서론
모야모야병(Moyamoya disease)은 원인을 알 수 없는 진
행하는 만성 폐쇄성 뇌혈관질환으로, 내경동맥 말단부의
협착 및 폐색과 뇌 기저부의 이상 혈관망의 발달이 특징적
이다. 1969년 Suzuki와 Takaku [1]는 뇌혈관 조영검사에서
특징적 소견인 경동맥 말단부 협착 소견과 더불어 뇌 기저부
에서 담배연기처럼 모락모락 피어 오르는 모양의 혈관 망을
보고 ‘담배연기 모양’이라는 뜻의 일본말 표현인 모야모야라
고 명명하였다.
모야모야병은 두 개의 발병연령 패턴을 보이는데, 건강
보험심사평가원의 데이터를 분석한 자료에서는 5-9세,
50-54세[2], 한국모야회의 환우회 자료에서는 6-10세,
31-35세로(한국모야회 제공) 성인의 경우 차이를 보이는데,
이는 진단과정의 차이에 의한 것으로 판단된다. 대략 2:1의
성비로 여성의 발병률이 더 높다[3,4]. 일반적으로 모야모야
병의 유병률 및 발병률은 한국과 일본을 포함한 아시아 국가
에서 높게 보고되고 있으며[3], 모야모야병의 유병률 및 발
병률은 점진적으로 증가하고 있다[2]. 일반적인 임상증상으
로는 뇌경색(34%), 일과성 뇌허혈 발작(42%), 그리고 뇌출
혈(14%)이 있다[5]. 증상이 있는 모야모야병 환자에서 혈관
성인 모야모야병의 진단과 치료
김 정 은·방 창 환 | 서울대학교 의과대학 신경외과학교실Diagnosis and treatment of adult Moyamoya
disease
Jeong Eun Kim, md·Chang Hwan Pang, md
Department of Neurosurgery, Seoul National University College of Medicine, Seoul, Korea
Received: September 27, 2019 Accepted: October 20, 2019 Corresponding author: Jeong Eun Kim
E-mail: eunkim@snu.ac.kr © Korean Medical Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons. org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Moyamoya disease (MMD) refers to a chronic progressive steno-occlusive disease at the distal portion of the internal carotid artery with abnormal collateral vessel formation of unknown etiology. The definite diagnosis of MMD requires cerebral angiography or magnetic resonance angiography and/or magnetic resonance imaging after excluding other underlying diseases, particularly in adult patients. The treatment aims to improve regional cerebral blood flow to prevent cerebral ischemic events and alleviate hemodynamic instability that can provoke cerebral hemorrhage. Although various surgical revascularization methods have been introduced, combined revascularization surgery including direct revascularization is preferred over indirect revascularization only in adult MMD patients. Several recent studies have shown that surgical treatment has better outcomes and prognosis for symptomatic hemodynamically unstable MMD patients with both ischemic and hemorrhagic presentations. For asymptomatic patients, follow up with appropriate imaging is recommended. Surgery should be considered when new symptoms emerge with hemodynamic aggravation.
재형성 수술은 추가적인 뇌졸중을 예방하기 위한 표준치료
이다[6]. 수술은 간접혈관문합술(간접법) 또는 직접을 포함
한 복합혈관문합수술(직접법)의 방법으로 외경동맥계통 혈
류를 내경동맥계통 혈류로 전환하여 두개내 혈류를 촉진시
키는 것이다.
병인과 유전자
모야모야병의 확실한 병인은 모르나, 발병과 연관이 있을
것으로 생각되는 여러 인자들은 Table 1과 같다.
2011년도에 모야모야병에 대한 감수성 있는 유전자
로 염색체 17q25에 위치하는 ring finger 213 (RNF213)
유전자가 발견되었다[7]. 이 유전자 다형성 p.R4810K
(c.14576G>A)은 가족성 모야모야병 환자의 95%에서 확인
되었으며, 산발적으로 발생한 모야모야병 환자의 79%에서
발견되었고, 조기발병 및 모야모야병의
심한 정도와 관련 있는 것으로 생각되
어, 좋은 생체표지자 및 예후예측인자로
생각된다[8]. 하지만 이와 같은 유전자
다형성은 동아시아 일반인의 0.5-2%에
서도 존재한다[7]. 대부분의 다형성 보
인자에서 모야모야병이 발병하지 않고
[9], 다형성 p.R4810K는 동맥경화성 두
개내 동맥협착증 환자의 21%에서도 발
견되어[10], 혈관의 폐쇄성 변화를 초래
하는 공통된 소인으로 생각된다. 결론적
으로 RNF213은 모야모야병에 아직까
지는 비특이적이다.
진단
1. 진단기준
모야모야병의 일본후생노동성 진단
기준은 Table 2와 같다[11]. 임상적으로
모야모야병의 진단은 모야모야증후군
을 배제하는 일련의 과정으로 구성된다.
모야모야증후군이란 모야모야병의 혈관특징을 가지면서,
Table 2에서 기술된 다른 동반질환에 의한 것을 의미한다. 모
야모야병의 진단은 병리학적인 진단이 아니라 영상의학적 진
단으로 두개내 동맥의 협착과 폐색이 있을 때, 진성 모야모야
병으로 잘못 진단되는 경우가 많다. 특히 소아환자와는 달리
table 1. Associated factors for pathophysiology of Moyamoya disease Associate factors for Moyamoya disease
Vascular endothelial growth factor Matrix metalloproteinase-9 Hepatocyte growth factor Endothelial progenitor cell Transforming growth factor-β1 Granulocyte colony stimulating factor Interleukin-1β
Caveolin
Basic fibroblast growth factor
table 2. Diagnostic criteria for Moyamoya disease
Diagnostic criteria for Moyamoya disease
Cerebral angiography is considered essential for the diagnosis, and must show at least the following findings:
(i) Stenosis or occlusion of the terminal portion of the intracranial internal carotid artery or proximal portions of the anterior cerebral artery and/or the middle cerebral artery.
