저작자표시-비영리 2.0 대한민국 이용자는 아래의 조건을 따르는 경우에 한하여 자유롭게 l 이 저작물을 복제, 배포, 전송, 전시, 공연 및 방송할 수 있습니다. l 이차적 저작물을 작성할 수 있습니다. 다음과 같은 조건을 따라야 합니다: l 귀하는, 이 저작물의 재이용이나 배포의 경우, 이 저작물에 적용된 이용허락조건 을 명확하게 나타내어야 합니다. l 저작권자로부터 별도의 허가를 받으면 이러한 조건들은 적용되지 않습니다. 저작권법에 따른 이용자의 권리는 위의 내용에 의하여 영향을 받지 않습니다. 이것은 이용허락규약(Legal Code)을 이해하기 쉽게 요약한 것입니다. Disclaimer 저작자표시. 귀하는 원저작자를 표시하여야 합니다. 비영리. 귀하는 이 저작물을 영리 목적으로 이용할 수 없습니다.
Clinical outcome and Predictive factors of
Coronary aneurysm
after Percutaneous Coronary Intervention
by
Eun-Jin Han
Major in Medicine
Department of Medical Sciences
The Graduate School, Ajou University
Clinical outcome and Predictive factors of
Coronary aneurysm
after Percutaneous Coronary Intervention
by
Eun-Jin Han
A Dissertation Submitted to The Graduate School of
Ajou University in Partial Fulfillment of the Requirements
for the Degree of
Master of Medicine
Supervised by
Seung-Jea Tahk, M.D., Ph.D.
Major in Medicine
Department of Medical Sciences
The Graduate School, Ajou University
This certifies that the dissertation
of Eun-Jin Han is approved.
SUPERVISORY COMMITTEE
Seung-Jea Tahk
Joon-Han Shin
Byoung-Joo Choi
The Graduate School, Ajou University
December, 20th, 2011
i -ABSTRACT-
Clinical Outcome and Predictive Factors of Coronary Aneurysm
After Percutaneous Coronary Intervention
Coronary artery aneurysms (CAAs) defined as angiographic luminal dilatation (50% larger than the adjacent reference vessel) at the site of stent implantation are rare and the reported incidence varies from 0.3% to 6%(Aoki et al., 2008). A new term, peri-stent contrast staining (PSS) was defined as contrast staining outside the stent contour extending to ≥20% of the stent diameter which do not fulfill the classic definition of CAAs by a Japanese group (Imai et al., 2011). It is controversial that these abnormal angiographic findings may be related with adverse clinical events because recent DES registry data showed CAAs took mostly favorable clinical courses with continuous dual-antiplatelet therapy (Ahn et al., 2010) although poor clinical outcomes including in-stent restenosis and stent thrombosis after drug-eluting stent (DES) implantation were increased with CAAs after DES implantation (James et al., 2009).
In this study to assess the clinical outcome of CAAs and PSS after percutaneous coronary intervention (PCI) under the realworld practice, the patients with CAA or PSSs were younger and non-diabetic undergoing PCI with longer DES implantation, especially Sirolimus eluting stent. Poor clinical outcomes including in-stent restenosis and targel lesion revascularization were increased in the patients with CAA/PSS than without CAA/PSS but there was no difference of cardiovascular and all-cause mortality. In the subgroup analysis,
ii
there are no events of cardiac death but stent thrombosis and myocardial infarction were developed more frequently in CAA group compared with PSS group.
Keywords: coronary aneurysm, peri-stent contrast staining, clinical outcome, predictive
iii
TABLE OF CONTENTS
ABSTRACT ··· i
TABLE OF CONTENTS ··· iii
LIST OF FIGURES ··· v LIST OF TABLES ··· vi ABBREVIATION ··· vii I. INTRODUCTION ··· 1 II. METHODS ··· 2 A. Study population ---2 B. Intervention procedures ---2 C. Angiographic analysis ---2 D. Definition ---3 E. Statistical analysis ---3 III. RESULTS ··· 4
A. Occurrence of CAA/PSS after PCI ---4
B. Angiographic findings ---5
C. Risk Factors of CAAs & PSS ---8
D. Clinical Sequelae : CAA/PSS group versus non-CAA/PSS group ---9
E. Clinical outcome : CAA group versus PSS group ---10
IV. DISCUSSION ··· 12
V. CONCLUSION ··· 16
iv
v
LIST OF FIGURES
vi
LIST OF TABLES
Table 1. Baseline clinical characteristics between patients with and without CAAs or PSS
··· 4
Table 2. Angiographic characteristics between patients with and without CAAs or PSS ··· 6
Table 3. Risk factors of CAA and PSS ··· 8
Table 4. Clinical coutcome : CAA/PSS vs. non-CAA/PSS group ··· 9
vii
ABBREVIATION
PCI : Percutaneous coronary intervention CAA: Coronary artery aneurysm
PSS: Peri-stent contrast staining DES: Drug-eluting stent
- 1 -
I.
