Outcomes of bare metal stents
simultaneously implanted w ith
sirolimus-eluting stents in multivessel
coronary artery disease patients: potential
systemic effect of sirolimus-eluting stent
Sung Ju Lee
Department of Medicine
Outcomes of bare metal stents
simultaneously implanted w ith
sirolimus-eluting stents in multivessel
coronary artery disease patients: potential
systemic effect of sirolimus-eluting stent
Directed by Professor Young Won Yoon
The Master's Thesis submitted to the
Department of Medicine
the Graduate School of Yonsei University
in partial fulfillment of the requirements for the
degree of Master of Medicine
Sung Ju Lee
This certifies that the Master's Thesis
of Sung Ju Lee is approved.
Thesis Supervisor : Young Won Yoon
Thesis Committee Member : Hyuck Moon Kown
Thesis Committee Member : Hwal Suh
The Graduate School
Yonsei University
감사의
감사의
감사의
감사의 글
글
글
글
먼 먼먼저저저 논논논문문문을을을 쓰쓰기쓰기기 시시시작작작할할할 때때때부부부터터터 완완완료료료할할할 때때 까때 까까지지지 지지지도도도해해해 주 주주시시시고고고,,,미미미흡흡흡한한한 점점점이이이 많많많았았았어어어도도도 따따따뜻뜻뜻하하하게게게 격격격려려려해해해주주시주시시고고고,,,충충충고고고해해해 주 주주신신신 윤윤윤영영영원원원 교교교수수수님님님께께께 진진진심심심으으으로로로 감감감사사사드드드립립립니니니다다다... 그 그그리리리고고고 이이이 논논논문문이문이이 완완완성성성되되되기기기까까지까지지 지지지도도도하하하여여여 주주주신신신 권권권혁혁혁문문문 교교교 수 수수님님님과과과 서서서활활활 교교교수수수님님님께께께도도도 깊깊깊은은은 감감감사사사를를를 드드드립립립니니니다다다... 또 또또한한한,,,연연연구구구 진진행진행행에에에 있있있어어어서서서 많많많은은은 도도도움움움을을을 준준준 영영동영동동세세세브브브란란란스스스 병 병병원원원 내내내과과과 동동동기기기인인 종인 종종관관관,,,진진진혁혁혁,,,근근근만만만,,,민민민수수수,,,혜혜혜진진 에진 에에게게게도도도 감감감사사사하하하 고 고고,,,논논논문문문의의의 통통통계계계 및및및 전전전반반반적적적인인인 진진행진행행에에에 있있있어어어서서서 도도움도움움을을을 많많많이이이 주주주었었었 던 던던 성성성우우우에에에게게게 더더더욱욱더욱더더 감감감사사사드드드립립립니니니다다다...그그그리리리고고고 자자자료료료 모모모음음음에에에 자자자기기기 일일일 처 처처럼럼럼 열열열심심심히히히 도도도와와와준준준 후후후배배배 현현현철철철,,,심심심도도도자자자실실실 신신신용용용학학학 선선선생생생님님님,,,김김김경경경 애 애애 간간간호호호사사사,,,주주주현현현 씨씨씨에에에게게게도도도 감감감사사하사하하고고고,,,영영영어어어 교교정교정정에에에 도도도움움움을을을 준준준 후 후후배배배 지지지선선선에에에게게게도도도 감감감사사사드드드립립립니니니다다다... 무 무무엇엇엇보보보다다다도도도 오오오늘늘늘날날날까까까지지지 저저저를를를 있있있게게게 해해해주주주신신신 하하하나나나님님님,,,그그그리리리고고고,,, 언 언언제제제나나나 아아아들들들을을을 챙챙챙겨겨겨주주주시시시는는는 것것것 이이상이상상으으으로로로 저저저의의의 인인생인생생의의의 전전전반반반을을을 도도도 와 와와주주주시시시는는는 어어어머머머니니니,,,아아아버버버지지지 그그그리리리고고고,,,장장장인인인,,,장장장모모모님님님께께께도도도 감감감사사사드드드립립립니니니 다 다다...또또또한한한,,,언언언제제제나나나 저저저의의의 곁곁곁에에에서서서 토토토론론론과과과 충충충고고고를를를 아아끼아끼끼지지지 않않않은은은 사사사랑랑랑 하 하하는는는 아아아내내내 공공공지지지현현현과과과 기기기쁨쁨쁨을을을 함함함께께께 하하하고고고 싶싶싶습습습니니니다다다... 저저저 자자자 씀씀씀<TABLE OF CONTENTS>
Ⅰ . INTRODUCTION ··· 3
Ⅱ . MATERIALS AND METHODS ··· 5
1. Subjects ··· 5
2. Global risk assessment scoring ··· 6
3. Coronary intervention procedure ··· 7
4. Angiographic analysis ··· 8
5. Study end point ··· 10
6. Statistical analysis ··· 11
Ⅲ . RESULTS ··· 12
1. Characteristics of study population ··· 12
2. Angiographic outcome ··· 14
3. Subgroup analysis according to stented vessel in BM S+SES group ··· 17
4. M ultivariate analysis of predictors for in-stent restenosis ··· 18
Ⅳ . DISCUSSION ··· 20
V. CONCLUSION ··· 23
LIST OF FIGURES
Figure 1. Framingham scoring system for calculating the
10-year risk of major coronary event ··· 6
Figure 2. Quantitative angiographic analysis for follow up
angiographic result assessments ··· 9
Figure 3. Comparison of marginal distribution of at 6-months
follow-up percent diameter stenosis ··· 15
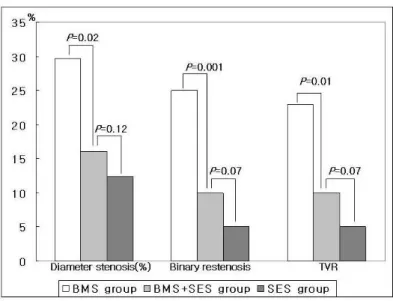
Figure 4. Comparison of diameter stenosis, binary restenosis
and TVR between BMS group, BMS+SES group
and SES group ··· 16
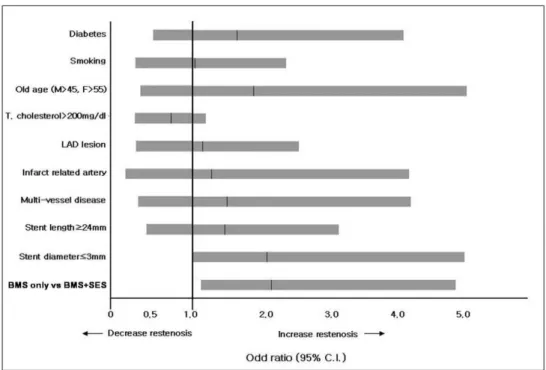
Figure 5. Multivariate analysis of predictors for in-stent
LIST OF TABLES
Table 1. Baseline characteristics of patients who received
BMS or SES ··· 12
Table 2. Baseline pre-procedural and post procedural angio
-graphic characteristics ··· 13
Table 3. Follow-up angiographic results ··· 14
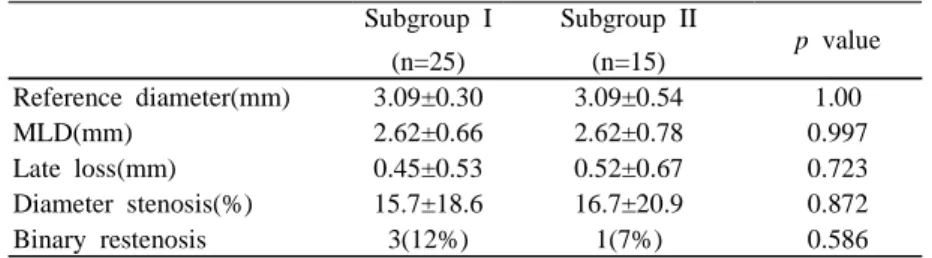
Table 4. Subgroup analysis for cobalt-chromium BMS
simultaneously implanted with SES in BMS+SES
group ··· 17
Table 5. Multivariate analysis of predictors for in-stent
A B STRA CT
Outcomes of bare metal stents simultaneously implanted with sirolimus-eluting stents in multivessel coronary artery disease patients:
potential systemic effect of sirolimus-eluting stent
Sung Ju Lee
Department of Medicine
The Graduate School, Yonsei University
(Directed by Professor Young W on Yoon)
Clinical studies with sirolimus-eluting stents(SESs) have shown a dramatic and sustained reduction in the degree of neointimal hyperplasia and in-stent restenosis. In spite of very low restenosis rate, the high cost and safety profiles of SES implantation preclude their use in routine angioplasty, especially when considering multi-vessel stenting. We evaluated outcomes of cobalt-chromium bare metal stent(BMS) simultaneously implanted with SES in multivessel coronary artery disease patients by 6 months angiographic follow-up in the present study.