(ii) Abnormal vascular networks in the vicinity of the occlusive or stenotic lesions in the arterial phase. (iii) Bilaterality of findings (i) and (ii)
When MRI and MRA findings meet all of the following criteria, cerebral angiography can be omitted. (i) MRA shows stenosis or occlusion of the terminal portion of the intracranial internal carotid artery
or proximal portions of the anterior cerebral artery and/or the middle cerebral artery. (ii) MRA shows abnormal vascular networks in the basal ganglia.
(iii) Bilaterality of findings (i) and (ii).
Moyamoya disease is an illness of unknown etiology. The differential diagnosis of this disease includes similar cerebrovascular lesions associated with the following underlying diseases, which should,
therefore, be excluded: (i) atherosclerosis, (ii) autoimmune disease, (iii) meningitis, (iv) brain tumors, (v) Down’s syndrome, (vi) von Recklinghausen’s disease, (vii) head injury, (viii) cerebrovascular lesions after head irradiation, and (ix) others.
Pathologic findings that can be used as references for the diagnosis
(i) Thickening of the arterial intima, mainly in the terminal portion of the internal carotid arteries, and narrowing or blockage of the lumen caused by this change, usually bilateral. Occasionally, lipid
deposits are also present in the thickened intima.
(ii) Arteries such as the anterior, middle, and posterior cerebral arteries forming the circle of Willis occasionally show varying degrees of stenosis or occlusion associated with fibrocellular
thickening of the intima, waviness of the internal elastic lamina, and thinning of the media. (iii) Numerous small vascular channels (perforating and anastomotic branches) can be seen around
the circle of Willis.
(iv) Pia mater may also show reticular conglomerates of small vessels.
Adapted from Research Committee on the Pathology and Treatment of Spontaneous Occlusion of the Circle of Willis; Health Labour Sciences Research Grant for Research on Measures for Infractable Diseases. Neurol Med Chir (Tokyo) 2012;52:245-266 [11].
성인환자의 경우 모야모야증후군의 경우가 많아, 두개내 동
맥의 협착과 폐색의 소견이 보일 때, 모야모야병과의 감별진
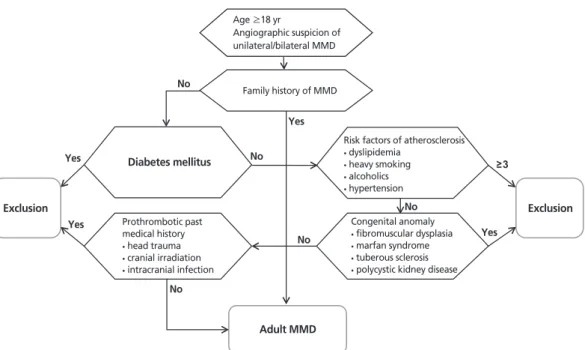
단이 중요하다. 따라서 성인 모야모야병의 진단기준은 다른
원인의 배제 원칙에 따라 Figure 1과 같다[5]. 가족력이 있다
고 하여 모야모야병을 확진할 수 있는 것은 아니나 이전의 연
구 들에서 Mineharu 등[12]은 가족성 모야모야병의 경우 상
염색체 우성 유전을 보이고 불완전 유전의 특징을 보이며, 성
인 모야모야병 환자 자녀의 약 반수에서 모야모야병이 이환
된다고 보고하였다. 따라서 혈관조영술 상 모야모야병 특징
과 더불어 모야모야병의 가족력이 있다면 확진을 할 수 있다.
가족력이 없는 환자의 경우 가능한 다른 원인을 배제한 뒤에
진단을 내릴 수 있다[5]. 이전에는 추정모야모야병으로 불렸
던 일측성 모야모야병의 경우에는, 증례가 점차 증가하고 양
측성으로 진행하는 것이 잘 알려지면서[13,14], 일본 후생노
동성 연구위원회에서 2015년 개정 발표한 모야모야병의 진
단기준에 비정상적 모야모야 혈관을 동반한 일측성 모야모야
병도 모야모야병의 진단에 포함시켰다.
2. 영상의학 및 핵의학적 평가
1) 뇌컴퓨터단층촬영
뇌의 분수령부위, 심부백질, 뇌실 주변부 또는 기저핵에서
뇌경색이나 뇌출혈을 의심하고 확인해볼 수 있으나, 뇌컴퓨
터단층촬영을 통한 진단기준은 정립되지 않아서, 일과성 뇌
허혈 발작만 있는 모야모야병 환자에서 뇌컴퓨터단층촬영을
통한 병변의 확인은 어렵다[4].