INTRODUCTION
Coronary artery aneurysms (CAAs) defined as angiographic luminal dilatation (50% larger than the adjacent reference vessel) at the site of stent implantation are rare and the reported incidence varies from 0.3% to 6% (Aoki et al., 2008). A new term, peri-stent contrast staining (PSS) was defined as contrast staining outside the stent contour extending to ≥20% of the stent diameter which do not fulfill the classic definition of CAAs by a Japanese group (Imai et al., 2011). There are growing concerns that these abnormal angiographic findings may be related with adverse clinical events such as in-stent restenosis and stent thrombosis after drug-eluting stent (DES) implantation (James et al., 2009). Although some reported that CAAs after DES implantation showed mostly favorable clinical course, it still remains to be uncertain if the poorer outcomes is not related with CAAs or PSS after percutaneous coronary intervention (PCI) under real world practice. (Ahn et al., 2010). There are also insufficient data which factors contribute to the development and progression of CAAs and PSS. The aim of the present study was to assess the clinical outcome and predictive factors for occurrence of coronary aneurysm and peri-stent contrast staining.
- 2 -
II.
METHODS
A. Study population
From the registry data of the single cardiovascular center, Ajou university hospital (Suwon, South Korea), 7355 patients with percutaneous coronary intervention (including drug-eluting or bare metal stent implantation) between January 2003 and December 2010 were identified. Among them, 2567 patients with 5,158 lesions with follow-up coronary angiography after index PCI were recruited in this retrospective, observational study. All patients were advised to maintain dual antiplatelet therapy including lifelong use of aspirin (at least 100mg daily) unless contraindicated. Seventy-eight CAAs or PSSs in 54 patients were detected at late angiography, and the clinical and angiographic data were compared between patients with and without CAA or PSS.
B. Intervention procedures
Eligibility criteria for PCI included coronary artery with ≥ 75% stenosis. These procedures were performed according to current standard guidelines.
C. Angiographic analysis
In quantitative coronary angiography, mean reference vessel diameter, minimal luminal diameter, lesion length, percentage of diameter stenosis, and late luminal loss were analyzed using the computer-assisted automated edge detection method.
- 3 -
D. Definitions
According to coronary angiographic morphologies, coronary artery aneurysm (CAA) was defined as a localized or diffuse dilatation of a major epicardial, stented coronary artery that exceeded 1.5 times a diameter of the adjacent reference vessel at late angiography. Peri-stent contrast staining (PSS) was defined as contrast staining outside the Peri-stent contour extending to ≥20% of stent diameter measured by quantitative coronary angiography. Lesion complexity was classified according to the American Heart Association / American College of Cardiology lesion type classification. Stent fractures were defined as angiographic evidence of separation of the stent struts evaluated in multiple projections. Major adverse cardiovascular events included binary in-stent restenosis, target lesion revascularization, myocardial infarction, stent thrombosis and death.
E. Statistical analysis
Categorical data were presented as counts and percentages and compared using Pearson chi-square test, and continuous data were expressed as mean ± SD and compared using the Student t test. In order to find the independent risk factors for development of CAA or PSS, multivariable logistic regression analysis was performed. Kaplan-Meier survival analysis with log-rank significance was used for event-free survival. Cox’s regression proportional hazard ratio analysis was performed to find independent risk factors contributing for major adverse cardiovascular events. Statistical analyses were performed with SPSS 13.0 (SPSS Inc, Chicago, IL). 2-tailed p< .05 was considered statistically significant.
- 4 -
III.
RESULTS
A. Baseline Characteristics
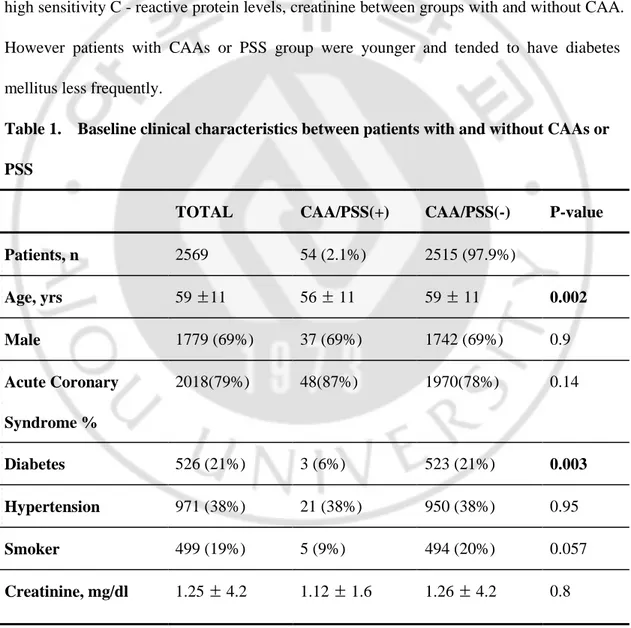
There are no significant differences in baseline clinical characteristics including gender, and hypertension, smoking history in addition to laboratory findings such as cholesterol and high sensitivity C - reactive protein levels, creatinine between groups with and without CAA. However patients with CAAs or PSS group were younger and tended to have diabetes mellitus less frequently.