The present study enrolled consecutive 209 patients (238 lesions) who had symptomatic coronary artery disease successfully treated with SESs or cobalt-chromium BMSs, and had undergone follow-up angiography. At the 6 months follow-up angiography, Late loss, minimal luminal diameter(MLD), diameter stenosis(%) of BMS were significantly lower in the SES+BMS group compared with BMS only group. In-stent binary angiographic restenosis and target vessel revascularization(TVR) of BMS were significantly reduced in the BMS+SES group compared with BMS only group (25/108 vs 4/40, p<0.01, 23/108 vs 4/40
restenosis risk when compared with BMS simultaneously implanted with SES by multivariate analysis (OR=2.154, 95% C.I.=1.179-4.959, p=0.04). The result of this study suggests that SES implantation can decrease neointimal proliferation of simultaneously implanted cobalt-chromium BMS by potential systemic sirolimus effect.
Key Words: bare-metal stent (BMS), sirolimus-eluting stent(SES), neointimal proliferation, restenosis, systemic effect.
Outcomes of bare metal stents simultaneously implanted with sirolimus-eluting stents in multivessel coronary artery disease patients: potential systemic effect of sirolimus-eluting stent
Sung Ju Lee
Department of Medicine
The Graduate School, Yonsei University
(Directed by Professor Young W on Yoon)
Ⅰ
ⅠⅠ . INTRODUCTION
In-stent restenosis(ISR) constitutes the major drawback of percutaneous coronary interventions. Despite leading to better results compared with plain balloon angioplasty, the long-term success of coronary stenting has also been limited by a significant rate of restenosis.1,2 Recently, cutting ballon angioplasty or intracoronary brachytherapy has been used to treat ISR, but the rate of recurrence after treatment for ISR remains high(>30%).3,4,5 The predominant mechanism of ISR is neointimal tissue proliferation, which is characterized by an inflammatory reaction at the site of injury, the migration and proliferation of vascular smooth muscle cells, and the synthesis of excessive extracellular matrix.
Clinical studies with sirolimus eluting stents(SESs) have shown a dramatic and sustained reduction in the degree of neointimal hyperplasia and in-stent restenosis.6,7,8 The natural macrocyclic lactone sirolimus is a potent immuno
-suppressive agent. Sirolimus binds to an intracellular receptor protein and elevates p27 levels, which leads to inhibition of cyclin-dependent kinase complexes and ultimately induces cell-cycle arrest in the late G1 phase.9 In recent studies,10 administration of oral sirolimus inhibited ISR, but adverse effect were frequent, underscoring the importance of local drug delivery to achieve high tissue concentrations without systemic adverse effect. Clinical studies with SES have shown local delivery effect11,12 and reduced serum C-reactive protein.13,14
In spite of very low restenosis rate, the high cost of SES implantation preclude their use in routine angioplasty, especially when considering multiple stenting. In a recent study,15 acute myocardial infarction secondary to late stent thrombosis at 18 months post stent deployment was reported, and SESs were associated with exercised induced paradoxic coronary vasoconstriction due to diffusion of the antiproliferative drug from the stent to the peri-stent region, inducing endothelial dysfunction.16 Moreover, SES are not variable in lengths and diameters and not easy to implant the stent to the target lesion in severe angulated or calcified lesion. By these reasons, there are some limitations for SES implantation in all coronary interventions. Although systemic sirolimus level is very low after SES implantation, there are possible systemic effects of sirolimus and SES may influence neighboring vessels.17 So, we evaluated systemic effect of SES by 6 months follow-up angiographic evaluation for cobalt-chromium bare metal stent(BMS) simultaneously implanted with SES in this study. The purpose of this study was to evaluate the hypothesis that SES implantation could decrease neointimal proliferation of cobalt-chromium BMS by systemic sirolimus effect in case of multi-vessel stenting.