2) 뇌자기공명영상
자기공명영상혈관조영검사에서의 특징적인 내경동맥 말
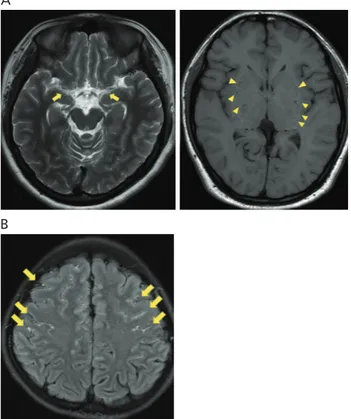
단부위의 혈관 폐색의 소견 이외에, 자기공명영상에서는 윌
리스 동맥고리의 대뇌동맥들의 신호음성이 보이지 않고, 기
저핵과 같은 뇌 심부에 모야모야 혈관에 의해 구멍이 뚫린
듯한 비정상적인 신호음성 또는 저신호강도가 다발성으로
관찰된다(Figure 2A). 울혈된 연질막 혈관의 느리고 정체되
어 있는 혈류, 또는 울혈로 인한 연수막의 비후로 인해 T1
강조영상 및 플레어영상(FLAIR)에서 연수막의 조영증강 및
연수막의 고신호강도가 관찰되는 것을 ‘담쟁이덩굴사인(ivy
sign)’이라 하여 특징적인 소견으로 판단한다[15] (Figure
2B). 혈관벽영상에 의해 모야모야병과 동맥경화에 의한 혈
관의 협착을 구분할 수 있다는 연구도 있다[16].
3) 뇌혈관조영검사
모야모야병의 진단기준인 일측 혹은 양측 내경동맥 원위
부의 협착, 폐색 및 모야모야혈관을 관찰하고 진단하는데 있
어 가장 확실한 방법이다(Figure 3). 더불어 수술이 필요할
Family history of MMD Diabetes mellitus Exclusion Exclusion Adult MMD No No No Yes Yes Yes 3 No No Yes Age ≥18 yr Angiographic suspicion of unilateral/bilateral MMDRisk factors of atherosclerosis
• dyslipidemia • heavy smoking • alcoholics • hypertension Congenital anomaly • fibromuscular dysplasia • marfan syndrome • tuberous sclerosis • polycystic kidney disease
Prothrombotic past medical history
• head trauma • cranial irradiation • intracranial infection
Figure 1. Diagnostic diagram for adult Moyamoya disease (MMD) in Seoul National University Hospital. The diagnostic criteria for adult Moyamoya disease are based on the exclusion principle. Reproduced from Kim JE et al. Neurol Med Chir (Tokyo) 2012;52:311-317, according to the Creative Commons license [5].
때, 외경동맥의 분지 및 측부순환을 파악하여 수술계획을 세
우는 데에도 중요한 검사이다. 뇌혈관조영검사 상 임상적으
로 Suzuki 병기(Suzuki stage)를 평가하기도 하는데, 이는
1969년 Suzuki와 Takaku [1]에 의해 병이 처음 기술될 때
평가했던 병기로, 후순환계의 혈관조영검사를 대부분 하지
못한 상태에서 후순환계를 평가하였다는 점, 병기를 정의할
때 환자수가 적고 대부분이 소아환자였다는 점, 정의에 의
해 정확한 병기를 매길 수 없는 경우가 많다는 점 및 혈류역
학적인 결핍 및 임상상태를 완벽하게 반영할 수 없다는 점을
고려하면, 성인 모야모야병에서 임상적으로 그 가치에는 의
문점이 있다.
4) 혈류역학적 검사
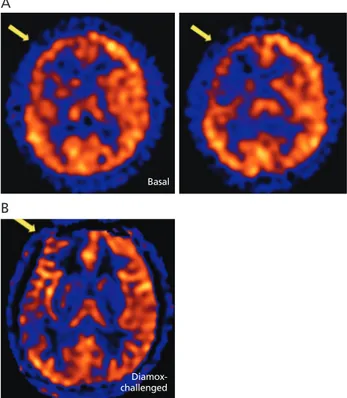
뇌혈류 및 뇌대사를 평가하기 위한 혈류역학적 검사로는
단일광자방출컴퓨터단층촬영, 제논조영증강단층촬영, 관류
컴퓨터단층촬영, 관류자기공명영상 및 양전자방출단층촬영
등이 있다. 단일광자방출컴퓨터단층촬영(Figure 4A) 및 제
논조영증강단층촬영은 국소 뇌혈류량 및 뇌혈관예비능을 측
정한다. 양전자방출단층촬영은 그 외에도 국소 산소대사율
및 국소 산소추출률을 평가한다[17]. 관류자기공명영상과 관
류컴퓨터단층촬영은 조영제 주입 후 평균통과시간과 최고점
도달시간의 지연이 있는 경우 만성허혈 상태임을 판정하게
되는데, 단일광자방출컴퓨터단층촬영, 제논조영증강단층촬
영 및 양전자방출단층촬영과 비교하여 실제 뇌조직관류량
을 반영하는데 한계가 있다. 따라서 최근 실제 뇌조직관류
량을 반영하기 위해, 관류자기공명영상에서 동맥스핀라벨링
(arterial spin-labeling) 기법(Figure 4B)이 개발되었는데,
이는 조영제를 사용하지 않아도 되며, 방사선의 노출 없이
검사를 반복적으로 시행할 수 있다는 장점이 있다[18,19].
치료
모야모야병 치료의 목표는 병인을 정상화 하는 것이 아니
라, 혈류량을 개선시켜 뇌허혈을 예방하고, 뇌출혈을 유발할
수 있는 혈류역학적 이상을 교정하는 것이다[17]. 치료 방법
은 보존치료 및 수술치료로 나누어진다.
Figure 2. The characteristics of Moyamoya disease in magnetic resonance (MR) imaging. (A) The MR imaging shows that the signal voids of the major vessels in the Circle of Willis are missing (arrows), and that there are multiple small punctate holes in the basal ganglia (arrow heads) that represents typical Moyamoya vessels. (B) FLAIR MR imaging shows multiple high signal intensi-ties at cortical sulci (arrows), called the ‘Ivy sign.’