Table 1. Baseline clinical characteristics between patients with and without CAAs or PSS
TOTAL CAA/PSS(+) CAA/PSS(-) P-value
Patients, n 2569 54 (2.1%) 2515 (97.9%) Age, yrs 59 ±11 56 ± 11 59 ± 11 0.002 Male 1779 (69%) 37 (69%) 1742 (69%) 0.9 Acute Coronary Syndrome % 2018(79%) 48(87%) 1970(78%) 0.14 Diabetes 526 (21%) 3 (6%) 523 (21%) 0.003 Hypertension 971 (38%) 21 (38%) 950 (38%) 0.95 Smoker 499 (19%) 5 (9%) 494 (20%) 0.057 Creatinine, mg/dl 1.25 ± 4.2 1.12 ± 1.6 1.26 ± 4.2 0.8
- 5 - Total Cholesterol, mg/dl 170 ± 57 174 ± 49 170 ± 57 0.65 HDL-Cholesterol, mg/dl 43 ± 12 42 ± 8 43 ± 12 0.56 LDL-Cholesterol, mg/dl 101 ± 42 106 ± 44 101 ± 42 0.39 Triglyceride, mg/dl 137 ± 97 132 ± 83 137 ± 98 0.73 hsCRP, mg/dl 0.60 ± 2.65 0.46 ± 1.15 0.61 ± 2.67 0.75
Values are expressed as lesions number (percentage) or mean ± SD.
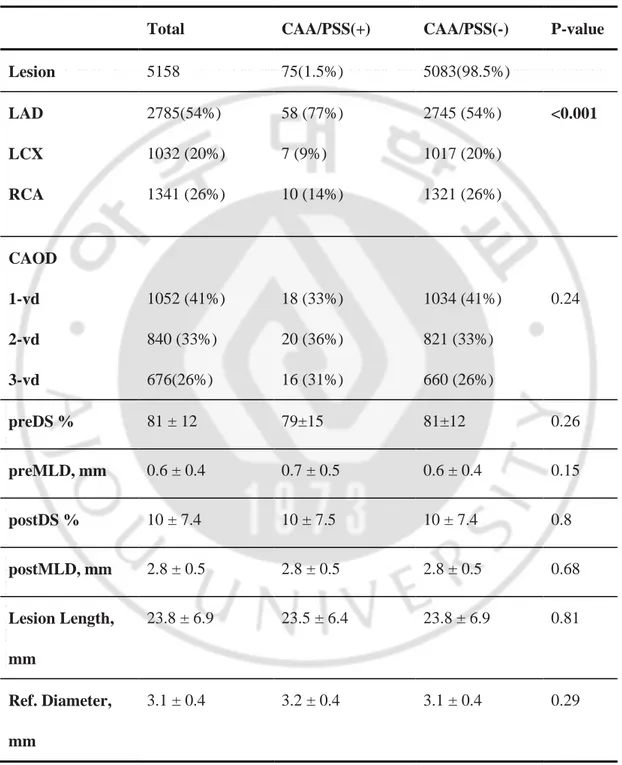
B. Angiographic findings
The CAAs and PSS were developed frequently with a drug-eluting stent compared with bare-metal stent. There was predilection among lesions of the left anterior descending artery (58 lesions, 77%) compared with the proportion of native lesions in patients without CAAs. Whereas other angiographic characteristics such as reference vessel size, minimal lumen diameter, diameter stenosis, and stent diameter did not differ significantly between groups. Stent length was longer in patients with CAA or PSS compared to patients without that abnormal lesion. It was interesting that Sirolimus-eluting stent was the most commonly used stent type in both groups but there were significant predominance in CAA/PSS group.
- 6 -
Table 2. Angiographic characteristics between patients with and without CAAs and PSS
Total CAA/PSS(+) CAA/PSS(-) P-value
Lesion 5158 75(1.5%) 5083(98.5%) LAD LCX RCA 2785(54%) 1032 (20%) 1341 (26%) 58 (77%) 7 (9%) 10 (14%) 2745 (54%) 1017 (20%) 1321 (26%) <0.001 CAOD 1-vd 2-vd 3-vd 1052 (41%) 840 (33%) 676(26%) 18 (33%) 20 (36%) 16 (31%) 1034 (41%) 821 (33%) 660 (26%) 0.24 preDS % 81 ± 12 79±15 81±12 0.26 preMLD, mm 0.6 ± 0.4 0.7 ± 0.5 0.6 ± 0.4 0.15 postDS % 10 ± 7.4 10 ± 7.5 10 ± 7.4 0.8 postMLD, mm 2.8 ± 0.5 2.8 ± 0.5 2.8 ± 0.5 0.68 Lesion Length, mm 23.8 ± 6.9 23.5 ± 6.4 23.8 ± 6.9 0.81 Ref. Diameter, mm 3.1 ± 0.4 3.2 ± 0.4 3.1 ± 0.4 0.29
- 7 - Stent Diameter, mm 3.1 ± 0.4 3.1 ± 0.3 3.1 ± 0.4 0.62 Stent Length, mm 25.3 ± 6.5 27.4 ± 6.2 25.3 ± 6.5 0.01 BMS 876 (17%) 2 (2%) 874 (18%) 0.001 DES 4333(84%) 73(98%) 4260(83%) 0.004 Sirolimus-eluting stents 2445 (47%) 66(85%) 2389(47%) <0.001 Paclitaxel-eluting stents 818 (16%) 4(5%) 813(16%) 0.025 Everolimus-eluting stents 562(11%) 3(1%) 559(11%) 0.04 Zotarolimus-eluting stents 227(4%) 0 227(4%) 0.04 High pressure balloon 2373(46%) 23(42%) 2350(46%) 0.5
Values are expressed as lesions number (percentage) or mean ± SD.