Ⅱ
ⅡⅡ . MATERIALS AND METHODS
1. Subjects
209 consecutive patients (238 lesions) who had symptomatic coronary artery disease successfully treated with SESs or cobalt-chromium stents were enrolled in this study, and we had undergone follow-up angiography between January 2004 and September 2005 at Yongdong Severance Hospital, Yonsei University. Another type of drug-eluting stent (paclitaxel-eluting stent) deployed patients were excluded.
The diagnosis of hypertension was based on the known history of hypertension and the systolic blood pressure over 140mmHg or diastolic blood pressure over 90mmHg. Diabetes mellitus was diagnosed as fasting serum glucose level over 126 mg/dl, or treatment with either oral hypoglycemic agents or insulin. ST-segment elevation myocardial infarction(STEMI), non ST-segment elevation myocardial infarction(NSTEMI) and Unstable angina(UA) were difined as acute coronary syndrome(ACS).18 Total cholesterol was determined by the cholesterol -oxidase method (Daiichi, Tokyo, Japan). Low density lipoprotein (LDL) -cholesterol levels were assessed via the direct enzymatic method, using cholestest LDL (Daiichi,Tokyo, Japan). High density lipoprotein (HDL)-cholesterol levels were determined by the direct method, using polyethylene glycol-modified enzymes (Daiichi,Tokyo, Japan).
A "per-lesion" analysis was performed for all angiographic parameters in this study. The study group (BMS+SES group) was defined as cobalt-chromium BMS simultaneously implanted with SES. SES treated patients designated as the SES group, and cobalt-chromium BMS treated patients without SES insertion were designated as the BMS group.
2. Global risk assessment scoring
10-year risk of major coronary events was calculated by using Framingham scoring system based on Framingham Heart Study.19,20
Figure 1. Framingham scoring system for calculating the 10-year risk of major coronary events in adults without diabetes. All age ranges are given in years.
3. Coronary intervention procedure
Coronary angioplasty was performed according to standard rules and the experience of the operator. All patients received bolus injection of unfractionated heparin (10,000 U) before procedures. The patients were treated with oral aspirin (200mg daily) and clopidogrel (loading dose 300mg, then 75mg daily). The intervention procedures employed the femoral approach. Patients were underwent implantation of either a cobalt-chromium BMS (Vision® stent: Guidant Corp., Santa Clara, CA, USA, Driver® stent: Medtronic AVE Inc., Minneapolis, MN, USA) or SES (Cypher® stent: Cordis Corp, Roden, Netherland). The procedure was considered to be successful if the quantitative coronary angiography (QCA) estimated residual stenosis was <30% and TIMI 3 flow distally was observed immediately after stent implantation.21
4. Angiographic analysis
We performed quantitative computer-assisted offline analysis (QCA) of the angiogram, using the automated edge-detection system (Medis Medical Imaging System, Nuenen, Netherlands). The coronary catheter was used for calibration. In most case, the interpolated reference diameter(RD) was used to calculate percent stenosis. All steps in the analysis, including frame selection, QCA analyses, were carried out fully blinded to the indenity and clinical status of the patients. The pre-PCI RD, minimal lumen diameter(MLD), lesion length, and post-PCI MLD, RD were evaluated by QCA analysis. At the 6 months follow-up angiography, MLD, RD, percent diameter restenosis were also evaluated by QCA method (Figure 2). Lesion length was defined as the axial extent of the lesion that contained a shoulder to shoulder lumen reduction by >20%.22 Reference diameter was calculated the average of proximal and distal to the lesions. Binary restenosis was defined as the incidence of percent diameter stenosis >50% at the QCA follow-up.22 The lesion morphology exam was classified using the modified American College of Cardiology/American Heart Association grading system, as type A, B1, B2, or C lesions.23 Complex lesions were defined as type B or C lesions.24
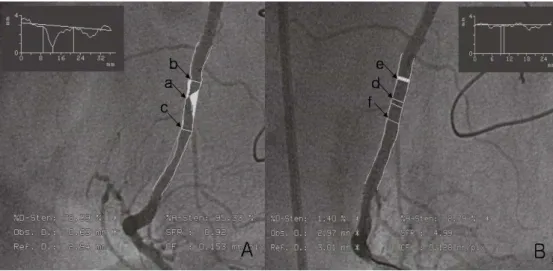
Figure 2. Quantitative angiographic analysis. Selected images for analysis were identified by angiographic projection that demonstrated the stenosis in an unforeshortened view, minimized the degree of vessel overlap.
A. critical restenosis of mid-RCA at 6-months follow-up; a: minimal lumen diameter(MLD), b: proximal luminal diameter, c: distal luminal diameter, reference diameter: (proximal luminal diameter+distal luminal diameter)/2.
B. QCA of post successful target vessel revascularization(TVR); d: post-procedure MLD, e,f: proximal and distal luminal diameter.
5. Study end point
The primary end point of this study was late lumen loss as assessed by QCA at 6 months follow-up. The secondary end points included other angiographic parameters of restenosis, such as binary restenosis and MLD, TVR at 6 months follow-up.