A
B
A
B
Figure 3. The typical cerebral angiographic features of Moyamoya disease. Digital subtraction angiography shows bilateral steno-occlusive change of the terminal internal carotid artery (arrows), and characteristic collateral vessels, named as ‘Moyamoya (puff of smoke)’ (arrow heads). (A) Anteroposterior view of internal carotid angiography and (B) lateral view of internal carotid angiography.
1. 보존치료
성인 환자의 경우는 증상이 있고, 증상이 있는 부위
에 혈류역학적 검사에 의한 혈류감소가 관찰되는 경우 혈
관재형성수술을 시행하게 되며, 증상이 없거나, 혈류역학
적 이상이 뚜렷하지 않은 경우는 보존 치료를 하게 된다.
그러나, Cho 등[20]은 241명의 혈류역학적으로 안정적인
성인 모야모야병 환자를 83개월 넘게 관찰하였을 때, 연
간 뇌졸중 발생률을 4.5%로 보고하였다. 연간 뇌졸중 발
생률은 뇌출혈이 있었던 환자에서 5.7%로, 4.2%의 뇌허
혈 증상이 있었던 환자군 또는 3.4%의 무증상이었던 환
자군에 비해 높았다. 모야모야병의 가족력 및 갑상선질환
이 뇌졸중 발생의 위험인자였다. 또한, Kuroda 등[21]은
6년 이상 관찰한 결과 질병의 진행률을 약 20%로 발표하였
고, Lee 등[22]의 연구에서는 수술치료를 받은 일측성 모야
모야병 환자에서 병이 없는 반대편으로의 진행이 약 15%에
서 관찰되어, 성인 모야모야병은 진행하는 질환임이 잘 알
려져 있다. 따라서, 보존치료를 하는 성인 모야모야병 환자
들은 임상적, 영상•핵의학적 검사를 통한 추적관찰이 반
드시 필요하다. 모야모야병 환자에서 항혈소판제, 혈관확
장제, 스타틴제(statin) 등 약물치료의 효과는 증명된 바가
없다[11].
2. 수술치료(혈관재형성 수술)
혈관재형성 수술은 뇌 혈류역학적 상태를 개선시켜, 뇌경
색의 위험, 일과성 뇌허혈 발작 및 뇌출혈의 빈도를 감소시
키는데 효과적이다[23,24]. 혈관재형성 수술의 방법으로는
간접법과 직접법이 있는데, 간접법이란 혈관이 풍부한 조직
을 뇌표면에 덮어주어 신생혈관이 자라는 것을 유도하는 방
법이고, 직접법이란 외경동맥순환계의 혈관을 내경동맥순
환계의 혈관에 직접 이어줌으로써 혈류를 개통시키는 방법
을 말한다(Table 3). 대개의 경우 직접법은 간접법을 같이
하는 경우가 많아 혼합법으로 불리기도 한다.
간접법은 직접법에 비해 상대적으로 수술이 쉽고, 수술
시간이 짧으며, 과관류증후군이 드물게 발생한다. 그러나
신생혈관 형성에 시간이 필요하며, 즉각적인 혈류개선에는
효과적이지 않고, 충분한 시간이 경과한 후에도 신생혈관
형성이 일어나지 않는 경우가 있다는 점이 단점이다. 직
접법은 수술이 기술적으로 힘들고 수술시간이 상대적으로
길며 과관류현상이 많다는 점이 단점인데 비해, 수술 직후
바로 우회혈관에 의한 혈류공급이 가능하다는 점이 장점
이다.
table 3. Various revascularization surgical methods Classification Method Direct anastomosis Indirect anastomosis MCA-STA anastomosis OA-STA anastomosis STA-PCA anastomosis OA-PCA anastomosis Encephalo-duro-arterio synangiosis Encephalo-duro-arterio-galeo synangiosis Encephalo-myo synangiosis Encephalo-myo-arterio synangiosis Encephalo-duro-arterio-myo synangiosis Encephalo-galeo synangiosis
Multiple burr hole encephalo-galeo-periosteo synangiosis Omental-cerebral transposition
MCA, middle cerebral artery; STA, superficial temporal artery; PCA, posterior cere-bral artery; OA, occipital artery.
A
Basal
Figure 4. The characteristic features of a hemodynamic study in Moyamoya disease. (A) The single photon emission computed tomography and (B) mag-netic resonance arterial spin labeling imaging shows marked decreases in both the cerebrovascular reserve capacity and tissue perfusion in the right cerebral hemisphere (arrows).
Diamox-challenged B
소아환자에서는 성인 환자에 비해 수령혈관이 가늘어 직
접법이 기술적으로 더 힘들고, 간접법에 의해 신생혈관이
잘 형성되어 간접법을 주로 사용하게 된다. 반면에 성인 환
자에서는 간접법의 신생혈관 형성 및 출혈을 예방하는 효과
가 확실치 않다[25]. Mizoi 등[26]은 성인 모야모야병 환자,
특히 40세 이상에서 간접법 이후에 우회 혈관의 형성이 감
소되어 있는 것을 보고, 직접법이 주된 치료법이 되어야 한
다고 발표하였다. 또한, 성인 모야모야병에서 직접법과 간
접법의 효과를 비교한 11개의 논문에 대한 메타분석에서는
직접법이 간접법에 비해 향후 뇌졸중의 발생률을 감소시키
고, 혈관조영검사상의 혈관신생정도가 더 큰 데 비해 수술
합병증은 차이가 없음을 보였다[27]. 따라서, 성인 모야모
야병 환자에서는 두 수술법의 차이를 숙지하고, 환자의 나
이, 수술의 적응증, 질병의 상황, 수술자의 경험, 마취 및
중환자 관리의 전문가가 있는가에 따라 수술방법을 결정해
야 한다.