LAD, Left anterior descending artery; LCX, left circumflex artery; RCA, right coronary artery.
- 8 - BMS, bare metal stent; DES, drug-eluting stent
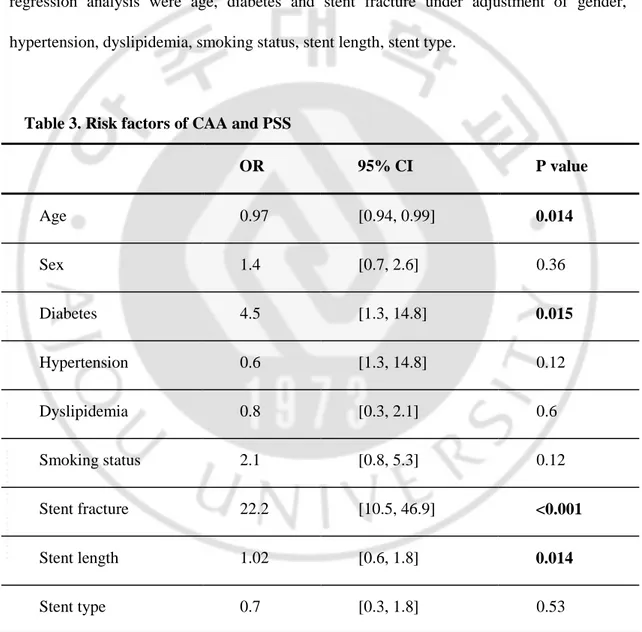
C. Risk Factors of CAAs & PSS
The independent risk factors for CAA or PSS identified by the multivariable logistic regression analysis were age, diabetes and stent fracture under adjustment of gender, hypertension, dyslipidemia, smoking status, stent length, stent type.
Table 3. Risk factors of CAA and PSS
OR 95% CI P value Age 0.97 [0.94, 0.99] 0.014 Sex 1.4 [0.7, 2.6] 0.36 Diabetes 4.5 [1.3, 14.8] 0.015 Hypertension 0.6 [1.3, 14.8] 0.12 Dyslipidemia 0.8 [0.3, 2.1] 0.6 Smoking status 2.1 [0.8, 5.3] 0.12 Stent fracture 22.2 [10.5, 46.9] <0.001 Stent length 1.02 [0.6, 1.8] 0.014 Stent type 0.7 [0.3, 1.8] 0.53
Stent length: using longer stents more than 30mm Stent type: drug eluting stent
- 9 -
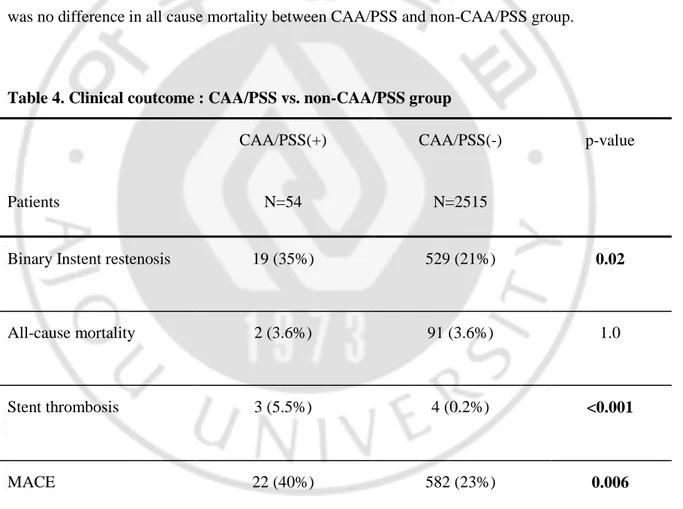
D. Clinical outcome : CAA/PSS group versus non-CAA/PSS group
The follow-up angiographic study revealed binary restenosis were 19 cases (35%) in CAA/PSS group, whereas there were 529 patients (21%) experienced binary instent restenosis in non-CAA/PSS group (p=0.02). All cause mortality was 3.6% in CAA/PSS group but there was no event of cardiac death. Total major cardiovascular events composed binary restenosis, myocardial infarction, death was increased in CAA/PSS group, but there was no difference in all cause mortality between CAA/PSS and non-CAA/PSS group.