6. Statistical Analysis
Statistical analyses were performed using a SPSS 11.0 for Windows (SPSS Inc., IL, USA). The treatment group difference were presented as mean ± standard deviation and were evaluated with the ANOVA for continuous variables. Fisher's exact statistics, controlling for the site groups, were used for the categorical variables. Multivariate analysis (logistic regression) was also performed, in order to determine the parameter for the prediction of angiographic ISR. A statistical significance was declared if the 2-sided probability value was <0.05.
Ⅲ
ⅢⅢ . RESULTS
1. Characteristics of study population
The general and metabolic characteristics of all the patients studied were shown in Table 1. There were no difference between the BMS+SES group, the SES group, and the BMS group in age, gender, DM, hypertension, lipid profiles, smoking history, Framingham risk score, and clinical diagnosis. Mean baseline reference diameter was smaller in the BMS+SES group (3.07±0.42 vs 3.28±0.38,
p<0.001). Baseline stent diameter was also smaller in the BMS+SES group
(3.21±0.35 vs 3.36±0.73, p=0.004) (Table 2).
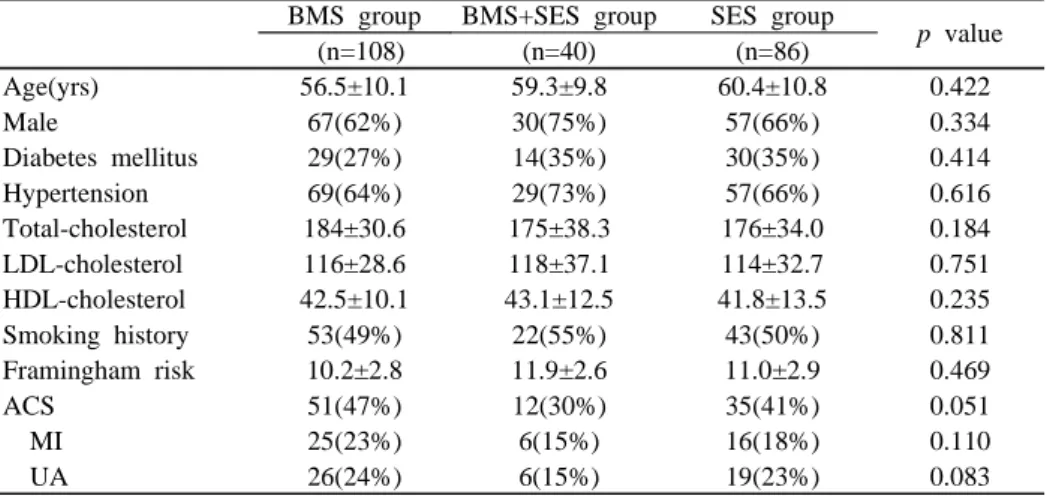
Table 1. Baseline Characteristics of Patients Who Received BMS or SES
Data are expressed as mean ± SD.
Abbreviations; BMS group: BMS only implanted group, BMS+SES group: BMS simultaneously implanted with SES, SES group: SES only implanted group, ACS: acute coronary syndrome, LDL: low-density lipoprotein, HDL: high-density lipoprotein, MI: myocardial infarction, UA: unstable angina
BMS group BMS+SES group SES group
p value (n=108) (n=40) (n=86) Age(yrs) 56.5±10.1 59.3±9.8 60.4±10.8 0.422 Male 67(62%) 30(75%) 57(66%) 0.334 Diabetes mellitus 29(27%) 14(35%) 30(35%) 0.414 Hypertension 69(64%) 29(73%) 57(66%) 0.616 Total-cholesterol 184±30.6 175±38.3 176±34.0 0.184 LDL-cholesterol 116±28.6 118±37.1 114±32.7 0.751 HDL-cholesterol 42.5±10.1 43.1±12.5 41.8±13.5 0.235 Smoking history 53(49%) 22(55%) 43(50%) 0.811 Framingham risk 10.2±2.8 11.9±2.6 11.0±2.9 0.469 ACS 51(47%) 12(30%) 35(41%) 0.051 MI 25(23%) 6(15%) 16(18%) 0.110 UA 26(24%) 6(15%) 19(23%) 0.083
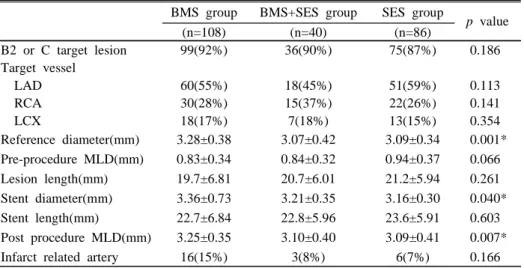
Table 2. Baseline pre-procedural and post-procedural angiographic Characteristics
Data are expressed as mean ± SD.