국민건강보험공단 자료에 따르면, 2009년부터 2013년
사이에 10,506명의 모야모야병 환자가 새롭게 진단되었
고, 같은 시기에 3,326건의 혈관재형성수술이 시행되어 대
략 31.4%의 새롭게 진단된 모야모야병 환자가 수술을 받았
다[28]. 이중에 2,157건(64.8%)은 직접법이었고, 1,169건
(35.1%)은 간접법이었으며, 직접법의 건수가 점진적으로 증
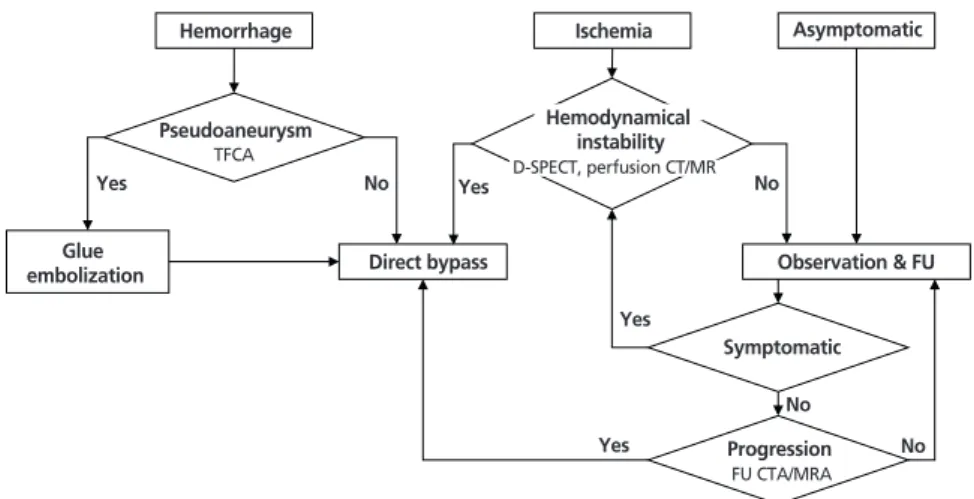
가하였다. 저자의 병원에서의 성인 모야모야병 환자의 치료
흐름도는 Figure 5와 같다.
치료성적
1. 허혈성 모야모야병 환자에서
보존치료와 비교한 수술의
결과
허혈성 성인 모야모야병 환자
에서 직접법을 받고 난 뒤, 증상
이 있는 뇌출혈 또는 뇌경색의
연간 발생위험은 각각 0.4% 및
0.2%이고, 임상적인 측면, 혈관
조영술의 측면, 혈류역학적 측면 모두에서 수술 후 6개월 뒤
호전을 보였고, 수술 후 5년까지 장기적으로 안정적이었으
며, 5년 뇌경색 및 뇌출혈 없이 생존할 확률은 98.7% 이었
다[23]. 이에 대한 반대의 결과를 보이는 연구도 있다. Jang
등[29]은 후향적 연구에서 허혈성 모야모야병 환자에서 수술
이 뇌졸중에 대한 예방효과가 없어서, 수술 후 6년째 뇌졸중
이 수술한 군의 19.2%에서, 수술을 받지 않은 군의 10.2%
에서 발생하였다고 발표하였다. 또 다른 연구에서는 성인 허
혈성 모야모야병 환자에서 5년 뇌경색 재발률은 수술 군에
서 24.4%이며, 수술을 받지 않은 군에서는 11.8%라 보고하
였다[30]. 그러나 이들 연 구들에는 한계점이 있는데, 첫째는
수술 30일 이내의 뇌졸중 발생률이 13.3-17.1%이었으며,
이것은 다른 연구의 수술 후 같은 기간 동안의 뇌졸중 발생
률에 비해 의미 있게 높았다는 점이고, 둘째는 수술방법으로
간접법만을 하였다는 점이다.
2. 출혈성 모야모야병 환자에서 보존치료와 비교한
수술의 결과
뇌출혈이 있었던 모야모야병 환자에서, 재출혈 발생률은
5년째에 16.9%, 10년째에 26.3%로 드물지 않다[31]. 출
혈성 성인 모야모야병에서 직접법의 재출혈 예방에 대한
확실한 근거는 일본 성인 모야모야병 시험(Japan Adult
Moyamoya Trial)의 결과에 있다[25]. 이 연구는 다기관,
Hemorrhage Ischemia Asymptomatic
Pseudoaneurysm TFCA Observation & FU Direct bypass Glue embolization Symptomatic Progression FU CTA/MRA Yes No Yes No Yes Yes No No Hemodynamical instability D-SPECT, perfusion CT/MR
Figure 5. Management flow sheet for adult Moyamoya disease in Seoul National University Hospital. TFCA, trans-femoral cerebral angiography; D-SPECT, Diamox-challenged single photon emission computed tomography; CT, com-puted tomography; MR, magnetic resonance image; FU, follow-up; CTA, comcom-puted tomographic angiography; MRA, magnetic resonance angiography.