Table 4. Clinical coutcome : CAA/PSS vs. non-CAA/PSS group
Patients CAA/PSS(+) N=54 CAA/PSS(-) N=2515 p-value
Binary Instent restenosis 19 (35%) 529 (21%) 0.02
All-cause mortality 2 (3.6%) 91 (3.6%) 1.0
Stent thrombosis 3 (5.5%) 4 (0.2%) <0.001
MACE 22 (40%) 582 (23%) 0.006
- 10 -
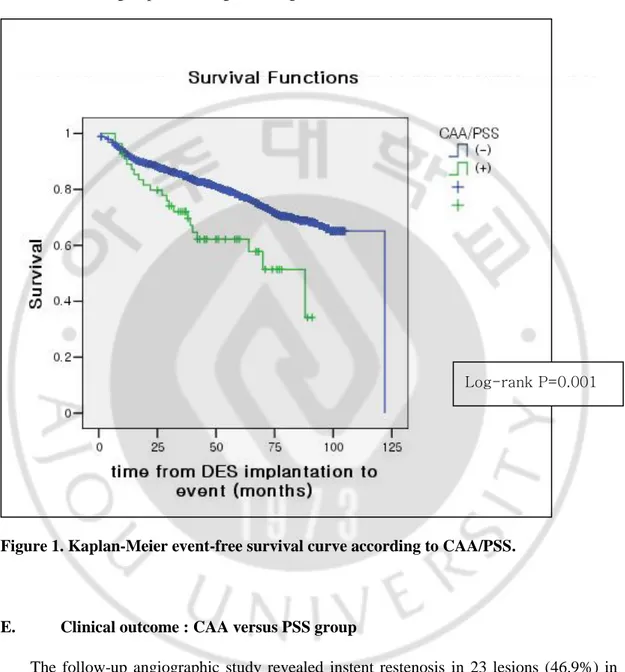
Survival analysis using Kaplan-Meier analysis showed significant difference in event-free survival between groups according to having CAA/PSS.
Figure 1. Kaplan-Meier event-free survival curve according to CAA/PSS.
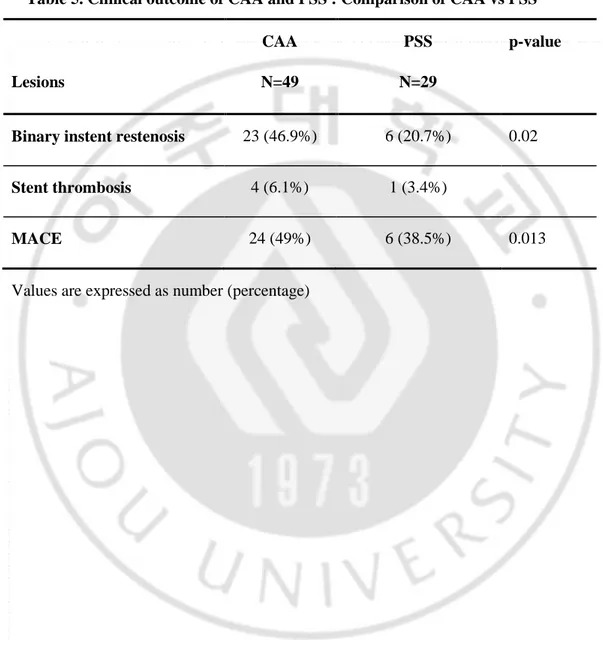
E. Clinical outcome : CAA versus PSS group
The follow-up angiographic study revealed instent restenosis in 23 lesions (46.9%) in CAA group and 6 lesions (20.7%) in the PSS group, respectively (P=0.02). Target lesion revascularization tended to occur more frequently in the CAA group than in the PSS group. There was no event of cardiac death in CAA/PSS group but cases with acute myocardial
- 11 -
infarction caused by stent thrombosis were 5 lesions in CAA/PSS group. Patients in CAA group experienced more frequent MACE compared with PSS group.
Table 5. Clinical outcome of CAA and PSS : Comparison of CAA vs PSS
Lesions CAA N=49 PSS N=29 p-value
Binary instent restenosis 23 (46.9%) 6 (20.7%) 0.02
Stent thrombosis 4 (6.1%) 1 (3.4%)
MACE 24 (49%) 6 (38.5%) 0.013
- 12 -
IV.
DISCUSSION
Although the published incidence of stent-associated CAA after DES implantation ranges from 0.3% to 6%, the true overall incidence of CAA or PSS in the real world practice remains unknown because of insufficient data and study design (Aoki et al., 2008). In our study, CAAs were rarely detected (1.5% per lesion, 2.1% per patient) during the angiographic follow-up. There is a concern that CAAs develop more commonly after DES compared to BMS implantation, available data including that from our review show that there is significantly frequent CAA/PSS formation in DES lesions compared to BMS lesions (Bavry et al., 2007; Aoki et al., 2008; Paulista et al., 2008; James et al., 2009). Especially patients undergoing PCI with sirolimus-eluting stent had dominantly CAA or PSS(Stabile et al., 2004; Virmani et al., 2004). CAA/PSS lesions could be regarded as representing an abnormal vessel wall response and PSS could be regarded as a continuum of pathological process in vessel wall at the site of DES implantation (Rab et al., 1991; Bell et al., 1992; Nebeker et al., 2006). The title the larger, the better in the BMS era might have caused more vascular injury due to the high-pressure balloon(Hill et al., 1983; Bell et al., 1992; Aoki et al., 2008); however, in the DES era, the high-pressure balloon was not routinely applied and it may have the effect of less vascular injury compared to the previous stent even though DES have the other factors such as polymeric and drug-related reactions (Köster et al., 2000; Stabile et al., 2004; Hong et al., 2006; Bavry et al., 2007; Alfonso et al., 2009).