Abbreviations; BMS group: BMS only implanted group, BMS+SES group: BMS simultaneously implanted with SES, SES group: SES only implanted group, LAD: left anterior descending artery, RCA: right coronary artery, LCX: MLD: minimal lumen diameter
*p<0.05
BMS group BMS+SES group SES group
p value (n=108) (n=40) (n=86) B2 or C target lesion 99(92%) 36(90%) 75(87%) 0.186 Target vessel LAD 60(55%) 18(45%) 51(59%) 0.113 RCA 30(28%) 15(37%) 22(26%) 0.141 LCX 18(17%) 7(18%) 13(15%) 0.354 Reference diameter(mm) 3.28±0.38 3.07±0.42 3.09±0.34 0.001* Pre-procedure MLD(mm) 0.83±0.34 0.84±0.32 0.94±0.37 0.066 Lesion length(mm) 19.7±6.81 20.7±6.01 21.2±5.94 0.261 Stent diameter(mm) 3.36±0.73 3.21±0.35 3.16±0.30 0.040* Stent length(mm) 22.7±6.84 22.8±5.96 23.6±5.91 0.603 Post procedure MLD(mm) 3.25±0.35 3.10±0.40 3.09±0.41 0.007*
2. Angiographic outcome
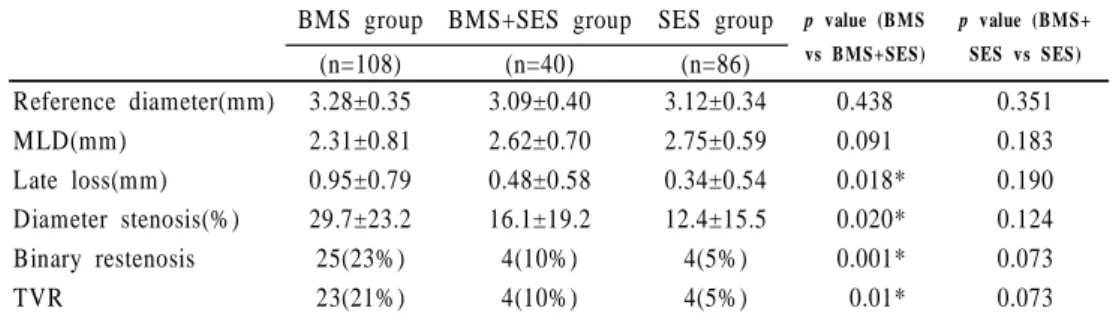
Follow-up angiography was performed in all lesions (n=234). Mean follow-up duration was 229±69days. Follow-up angiographic results were shown Table 3. Late loss, MLD, diameter stenosis(%) of BMS were significantly lower in the BMS+SES group compared with the BMS group. Marginal distribution of follow-up angiographic result demonstrated skew pattern to right in the BMS+SES group and SES group (Figure 3). In-stent binary angiographic restenosis and TVR of BMS were significantly reduced in the BMS+SES group compared with the BMS group (25/108 vs 4/40, p<0.01, 23/108 vs 4/40 p=0.01). However, there were no significant difference of binary restenosis, diameter stenosis(%) and TVR of BMS between BMS+SES group and SES group (10% vs 5%, p=0.07, 16.1% vs 12.4%,
p=0.12, 10% vs 5%, p=0.07) (Figure 4).
Table 3. Follow-up Angiographic Results
Data are expressed as mean ± SD.
Abbreviations; BMS group: BMS only implanted group, BMS+SES group: BMS simultaneously implanted with SES, SES group: SES only implanted group, MLD: minimal lumen diameter, TVR: target vessel revascularization
*p<0.05
BMS group BMS+SES group SES group p value (B MS
vs B MS+SES) p value (BMS+ SES vs SES) (n=108) (n=40) (n=86) Reference diameter(mm) 3.28±0.35 3.09±0.40 3.12±0.34 0.438 0.351 MLD(mm) 2.31±0.81 2.62±0.70 2.75±0.59 0.091 0.183 Late loss(mm) 0.95±0.79 0.48±0.58 0.34±0.54 0.018* 0.190 Diameter stenosis(%) 29.7±23.2 16.1±19.2 12.4±15.5 0.020* 0.124 Binary restenosis 25(23%) 4(10%) 4(5%) 0.001* 0.073 TVR 23(21%) 4(10%) 4(5%) 0.01* 0.073
Figure 3. Marginal distribution of at 6-month follow-up. percent diameter stenosis were skewed to the right in the SES group and BMS+SES group.
Figure 4. Comparison of diameter stenosis, binary restenosis and TVR between BMS group, BMS+SES group and SES group. In-stent binary angiographic restenosis and TVR of BMS were significantly reduced in the BMS+SES group compared with the BMS group(23% vs 10%, p<0.01, 21% vs 10% p=0.01). diameter stenosis(%) was also significantly lower in the BMS+SES group compared with the BMS group (30% vs 16%). However, there were no significant difference of binary restenosis, diameter stenosis(%) and TVR between BMS+SES group and SES group (10% vs 5%, p=0.07, 16.1% vs 12.4%, p=0.12, 10% vs 5%, p=0.07)
3. Subgroup analysis according to stented vessel in BMS+SES group
The comparison of subgroup analysis for cobalt-chromium BMS simultaneously implanted with SES was shown in Table 4. There were no difference between subgroup I (BMS in same system of coroanry circulation, ex>LCA: SES implantation, LCA: BMS implantation) and subgroup II (BMS in other system of coronary circulation, ex>LCA: SES implantation, RCA: BMS implantation) in late loss, MLD, diameter stenosis, binary restenosis and TVR.
Table 4. Subgroup analysis for cobalt-chromium BMS simultaneously implanted with SES in BMS+SES group
Data are expressed as mean ± SD.
Abbreviations; Subgroup I: same system implantation, Subgroup II: other system implantation, MLD: minimal lumen diameter
Subgroup I (n=25) Subgroup II (n=15) p value Reference diameter(mm) 3.09±0.30 3.09±0.54 1.00 MLD(mm) 2.62±0.66 2.62±0.78 0.997 Late loss(mm) 0.45±0.53 0.52±0.67 0.723 Diameter stenosis(%) 15.7±18.6 16.7±20.9 0.872 Binary restenosis 3(12%) 1(7%) 0.586
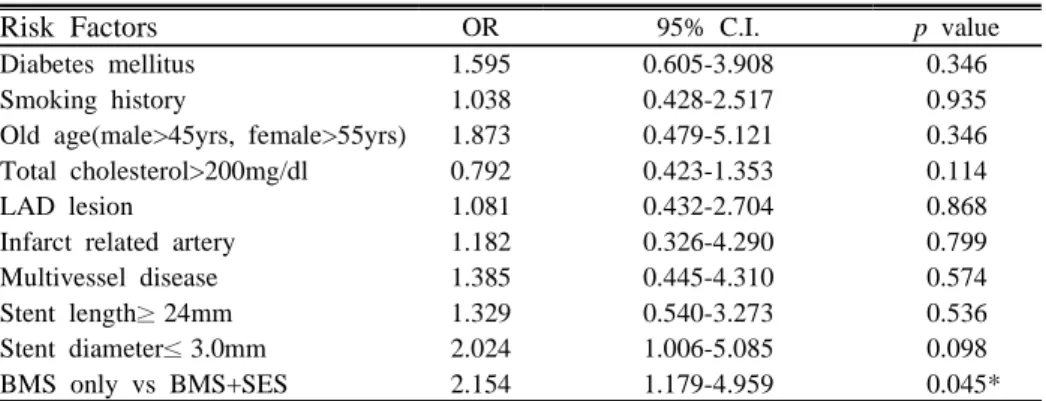
4. Multivariate analysis of predictors for in-stent restenosis
We constructed a multivariate model for predictors associated with restenosis. The BMS only implantation without SES increased restenosis risk compared with BMS simultaneously implanted with SES by multivariate analysis (OR=2.154, 95% C.I.=1.179-4.959, p=0.04). Other predictors were not related to in-stent restenosis (Table 5), (Figure 5).