전향적, 무작위 연구로서 연간 재출혈률이 수술을 한 군에
서 2.7%이며, 수술을 하지 않은 군에서 7.6%로 측정되어
직접법이 재출혈 예방에 효과가 있음을 입증하였다[25]. 따
라서 출혈성 모야모야병 환자에서 혈관재형성 수술은 향후
재출혈의 위험을 낮추는 데 있어서 효과적이다.
3. 수술 합병증
혈관재형성수술 이후에 발생하는 수술 합병증에는 뇌경
색, 뇌출혈, 경막외출혈, 경막하출혈, 과관류증후군, 뇌전증
발작, 감염, 두피의 괴사, 사망 등이 포함된다. 수술 후 영구
적인 신경학적 장애가 발생할 확률은 2.7-5.6%이고, 사망
률은 0-0.75%로 알려져 있다[23,24,32].
수술방법에 따른 수술 합병증의 발생은 큰 차이가 없다.
수술 후 발생하는 일시적인 신경학적 이상의 원인으로 주
목해야 하는 것은 과관류증후군이다[33,34]. Kim 등[33]은
수술 후 과관류증후군을 1) 수술 후 새롭게 나타난 신경학
적 이상, 2) 수술 직후엔 관찰되지 않고 수술 후 지연성으
로 나타난 신경학적 이상, 3) 15일 이내에 호전되는 가역적
신경학적 이상, 4) 뇌컴퓨터단층촬영에서 명백한 혈종 또는
확산뇌자기공명영상에서 급성 뇌경색과 같은 신경학적 이
상의 원인이 없는 경우의 네 가지 조건을 만족할 경우로 정
의하였다. 과관류증후군의 발생률은 수술을 받은 모야모야
병 환자의 17-50% 정도로 보고되고 있다[35,36]. 과관류
증후군에 대한 병인은 완전히 밝혀지지 않았으나, 만성 허
혈성 뇌 피질부위에서 상대적인 관류의 증가가 가능한 기전
으로 생각된다. 왜냐하면 특히 손이나 혀의 운동기능 이상
과 같은, 직접법의 문합부 주변의 뇌 피질 이상기능이 흔하
게 관찰되기 때문이다[33]. 새로운 혈류에 의한 분수령 영역
의 이동[37], 혈관형성인자 또는 세포외기질단백에 의한 혈
관 투과성의 증가 또한 가능한 기전이라는 보고도 있다[34].
과관류현상은 직접법 이후 자주 관찰되지만, 간접법 이후에
도 관찰된다는 발표가 있다. Cho 등[38]에 의하면 간접법
이후에도 과관류현상을 보이고, 단일광자방출컴퓨터단층촬
영에서 혈류량의 증가가 관찰이 되는 경우가 있는데, 이러
한 현상은 혈관내피성장인자 및 혈소판유래성장인자의 방
출이 국소혈관 확장 및 국소신경의 흥분에 기여하여 과관
류증후군이 발생하는 것이라 설명하였다. 과관류증후군의
치료에 대해서는 정립된 것이 아직 없으나, 엄격한 혈압조
절, 스테로이드제재, 미노사이클린(minocycline) 등이 제시
되고 있다[34,39].
결론
성인 모야모야병은 모야모야증후군과 같이 알려진 병인을
배제한 뒤 진단할 수 있으며, 혈관조영술 또는 뇌자기공명혈
관조영검사를 통해 확진할 수 있고, 일측성 모야모야병도 모
야모야병으로 진단할 수 있다. 다양한 영상, 핵의학적 검사
들을 통해 환자의 상태를 평가할 수 있다. 모야모야병의 치
료목표는 혈류량을 개선시켜 뇌허혈을 예방하고, 뇌출혈을
유발할 수 있는 혈류역학적 이상을 교정하는 것이다. 혈관재
형성수술의 방법으로는 직접법과 간접법이 있으나, 성인의
경우 직접법이 선호된다. 수술 합병증을 줄이기 위해서는 과
관류증후군의 치료와 같이 수술 이후의 치료도 중요하다. 무
증상이고 혈류역학적으로 안정한 성인 모야모야병의 경우는
일정한 간격을 두고 환자를 경과관찰하고 검사하여, 뇌졸중
발생 전에 질환의 진행을 발견하는 것이 중요하다. 특히 새
로운 증상이 발생하거나, 혈류역학적 상태가 악화된 환자의
경우 혈관재형성수술을 고려해야 한다.
찾아보기말:
진단; 치료; 성인; 모야모야병ORCID
Jeong Eun Kim, https://orcid.org/0000-0002-6927-3109 Chang Hwan Pang, https://orcid.org/0000-0002-9017-9336
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
1. Suzuki J, Takaku A. Cerebrovascular “moyamoya” disease. Disease showing abnormal net-like vessels in base of brain. Arch Neurol 1969;20:288-299.
2. Ahn IM, Park DH, Hann HJ, Kim KH, Kim HJ, Ahn HS. Incidence, prevalence, and survival of moyamoya disease in Korea: a nationwide, population-based study. Stroke 2014;45: 1090-1095.
3. Baba T, Houkin K, Kuroda S. Novel epidemiological features of moyamoya disease. J Neurol Neurosurg Psychiatry 2008;79: 900-904.
4. Scott RM, Smith ER. Moyamoya disease and moyamoya syn-drome. N Engl J Med 2009;360:1226-1237.
5. Kim JE, Kim KM, Kim JG, Kang HS, Bang JS, Son YJ, Han MH, Oh CW. Clinical features of adult moyamoya disease with special reference to the diagnosis. Neurol Med Chir (Tokyo) 2012;52:311-317.
