHBBs did not originate from the superior labrums or supraglenoid tubercles and were not observed in the intraarticular spaces, and then classified them using the classification of Dierickx et al. [1]. In order to exclude complete synovial tunnel, we included only the cases in which the firm attachments of LHBB to the rotator cuffs were identified.
According to our literature review, 5 cases of ADH
CO (completely attached to the supraspinatus, but not attached to the labrum) were reported [1-5], and in these, 2 cases were identified as having a firm attachment to the rotator cuff [1,4]. The other 2 cases were excluded because there was no clear evidence of a firm attachment to the rotator cuff and therefore, possibilities of complete synovial tunnel existed [2,5]. Whereas in the last case, the LHBB were tapered and merged to the rotator interval [3].
Our case is quite similar to the ADHCO case reported by Dierickx et al. [1], except for the laminated appearance of the rotator cuff tear. The above two cases can be thought to be caused by the secondary adhesion of LHBB to the
Fig. 4. (A) The oblique coronal view of magnetic resonance imaging of the non
symptomatic right shoulder shows a nonlabral origin (white arrow) and non
intraarticular origin of the long head of biceps brachii (LHBB). (B) The extra
articular portion of the LHBB of the non
symptomatic right shoulder is identified.
An intact rotator cuff (arrowheads) can be seen.
rotator cuff after both are torn. However, the likelihood of this seems to be low in our case for three reasons.
First, the remaining portion of LHBB appears completely normal without any inflammatory changes or adhesion to other tissues. Second, the LHBB pans out at its end and smoothly merges with the joint capsule and rotator cuff (Fig. 2B). Lastly, the MRI of the nonsymptomatic contralateral shoulder of the same patient also shows absence of an intraarticular portion of the LHBB but an intact rotator cuff (Fig. 4).
In laminated rotator cuff tears, the lower tissues are usually retracted more medially than the upper tissues, but in our case, the lower tissue was unusually retracted less medially than the upper tissue. This unusual retraction of the lower tissue may have come under constrain by the tension from strong attachment with the LHBB.
During embryonic development, the LHBB is formed from the mesoderm of the arm bud at around the 7th or 8th week [6]. In the past, the LHBB was thought to first develop in the extraarticular, extracapsular space and then migrate into the intraarticular space. But now the site of development and occurrence of the transmigration is under dispute [1,7]. Audenaert et al. [11] proposed that the LHBB develops between the fibrous capsule and synovial layer, and the staged migration occurs into intraarticular position. Egea et al. [3] and Parikh et al. [9]
proposed that this migration may be interrupted, and this may explain the variations in LHBB. But histological findings by Yeh et al. [12] in their case showed that the tendon fibers dispersed and mixed with the connective tissue of the superior joint capsule after it merged with the capsule, and they stated that the incomplete differentiation of the LHBB and the rotator cuff can explain these variants, a hypothesis to which Gaskin et al.
[5] agreed.
Although the variations of LHBBs have been thought to have no relations with pathology, a lot of opinions have been suggested that the possibility of the shoulder instability increases when accompanied with the variation of LHBB [2,3,5]. The relation with the rotator cuff tear was also suggested [1,3,7]. Dierickx et al. [1] believe that the rotator cuff tears can be induced by a complete adherence or a solid fusion between the rotator cuff and the LHBB. Egea et al. [3] suggested a correlation between a rotator cuff tear and an absence of the LHBB in the intra
articular space. In agreement to these previous findings, our case of abnormal LHBB was also accompanied with a full thickness rotator cuff tear. We believe the rotator cuff tear may have been caused by the stress on the rotator cuff insertion during biceps contraction because of its firm attachment to the biceps tendons. But further investigation is required to prove this assumption.
As variants of intraarticular LHBBs are difficult to diagnose accurately with MRI or other examinations, it is easy to misinterpret them as pathologic changes.
Therefore, increasing the knowledge and awareness of the variants of LHBBs is a way to improve the rate of accurate interpretations at preoperative examinations. This will help avoid unnecessary operations and decrease the possibility of treatment failures. In an effort to contribute to this, we report a case of an extraarticular origin of a LHBB firmly attached to the rotator cuff that has a laminated tear.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
1. Dierickx C, Ceccarelli E, Conti M, Vanlommel J, Castagna A.
Variations of the intra-articular portion of the long head of the biceps tendon: a classification of embryologically explained variations. J Shoulder Elbow Surg 2009;18:556-65.
2. Hyman JL, Warren RF. Extra-articular origin of biceps brachii.
Arthroscopy 2001;17:E29.
3. Egea JM, Melguizo C, Prados J, Aránega A. Capsular origin of the long head of the biceps brachii tendon: a clinical case. Rom J Morphol Embryol 2010;51:375-7.
4. Cheema P, Singla R. Extra-articular origin of long head of biceps brachii in human cadaver: a case report. J Morphol Sci
2010;27:157-9.
5. Gaskin CM, Golish SR, Blount KJ, Diduch DR. Anomalies of the long head of the biceps brachii tendon: clinical significance, MR arthrographic findings, and arthroscopic correlation in two patients. Skeletal Radiol 2007;36:785-9.
6. Ghalayini SR, Board TN, Srinivasan MS. Anatomic variations in the long head of biceps: contribution to shoulder dysfunction.
Arthroscopy 2007;23:1012-8.
7. Kanatli U, Ozturk BY, Esen E, Bolukbasi S. Intra-articular variations of the long head of the biceps tendon. Knee Surg Sports Traumatol Arthrosc 2011;19:1576-81.
REFERENCES
8. Richards DP, Schwartz M. Anomalous intraarticular origin of the long head of biceps brachii. Clin J Sport Med 2003;13:122-4.
9. Parikh SN, Bonnaig N, Zbojniewicz A. Intracapsular origin of the long head of the biceps tendon with glenoid avulsion of the glenohumeral ligaments. Orthopedics 2011;34:e781-4.
10. Hammond JE, Bryant B. Biceps adhesion to the rotator cuff: a case report. Am J Sports Med 2013;41:302-5.
11. Audenaert EA, Barbaix EJ, Van Hoonacker P, Berghs BM.
Extraarticular variants of the long head of the biceps brachii:
a reminder of embryology. J Shoulder Elbow Surg 2008;17(1 Suppl):114S-7S.
12. Yeh L, Pedowitz R, Kwak S, et al. Intracapsular origin of the long head of the biceps tendon. Skeletal Radiol 1999;28:178-81.