Table 5. Multivariate analysis of predictors for in-stent restenosis
Abbreviations; LAD: left anterior descending artery, BMS: bare-metal stent *p<0.05
Risk Factors OR 95% C.I. p value
Diabetes mellitus 1.595 0.605-3.908 0.346
Smoking history 1.038 0.428-2.517 0.935
Old age(male>45yrs, female>55yrs) 1.873 0.479-5.121 0.346
Total cholesterol>200mg/dl 0.792 0.423-1.353 0.114
LAD lesion 1.081 0.432-2.704 0.868
Infarct related artery 1.182 0.326-4.290 0.799
Multivessel disease 1.385 0.445-4.310 0.574
Stent length≥ 24mm 1.329 0.540-3.273 0.536
Stent diameter≤ 3.0mm 2.024 1.006-5.085 0.098
Figure 5. Multivariate analysis of predictors for in-stent restenosis. The BMS only implantation without SES increased restenosis risk compared with BMS simultaneously implanted with SES by multivariate analysis (OR=2.154, 95% C.I.=1.179-4.959, p=0.04).
ⅣⅣⅣ . DISCUSSION
This study demonstrated that the use of cobalt-chromium BMS, simultaneously implanted with SES (BMS+SES group) was more effective in reducing angiographic parameters of restenosis in patients with complex multivessel disease at a high risk for restenosis when compared with the use of cobalt-chromium BMS. Furthermore, the angiographic restenosis of BMS was markedly reduced in patients with complex disease by the use of SES in this study. The beneficial effect of cobalt-chromium BMS simultaneously implanted with SES on binary angiographic restenosis is attributed to reductions in the late lumen loss within the BMS+SES group(0.48mm) compared with the BMS group(0.95mm), a favorable effect that extends to the TVR(10% vs 21%).
This study also investigated the predictors of in-stent restenosis. In a recent study, in-stent restenosis was shown to be related to DM, smoking history, infarct related artery, age, cholesterol level, multi-vessel disease, small stent diameters, and long stent length.25 In our study, the patients who were treated with the BMS-only stent were at a higher risk for restenosis compared with those who had BMS+SES stent implanted, according to a multivariate analysis (OR=2.154, 95% C.I.= 1.179-4.959, p=0.04). These results suggest that the implantation of sirolimus stent might have inhibited the neointimal hyperplasia of the adjacent vessels, which were stented with BMS.
We also performed the subgroup analysis for BMS+SES group for a more comprehensive evaluation on the effect of sirolimus. There were no differences in the late loss, MLD, diameter stenosis, binary restenosis and TVR depending on the type of implantation system used. This result suggests that the cobalt-chromium BMS simultaneously implanted with SES whether in same of other system of coronary circulation, shows its advanced effect through its systemic effect, instead of a local effect. This effect might be similar with oral adminstration. However, the
systemic adminstration of oral rapamycin has a serious adverse effect in the therapeutic dosage for the anti-neointimal proliferation effect on coronary vessel.26,27
Drug eluting stents offer the possibility of delivering therapeutic levels of active metabolite locally while maintaining negligible levels in the systemic ciuculation.28 However, Uchimura et al29 reported that the low dose oral sirolimus may be more effective than high doses, paradoxically. Several recent studies also showed that a more intense inflammatory response to coronary stenting, as assessed by serial measurements of C-reactive protein, was associated with an increased risk of restenosis among patients who received SES.13,30 Although there were no clinical systemic adverse effects in the SIRIUS trial, systemic influence may occur by SES implantation in these reasons.31 Therefore, this present study suggests that BMS implantation simultaneously with SES may be a novel treatment in multivessel coronary artery disease without any systemic adverse effect.
Theoretical concerns that SES could be associated with higher rates of stent thrombosis due to a delayed endothelialization32 and premature discontinuation of clopidogrel were associated with a 30-fold greater risk of stent thrombosis in SES treatment.33 In a recent study, discontinuation of anti-platelet therapy was strongly associated with the development of stent thrombosis.34 Furthermore, there are several other limitations with DES. For example, it is difficult to insert DES at a diffuse, long lesion and calcified, angulated lesion due to the lack of diversity in diameter and length of DES, despite numerous studies that demonstrated the reduced adverse cardiac events and neointimal hyperplasia with the use of DES compared to BMS.35,36,37 Sianos et al reported some cases of treatment failure with SESs related to stent fracture, and all fractured stents were long and post dilated with larger balloons at high pressure due to severe calcification.38 Moreover, SES implantation is expensive, especially when applied to multivessel disease requiring more than one stent. At present, cost constraints and lack of incremental reimbursement may limit the use of drug-eluting stents in daily practice in Korea.
Therefore, the present study suggests BMS implantation simultaneously with DES because of difficulty to treat all lesions by DES.
The present study has several limitations. First of all, this trial was not a blind and randomized study. Secondly, this study is based on a relatively small number of cases, raising the possibility of selection bias. Thirdly, although we confirmed that there was no difference between same system implantation and other system implantation in the restenosis rate by subgroup analysis, this result might not be reliable due to a small size of the subgroup. In addition, we did not investigate peripheral blood levels and intracoronary levels of the sirolimus after SES treatment. Despite these limitation, our study is, to our knowledge, the first clinical study demonstrating of systemic SES effect by evaluation of BMS simultaneously implanted with SES.