6. Fukui M. Guidelines for the diagnosis and treatment of spon-taneous occlusion of the circle of Willis (‘moyamoya’ disease). Research Committee on Spontaneous Occlusion of the Circle of Willis (Moyamoya Disease) of the Ministry of Health and Welfare, Japan. Clin Neurol Neurosurg 1997;99 Suppl 2: S238-S240.
7. Liu W, Morito D, Takashima S, Mineharu Y, Kobayashi H, Hitomi T, Hashikata H, Matsuura N, Yamazaki S, Toyoda A, Kikuta K, Takagi Y, Harada KH, Fujiyama A, Herzig R, Krischek B, Zou L, Kim JE, Kitakaze M, Miyamoto S, Nagata K, Hashimoto N, Koizumi A. Identification of RNF213 as a susceptibility gene for moyamoya disease and its possible role in vascular development. PLoS One 2011;6:e22542.
8. Miyatake S, Miyake N, Touho H, Nishimura-Tadaki A, Kondo Y, Okada I, Tsurusaki Y, Doi H, Sakai H, Saitsu H, Shimojima K, Yamamoto T, Higurashi M, Kawahara N, Kawauchi H, Nagasaka K, Okamoto N, Mori T, Koyano S, Kuroiwa Y, Taguri M, Morita S, Matsubara Y, Kure S, Matsumoto N. Homozygous c.14576G>A variant of RNF213 predicts early-onset and severe form of moyamoya disease. Neurology 2012; 78:803-810.
9. Mikami T, Suzuki H, Komatsu K, Mikuni N. Influence of inflammatory disease on the pathophysiology of moyamoya disease and quasi-moyamoya disease. Neurol Med Chir (Tokyo) 2019 Jul 6 [Epub]. https://doi.org/10.2176/nmc.ra.2019-0059. 10. Bang OY, Chung JW, Cha J, Lee MJ, Yeon JY, Ki CS, Jeon P,
Kim JS, Hong SC. A polymorphism in RNF213 is a suscep-tibility gene for intracranial atherosclerosis. PLoS One 2016; 11:e0156607.
11. Research Committee on the Pathology and Treatment of Spontaneous Occlusion of the Circle of Willis; Health Labour Sciences Research Grant for Research on Measures for Infrac-table Diseases. Guidelines for diagnosis and treatment of moyamoya disease (spontaneous occlusion of the circle of Willis). Neurol Med Chir (Tokyo) 2012;52:245-266.
12. Mineharu Y, Takenaka K, Yamakawa H, Inoue K, Ikeda H, Kikuta KI, Takagi Y, Nozaki K, Hashimoto N, Koizumi A. Inheritance pattern of familial moyamoya disease: autosomal dominant mode and genomic imprinting. J Neurol Neurosurg Psychiatry 2006;77:1025-1029.
13. Ikezaki K, Inamura T, Kawano T, Fukui M. Clinical features of probable moyamoya disease in Japan. Clin Neurol Neurosurg 1997;99 Suppl 2:S173-S177.
14. Hayashi K, Suyama K, Nagata I. Clinical features of unilateral moyamoya disease. Neurol Med Chir (Tokyo) 2010;50:378-385.
15. Maeda M, Tsuchida C. “Ivy sign” on fluid-attenuated inver-sion-recovery images in childhood moyamoya disease. AJNR Am J Neuroradiol 1999;20:1836-1838.
16. Mossa-Basha M, de Havenon A, Becker KJ, Hallam DK, Levitt MR, Cohen WA, Hippe DS, Alexander MD, Tirschwell DL, Hatsukami T, Amlie-Lefond C, Yuan C. Added value of vessel wall magnetic resonance imaging in the differentiation of moyamoya vasculopathies in a non-asian cohort. Stroke 2016; 47:1782-1788.
17. Kim JE, Jeon JS. An update on the diagnosis and treatment of adult moyamoya disease taking into consideration contro-versial issues. Neurol Res 2014;36:407-416.
18. Lee S, Yun TJ, Yoo RE, Yoon BW, Kang KM, Choi SH, Kim JH, Kim JE, Sohn CH, Han MH. Monitoring cerebral perfusion changes after revascularization in patients with moyamoya disease by using arterial spin-labeling MR imaging. Radiology 2018;288:565-572.
19. Lee M, Zaharchuk G, Guzman R, Achrol A, Bell-Stephens T, Steinberg GK. Quantitative hemodynamic studies in moya-moya disease: a review. Neurosurg Focus 2009;26:E5.
20. Cho WS, Chung YS, Kim JE, Jeon JP, Son YJ, Bang JS, Kang HS, Sohn CH, Oh CW. The natural clinical course of hemo-dynamically stable adult moyamoya disease. J Neurosurg 2015;122:82-89.
21. Kuroda S, Ishikawa T, Houkin K, Nanba R, Hokari M, Iwasaki Y. Incidence and clinical features of disease progression in adult moyamoya disease. Stroke 2005;36:2148-2153.
22. Lee SC, Jeon JS, Kim JE, Chung YS, Ahn JH, Cho WS, Son YJ, Bang JS, Kang HS, Oh CW. Contralateral progression and its risk factor in surgically treated unilateral adult moyamoya disease with a review of pertinent literature. Acta Neurochir (Wien) 2014;156:103-111.
23. Cho WS, Kim JE, Kim CH, Ban SP, Kang HS, Son YJ, Bang JS, Sohn CH, Paeng JC, Oh CW. Long-term outcomes after combined revascularization surgery in adult moyamoya dis-ease. Stroke 2014;45:3025-3031.