Several mechanisms of CAA/PSS formation after DES implantation have been proposed, yet remained to be shown as relevant in most cases. Previous studies have shown that coronary arteries might be damaged by the toxic effects of drugs and polymers in DES(Rab et al.,
- 13 -
1991; Bell et al., 1992; Slota et al., 1997; Cook et al., 2009). Virmani et al reported some cases in which late thrombosis with malapposition and aneurysmal change occurs, especially in association with a hypersensitivity reaction to SESs(Virmani et al., 2004). Based on the fact that sirolimus is eluted from the stent struts for only 6 weeks (with a half life in the tissue of 60 hours), it seems unlikely that sirolimus itself can induce long-term alterations of the vessel wall(Köster et al., 2000; Hillen et al., 2002; Hong et al., 2006; James et al., 2009). There might be different mechanism for occurrence of CAA/PSS, the reason why CAA/PSS developed in younger and non-diabetic patients compared than non-CAA/PSS group. Procedural factors such as longer stent length might be related with lesion complexity as well as more “stent” effect on vessel wall. In the TAXUS VI trial, involving long and complex lesions, in 1.4% of patients in the paclitaxel-eluting stent arm late acquired aneurysms developed compared with patients in bare-metal stent arm (Dawkins et al., 2005; Nebeker et al., 2006).
Survival analysis showed significant difference in event free survival between CAA/PSS and non-CAA/PSS groups. The major cardiovascular adverse events including instent restenosis were significantly increased in CAA/PSS group compared with non-CAA/PSS group. Previous IVUS studies showed that CAA after DES implantation may be associated with DES restenosis and DES thrombosis (Hong et al., 2006; Alfonso et al., 2009). In current analysis, DES restenosis was more increased in CAA/PSS group but all cause mortality was not increased compared with patients in non-CAA/PSS group. Several reports about clinical outcome of CAA revealed that asymptomatic patients with CAA had benign course under continued dual antiplatelet therapy and did not experience life-threatening
- 14 -
problems, as our data revealed that no cardiac mortality related with CAA/PSS (Alfonso et al., 2009; Ahn et al., 2010).
In the current analysis, we used the PSS definition proposed by previous study which could be a transit phenomenon in the progression to CAA (Imai et al., 2011). There are several cases which showed progression from PSS to CAA during follow-up of angiography. Therefore the incidences of instent restenosis or target lesion revascularization tended to be higher in lesions with CAA than in lesions with PSS, suggesting that possible inflammatory reactions underlying CAA/PSS formation might be milder in PSS than CAA, which involved in the restenosis process of DES(Rab et al., 1991; Virmani et al., 2004). Also, cumulative incidence of stent thrombosis (ST) in lesions with CAA/PSS was numerically higher than ordinary post PCI results (Hong et al., 2006). Therefore, it would be reasonable to regard patients with CAA/PSS as being at high risk for subsequent ST. These observations might suggest that common mechanisms such as chronic inflammation might be operative for both VLST and restenosis requiring TLR(Aoki et al., 2008).
There are several important limitations in this study. First, this was a retrospective observational analysis of registry data from a single center with insufficient procedural information such as ballooning or stenting pressure to investigate the relationship of barotraumas to CAA/PSS occurrence. However, because of large volume center, the number of patients enrolled was not small and all patients who came into the cardiovascular center and underwent follow up angiography were included; therefore we could minimize selection bias. Second, the number of patients with PSS as well as CAA was relatively small to evaluate a possible correlation between morphological classification and risk of VLST. Also,
- 15 -
risk stratification for VLST according to the status of antiplatelet therapy could not be conducted because of the small number of patients with CAA/PSS. At last, most importantly, the number of patients with VLST after diagnosis of CAA/PSS, as well as in the non-CAA/PSS group, was very small, rendering the estimation of the incidences of VLST relatively inaccurate. The real incidences and risk factors of VLST and myocardial infarction after CAA/PSS diagnosis should be evaluated in a larger number of patients with scheduled follow-up.
- 16 -
V.