Ⅴ
ⅤⅤ . CONCLUSION
We evaluated systemic effect of SES by 6 months follow-up angiographic evaluation for cobalt-chromium BMS simultaneously implanted with SES in this study. Utilization of SES must be safe and effective in reducing adverse cardiac events and neointimal hyperplasia compared with BMS treatment. This study suggests that SES implantation can decrease neointimal proliferation of simultaneously implanted cobalt-chromium BMS by systemic sirolimus effect. Therefore, we must consider BMS implantation with SES as the novel PCI procedure in difficult lesions for the DES implantation.
REFEREN CES
1. Serruys PW, de Jaegere P, Kiemeneij F, Carlos M, Wolfgang R, Guy H, et al. A comparison of balloon-expandable-stent implantation with balloon angioplasty in patients with coronary artery disease. N Engl J Med 1994;331 :489-495.
2. Fishman DL, Leon MB, Baim DS, Richard AS, Michael PS, Ian P, et al.A randomized comparison of coronary stent placement and balloon angioplasty in the treatment of coronary artery disease. N Engl J Med 1994;331:496-501.
3. Nguyen-Ho P, Kaluza GL, Zymek PT, Raizner AE. Intracoronary brachy- therapy. Catheter Cardiovasc Interv 2002;56:281-288.
4. Lee MS, Singh V, Nero TJ, Wilentz JR. Cutting balloon angioplasty. J Invasive Cardiol 2002;14:552-556.
5. Belle EV, Bauter C, Hubert E, Bodart J, Abolmaali K, Meurice T, et al. Restenosis rates in diabetic patients: a comparison of coronary stenting and balloon angioplasty in native coronary arteries. Circulation 1997;96: 1454 -1460.
6. Popma JJ, Leon MB, Moses JW, Holmes DR, Cox N, Fitspatrick M, et al. Quantitative assessment of angiographic restenosis after sirolimus-eluting stent implantation in native coronary arteries. Circulation 2004;110:3773- 3780.
7. Morice MC, Serruys PW, Sousa JE, Fajadet J, Hayashi EB, Perin M, et al. A randomized comparison of a sirolimus-eluting stent with a standard stent for coronary revascularization. N Engl J Med 2002;346:1773-1780.
8. Moses JW, Leon MB, Popma JJ, Fizgerald PJ, Holmes DR, Caputo RP, et al. Sirolimus-eluting stents versus standard stents in patients in patients with stenosis in a native coronary artery. N Engl J Med 2003;349:1315-1323.
9. Farb A, Heller PF, Shroff S, Cheng L, Kolodgie FD, Carter AJ, et al. Pathological analysis of local delivery of paclitaxel via a polymer-coated stent. Circulation 2001;104:473-479.
10. Saunders RN, Metcalfe MS, Nicholson ML. Rapamycin in transplantation: a review of the evidence. Kidney Int 2001;59:3-16
11. Farb A, John M, Acampado E, Kolodgie FD, Prescott MF, Vimnami R. Oral everolimis inhibits in-stent neointimal growth. Circulation 2002;106 :2379-2384.
12. Prabhtej SB, Mehran M, Grise MG, Reilly JR, Fernandez M, Schatz RA, et al. Pilot trial of oral rapamycin for recalcitrant restenosis. Circulation 2003;107:1722-1724.
13. Dibra A, Ndrepepa G, Mehilli J, Durchinger J, Pache J, Shuhlen H, et al. Comparison of C-Reactive protein levels before and after coronary stenting and restenosis among patients treated with sirolimus-eluting versus bare metal stents. Am J Cardiol 2005;95:1238-1240.
14. Waksman R, Ajani AE, Pichard AD, Torguson R, Pinnow E, Canos D, et al. Oral rapamycin to inhibit restenosis after stenting of de novo coronary lesions: The oral rapamune to inhibit restenosis study. J Am Coll Cardiol 2004;44:1386-1392.
15. Virmani R, Farb A, Guagliumi G, Kolodgie FD. Drug-eluting stents: caution and concerns for long-term outcome. Coronary Artery Disease 2004;15: 313-318.
16. Togni M, Windecker S, Cocchia R, Wenaweser P, Cook S, Billinger M, et al. Sirolimus-eluting stents associated with paradoxic coronary vaso- constriction. J Am Coll Cariol 2005;46:231-236.
17. Klugherz BD, Lianos G, Lieuallen W, Kopia GA, Papandreou G, Narayan P, et al. Twenty-eight-day efficacy and phamacokinetics of the sirolimus -eluting stent. Coronary artery disease 2002;13:183-188.
18. Douglas P, Libby P, Bonow RO, Braunwald E. Braunwald's heart disease, 7th ed. Philadelphia: Elsevier sauders; 2005. p.1143-1145.
19. Peter WF, Castelli WP, Kannel WB. Coronary risk prediction in adults (The Framingham Study). Am J Cardiol 1987;59:91G-94G.
20. Greenland P, Gaziano JM. Selecting asymptomatic patients for coronary computed tomography or electrocardiographic exercise testing. N Engl J Med 2003;349:465-473.
21. Kuntz RE, Gibson CM, Nobuyoshi M, Baim DS. Generalized model of restenosis after conventional balloon angioplasty and new devices. J Am Coll Cardiol 1993;21:15-25.
22. Kuntz RE, Baim DS. Defining coronary restenosis: Newer clinical angio- graphic paradigms. Circulation 1993;88:1310-1323.
23. Ryan TJ, Faxon DP, Gunnar RM, Kennedy JW, King SB III, Loop FD, et al. Guidelines for percutaneous transluminal coronary angioplasty: A report of the ACC/AHA task force on assessment of diagnostic and therapeutic cardiovascular procedures J Am Coll Cardiol 1988;12:529-545.
24. Ellis SG, Vandormael MG, Cowley MJ, Disciascio G, Deligonul U, Topop EJ, et al. Coronary morphologic and clinical determinants of procedural outcome with angioplasty multivessel coronary disease: implications for patient selection. Circulation 1990;82:1193-1202.