24. Kim T, Oh CW, Kwon OK, Hwang G, Kim JE, Kang HS, Cho WS, Bang JS. Stroke prevention by direct revascularization for patients with adult-onset moyamoya disease presenting with ischemia. J Neurosurg 2016;124:1788-1793.
25. Miyamoto S, Yoshimoto T, Hashimoto N, Okada Y, Tsuji I, Tominaga T, Nakagawara J, Takahashi JC; JAM Trial Investi-gators. Effects of extracranial-intracranial bypass for patients with hemorrhagic moyamoya disease: results of the Japan Adult Moyamoya Trial. Stroke 2014;45:1415-1421.
26. Mizoi K, Kayama T, Yoshimoto T, Nagamine Y. Indirect revas-cularization for moyamoya disease: is there a beneficial effect for adult patients? Surg Neurol 1996;45:541-548.
Meta-analysis of the surgical outcomes of symptomatic moyamoya disease in adults. J Neurosurg 2018;128:793-799.
28. Kim T, Lee H, Bang JS, Kwon OK, Hwang G, Oh CW. Epide-miology of moyamoya disease in Korea: based on National Health Insurance Service data. J Korean Neurosurg Soc 2015; 57:390-395.
29. Jang DK, Lee KS, Rha HK, Huh PW, Yang JH, Park IS, Ahn JG, Sung JH, Han YM. Bypass surgery versus medical treatment for symptomatic moyamoya disease in adults. J Neurosurg 2017;127:492-502.
30. Noh HJ, Kim SJ, Kim JS, Hong SC, Kim KH, Jun P, Bang OY, Chung CS, Lee KH, Lee KH, Kim GM. Long term outcome and predictors of ischemic stroke recurrence in adult moya-moya disease. J Neurol Sci 2015;359:381-388.
31. Kim KM, Kim JE, Cho WS, Kang HS, Son YJ, Han MH, Oh CW. Natural history and risk factor of recurrent hemorrhage in hemorrhagic adult moyamoya disease. Neurosurgery 2017; 81:289-296.
32. Guzman R, Lee M, Achrol A, Bell-Stephens T, Kelly M, Do HM, Marks MP, Steinberg GK. Clinical outcome after 450 revascularization procedures for moyamoya disease. Clinical article. J Neurosurg 2009;111:927-935.
33. Kim JE, Oh CW, Kwon OK, Park SQ, Kim SE, Kim YK. Transient hyperperfusion after superficial temporal artery/ middle cerebral artery bypass surgery as a possible cause of postoperative transient neurological deterioration. Cerebro-vasc Dis 2008;25:580-586.
34. Fujimura M, Kaneta T, Mugikura S, Shimizu H, Tominaga T. Temporary neurologic deterioration due to cerebral hyperper-fusion after superficial temporal artery-middle cerebral artery anastomosis in patients with adult-onset moyamoya disease. Surg Neurol 2007;67:273-282.
35. Hwang JW, Yang HM, Lee H, Lee HK, Jeon YT, Kim JE, Lim YJ, Park HP. Predictive factors of symptomatic cerebral hyperperfusion after superficial temporal artery-middle cere-bral artery anastomosis in adult patients with moyamoya dis-ease. Br J Anaesth 2013;110:773-779.
36. Uchino H, Kuroda S, Hirata K, Shiga T, Houkin K, Tamaki
N. Predictors and clinical features of postoperative hyperper-fusion after surgical revascularization for moyamoya disease: a serial single photon emission CT/positron emission tomogra-phy study. Stroke 2012;43:2610-2616.
37. Heros RC, Scott RM, Kistler JP, Ackerman RH, Conner ES. Temporary neurological deterioration after extracranial-intra-cranial bypass. Neurosurgery 1984;15:178-185.
38. Cho WS, Lee HY, Kang HS, Kim JE, Bang JS, Oh CW. Symptomatic cerebral hyperperfusion on SPECT after indirect revascularization surgery for Moyamoya disease. Clin Nucl Med 2013;38:44-46.
39. Fujimura M, Niizuma K, Inoue T, Sato K, Endo H, Shimizu H, Tominaga T. Minocycline prevents focal neurological dete-rioration due to cerebral hyperperfusion after extracranial-intracranial bypass for moyamoya disease. Neurosurgery 2014;74:163-170.
Peer Reviewers’ Commentary
모야모야병은 동아시아, 특히 한국과 일본에서 발생빈도가 높은 희귀 난치성 질환이며, 국내에서 더 많은 연구가 필요한 질환이 다. 이 논문은 모야모야병의 개요, 역학, 발병기전, 임상 양상 및 수술적 치료에 대한 다양한 최신 지식을 매우 함축적으로 제시 하고 있다. 모야모야병은 소아와 성인에서 그 질환의 특성이 다 르게 나타나므로 권장되는 치료 기준 및 방법이 다르다. 이 질환 의 치료에 대한 1970~1990년대 보고는 주로 병의 진행이 빠 른 소아 환자에 대한 것이었다. 성인기 치료 기준, 특히 뇌출혈 로 발현된 경우의 치료 기준은 비교적 최근에 객관적 근거들이 보고되고 있다. 진단에 있어서 RNF213 유전자의 다형성이 임 상 경과에 미치는 영향에 대한 분석, 영상진단 방법 등 새로운 연구 결과들이 비교적 최근에 보고되었다. 이 논문은 모야모야 병의 향후 연구에 많은 도움을 줄 것으로 판단된다. [정리: 편집위원회]