CONCLUSION
In this study, CAA or PSS rarely developed after PCI with rates that have increased in DES implantation group, especially SES. Younger age and non-diabetes were clinical risk factors for CAA/PSS development and stent length was the angiographic predictor of CAA development after DES implantation. The CAAs increased the risk of instent restenosis but not in all cause mortality. PSS is a phenomenon which did not fulfill the definition of CAA which might progress to CAA and related with similar clinical outcome with CAA. CAA/PSS group did not experience fatal cardiac clinical outcome under prolonged dual antiplatelet therapy. Further Investigations including serial imaging and clinical follow-up are required to determine proper treatment strategies.
- 17 -
REFERENCES
1.
Ahn CM, Hong BK, Kim JY, Min PK, Yoon YW, Lee BK, Kwon HM,
Kim JS, Ko YG, Choi D, Hong MK, Jang Y, Shim WH, Cho SY, Kim
BK, Oh S, Jeon DW, Yang JY, Jung JH: Incidence and natural
history of coronary artery aneurysm developing after drug-eluting
stent implantation. Am Heart J 160: 987-994, 2010
2.
Alfonso F, Perez-Vizcayno MJ, Ruiz M, Suarez A, Cazares M,
Hernandez R, Escaned J, Banuelos C, Jimenez-Quevedo P,
Macaya C: Coronary aneurysms after drug-eluting stent
implantation: clinical, angiographic, and intravascular ultrasound
findings. J Am Coll Cardiol 53: 2053-2060, 2009
3.
Aoki J, Kirtane A, Leon MB, Dangas G: Coronary artery aneurysms
after drug-eluting stent implantation. JACC Cardiovasc Interv 1:
14-21, 2008
4.
Bavry AA, Chiu JH, Jefferson BK, Karha J, Bhatt DL, Ellis SG,
Whitlow PL: Development of coronary aneurysm after drug-eluting
stent implantation. Ann Intern Med 146: 230-232, 2007
5.
Bell MR, Garratt KN, Bresnahan JF, Edwards WD, Holmes Jr DR:
Relation of deep arterial resection and coronary artery aneurysms
after directional coronary atherectomy. J Am Coll Cardiol 20:
1474-1481, 1992
6.
Cook S, Ladich E, Nakazawa G, Eshtehardi P, Neidhart M, Vogel R,
Togni M, Wenaweser P, Billinger M, Seiler C, Gay S, Meier B,
Pichler WJ, Juni P, Virmani R, Windecker S: Correlation of
- 18 -
thrombus aspirates in patients with very late drug-eluting stent
thrombosis. Circulation 120: 391-399, 2009
7.
Dawkins KD, Grube E, Guagliumi G, Banning AP, Zmudka K,
Colombo A, Thuesen L, Hauptman K, Marco J, Wijns W, Popma JJ,
Koglin J, Russell ME: Clinical efficacy of polymer-based
paclitaxel-eluting stents in the treatment of complex, long coronary artery
lesions from a multicenter, randomized trial: support for the use of
drug-eluting stents in contemporary clinical practice. Circulation
112: 3306-3313, 2005
8.
Hill JA, Margolis JR, Feldman RL: Coronary arterial aneurysm
formation after balloon angioplasty. American Journal of Cardiology
52: 261-264, 1983
9.
Hillen U, Haude M, Erbel R, Goos M: Evaluation of metal allergies in
patients with coronary stents. Contact Dermatitis 47: 353-356,
2002
10.
Hong MK, Mintz GS, Lee CW, Park DW, Park KM, Lee BK, Kim YH,
Song JM, Han KH, Kang DH, Cheong SS, Song JK, Kim JJ, Park
SW, Park SJ: Late stent malapposition after drug-eluting stent
implantation: an intravascular ultrasound analysis with long-term
follow-up. Circulation 113: 414-419, 2006
11.
Imai M, Kadota K, Goto T, Fujii S, Yamamoto H, Fuku Y, Hosogi S,
Hirono A, Tanaka H, Tada T, Morimoto T, Shiomi H, Kozuma K,
Inoue K, Suzuki N, Kimura T, Mitsudo K: Incidence, risk factors,
and clinical sequelae of angiographic peri-stent contrast staining
after sirolimus-eluting stent implantation. Circulation 123:
2382-2391, 2011
12.
James SK, Stenestrand U, Lindback J, Carlsson J, Schersten F,
- 19 -
of drug-eluting versus bare-metal stents in Sweden. N Engl J Med
360: 1933-1945, 2009
13.
Köster R, Vieluf D, Kiehn M, Sommerauer M, Kahler J, Baldus S,
Meinertz T, Hamm CW: Nickel and molybdenum contact allergies in
patients with coronary in-stent restenosis. Lancet 356: 1895-1897,
2000
14.
Nebeker JR, Virmani R, Bennett CL, Hoffman JM, Samore MH,
Alvarez J, Davidson CJ, McKoy JM, Raisch DW, Whisenant BK,
Yarnold PR, Belknap SM, West DP, Gage JE, Morse RE, Gligoric G,
Davidson L, Feldman MD: Hypersensitivity cases associated with
drug-eluting coronary stents: A review of available cases from the
Research on Adverse Drug Events and Reports (RADAR) project. J
Am Coll Cardiol 47: 175-181, 2006
15.
