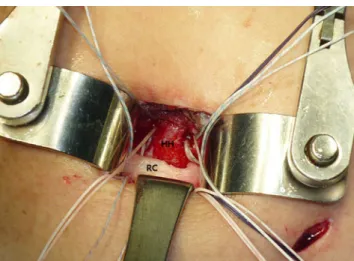
Anterolateral approach for mini-open rotator cuff repair
6
0
0
전체 글
(2)
(3)
(4)
(5)
(6)
수치

관련 문서
• Defenders need visibility into process and file telemetry, command line parameters, and Windows Event logs. • Subscribe to ETW logs to collect PowerShell cmdlets and
CFS = Container freight station where containers are stuffed and unstuffed MT Depot = area for storing empty containers. M&R = maintenance and repair of containers
“With the MySQL Query Analyzer, we were able to identify and analyze problematic SQL code, and triple our database performance. More importantly, we were able to accomplish
In this study, therefore, the method for measuring residual stresses using ESPI technique that is one of the laser applied measurement technique excellent in the view
In this study we will survey the changes in DNA repair factors during aging in rat, including mismatch repair (MMR), base excision repair (BER), and double-strand break
Evaluation of prevalance and clinical impact for unknown origin hypereosinophilia patients.. By
We have already looked at this problem from one standpoint for which we found the value of the potential was doubled at the surface and the expression for the
Conclusion: In Neer type II distal clavicle fracture treatment, both groups showed satisfactory result in clinical and radiological outcomes, but the hook plate