25. Singh M, Gersh BJ, McClelland RL, Kalin KL, Willerson JT, Penny WF, et al. Clinical and angiographic predictors of restenosis after percutaneous coronary intervention. Circulation 2004;109:2727-2731.
26. Hausleiter J, Kastrati A, Mehilli J, Vogeser M, Zohlnhofer D, Schulen H, et al. Randomized, double-blind, placebo-controlled trial of oral sirolimus for restenosis prevention in patients with in-stent restenosis: the Oral Sirolimus to Inhibit Recurrent In-stent Stenosis (OSIRIS) trial. Circulation 2004;110:790-795.
27. Rodriguez AE, Alemparte MR, Vigo CF, Pereira CF, Llaurado C, Russo M, et al. Pilot study of Oral Rapamycin to Prevent Restenosis in Patients Undergoing Coronary Stent Therapy: Argentina single-center study (ORAR trial). J Invasive Cardiol 2003;15:581-584.
28. Lowe R, Menown A, Nogareda G, Penn M. Coronary stents: in these days of climate change should all stents wear coats?: Heart 2005;91:suppl 20-23.
29. Uchimura N, Perrera GB, Fujitani RM, Tobis JM, Ishimaru S, Wilson SE, et al. Dose-dependent inhibition of myointimal hyperplasia by orally administered rapamycin. Ann Vasc Surg 2004;18:172-177.
30. Jose M, Torre-Hernandez DL, Sainz-Laso F, Burgos V, Perez T, Figueroa A, et al. Comparison of c-reactive protein levels stenting with bare metal versus sirolimus eluting stents. Am J Cardiol 2005;95:748-751.
31. Holmes DR, Martin BL, Moses JW, Popma JJ, Cutlip DC, Fitzgerald PJ, et al. Analysis of 1-year clinical outcomes the SIRIUS trial. Circulation 2004;109:634-640.
32. Schofer J, Schluter M, Gershlick AH, Wijins W, Garcia E, Schampaert E, et al. Sirolimus-eluting stents for treatment of patients with long athero- sclerotic lesions in small coronary arteries. Lancet 2003; 362:1093-1099.
33. Jeremias A, Sylvia B, Bridges J, Kirtane AJ, Bigelow B, Pinto DS, et al. Stent thrombosis after successful sirolimus-eluting stent implantation. Circulation 2004;109:1930-1932.
34. Cutlip DE, Baim DS, Kalon KL, Popma JJ, Lansky AJ, Cohen DJ, et al. Stent thrombosis in the modern era: a pooled analysis of multicenter coronary stent clinical trials. Circulation 2001;103:1967-1971.
35. Ruaraidh AH, Dunder Y, Bakhai A, Rumona D, Walley T. Drug-eluting stents: an early systematic review to inform policy. European heart J 2004;25:902-919.
36. Indolfi C, Pavia M, Angelillo IF. Drug-eluting stents versus bare metal stents in percutaneous coronary interventions (a metal-analysis). Am J Cardio 2005;95:1146-1152.
37. Lemos PA, Serruys PW, van Domburg RT, Saia F, Arampatzis CA, Hoye A, et al. Unrestricted Utilization of Sirolimus-Eluting Stents Compared With Conventional Bare Stent Implantation in the "Real World": The Rapamycin-Eluting Stent Evaluated At Rotterdam Cardiology Hospital (RESEARCH) Registry. Circulation 2004;109:190-195.
38. Sianos G, Hofma S, Ligthart J, Saia F, Hoye A, Lemos PA, et al. Stent fracture and restenosis in the drug-eluting stent era. Catheterization and Cardiovascular Interventions 2004;61:111-116.
A B STRA CT(IN KOREA N ) 다혈관 관상동맥질환 환자에서의 sirolimus 약물용출 스텐트와 동시에 시술된 bare-metal 스텐트의 예후분석을 통한 약물용출 스텐트의 주변 혈관에 미치는 영향에 대한 평가 <지도교수 윤 영 원> 연세대학교 대학원 의학과 이 성 주 관상동맥질환의 중재적 치료로 관상동맥 협착 부위의 스텐트 삽입술이 보편 화되었고, sirolimus 용출 스텐트의 시술의 도입으로 재협착율을 획기적으 로 감소시켰다. sirolimus 용출 스텐트의 시술은 매우 낮은 재협착율에도 불구하고, 고가의 시술비 부담과 부작용으로 인해 다혈관 질환에서 전적 으로 sirolimus 용출 스텐트를 시술하는 데에 어려움이 있어 적절한 대책 이 필요하다. 본 연구에서는 다혈관 관상동맥질환 환자에서의 sirolimus 용출 스텐트와 동시에 시술된 cobalt-chromium BMS의 예후 분석을 통한 sirolimus 용출 스텐트의 전신적인 효과에 대해서 알아보고자 하였다. 흉 통을 주소로 내원하여 sirolimus 용출 스텐트 및 cobalt-chromium BMS시 술을 시행한 209명(238 병변)의 환자들을 대상으로 하여 연구가 진행되 었고, 6개월 후 추적관상동맥을 통하여 예후 분석을 시행하였다. BMS군 과 비교하여 SES와 BMS를 동시시술한 군에서 의미 있게 BMS의 late loss,
MLD, diameter stenosis(%)가 낮았다. 또한, binary restenosis 와 TVR 역시 의미 있게 낮았다(25/108 vs 4/40, p<0.01, 23/108 vs 4/40 p=0.01). 또한,
cobalt-chromium BMS를 SES와 같이 시술하지 않는 것은 재협착율을 증가시
키는 독립적인 인자임을 확인하였다(OR=2.154, 95% C.I.=1.179-4.959,
관상동맥에 시술한 BMS에 영향을 줄 수 있으며, 다혈관 질환을 가진 환자에 서 cobalt-chromium BMS와 sirolimus 용출 스텐트를 동시에 시술하여 좋은 예 후를 보일 수 있음을 시사한다고 하겠다.
핵심 되는 말:sirolimus용출 스텐트,cobalt-chromium BMS,신생내막세포 증 식,재협착,전신적인 효과