Paulista PP, Paulista PH, Centemero MP, Feres F: [Coronary
aneurysm after drug-eluting stent implantation]. Rev Bras Cir
Cardiovasc 23: 126-128, 2008
16.
Rab ST, King SB, 3rd, Roubin GS, Carlin S, Hearn JA, Douglas JS,
Jr.: Coronary aneurysms after stent placement: a suggestion of
altered vessel wall healing in the presence of anti-inflammatory
agents. J Am Coll Cardiol 18: 1524-1528, 1991
17.
Slota PA, Fischman DL, Savage MP, Rake R, Goldberg S:
Frequency and outcome of development of coronary artery
aneurysm after intracoronary stent placement and angioplasty.
American Journal of Cardiology 79: 1104-1106, 1997
18.
Stabile E, Escolar E, Weigold G, Weissman NJ, Satler LF, Pichard
AD, Suddath WO, Kent KM, Waksman R: Marked malapposition and
aneurysm formation after sirolimus-eluting coronary stent
- 20 -
19.
Virmani R, Guagliumi G, Farb A, Musumeci G, Grieco N, Motta T,
Mihalcsik L, Tespili M, Valsecchi O, Kolodgie FD: Localized
Hypersensitivity and Late Coronary Thrombosis Secondary to a
Sirolimus-Eluting Stent. Circulation 109: 701-705, 2004
- 21 - - 국문요약 –
관상 동맥 성형술 후 발생하는 관동맥류의 임상적 결과 및
예측인자 분석
아주대학교 대학원의학과 한 은 진 (지도교수: 탁 승 제) 관상동맥 성형술 후 발생하는 관동맥류 및 스텐트 주변 조영 소견은 관상동맥 성형술 이후 발생하는 주요 임상 사건의 발생, 즉 병변내 재관류 증가, 스텐트 내 혈전증에 의한 급성 심근 경색, 심인성 사망의 빈도가 증가하는 것과 연관된 다는 보고가 있어 주의를 요하였다. 하지만 최근 약물 용출 스텐트 삽입술을 시 행한 환자들의 대규모 임상 연구를 통한 보고에서는 이중 항 혈소판제를 지속적 으로 사용하는 경우 임상 경과가 양호하였던 것을 보고하였다. 실제 의료 환경에 서의 관상동맥 성형술 이후 발생하는 관동맥류 및 스텐트 주변 조영의 발생 빈 도와 발생에 미치는 요인 및 임상 결과를 확인하기 위하여 2003년 1월부터 2010 년 12월까지 아주대학교 병원 순환기내과에 내원하여 관상동맥 성형술을 시행 받은 환자 중 추적 관동맥 조영술을 시행한 환자 2659명을 분석하여 관동맥류 및 스텐트 주변 조영 소견이 나타난 54명의 환자 78 병변을 분석하였다. 관동맥 류 및 스텐트 주변 조영 소견이 나타난 환자는 전체의 2.1%, 병변은 전체 병변의- 22 - 1.5% 였으며 좌전행지에서 흔하게 발병하였고 약물 용출 스텐트가 98%에서 사 용되었으며 주로 Sirolimus-eluting stent가 사용되었고(77%) 병변에 사용한 스텐트 길이가 통계적으로 유의하게 길었다. 관동맥류 및 스텐트 주변 조영이 발생한 환 자군은 발생하지 않은 환자군에 비해 젊고 당뇨 환자가 유의하게 적었다. 관동맥 류 및 스텐트 주변 조영의 발생은 스텐트내 재협착의 유의한 증가와 관련되어 주요 심혈관 사건의 증가를 가져오나 실제로 관동맥류 및 스텐트 주변 조영이 있었던 환자 중 심인성 사망과 같은 치명적인 임상 결과는 없었으며 모든 원인 에 의한 사망은 관동맥류 및 스텐트 주변 조영이 발생한 환자나 발생하지 않은 환자 군에서 발생 빈도가 같았다. 또한 스텐트 주변 조영은 시간이 지나면 관동 맥류로 진행하는 소견을 보이거나 관동맥류 병변이 시간이 지남에 따라 자연적 으로 소실되는 소견을 보여 두 영상학적 병변은 약물 용출 스텐트에 의한 혈관 벽의 변화를 보여주는 연속적인 병변으로 고려될 수 있었으나 관동맥류가 발생 한 환자군에 비하여 스텐트 주변 조영만 발생한 환자군에서는 주요 심혈관 사건 의 발생은 유의하게 낮아 보다 임상적으로 보다 경미한 상태로 고려될 수 있겠 다. 최근의 문헌 고찰에 따르면 무증상 환자에서 관동맥류 및 스텐트 주변 조영 이 발생한 경우 이중 항 혈소판제를 지속적으로 유지한 경우 주요 심혈관 사건 의 발생이 적은 비교적 양호한 임상경과를 보이는 결과가 보고되었는데 이는 본 연구의 결과와 부합하는 소견이었다. 핵심어: 관동맥 성형술, 관동맥류, 스텐트 주변 조영, 임상 경과, 예측인자, 약물용출 스텐트