저작자표시-비영리-변경금지 2.0 대한민국 이용자는 아래의 조건을 따르는 경우에 한하여 자유롭게 l 이 저작물을 복제, 배포, 전송, 전시, 공연 및 방송할 수 있습니다. 다음과 같은 조건을 따라야 합니다: l 귀하는, 이 저작물의 재이용이나 배포의 경우, 이 저작물에 적용된 이용허락조건 을 명확하게 나타내어야 합니다. l 저작권자로부터 별도의 허가를 받으면 이러한 조건들은 적용되지 않습니다. 저작권법에 따른 이용자의 권리는 위의 내용에 의하여 영향을 받지 않습니다. 이것은 이용허락규약(Legal Code)을 이해하기 쉽게 요약한 것입니다. Disclaimer 저작자표시. 귀하는 원저작자를 표시하여야 합니다. 비영리. 귀하는 이 저작물을 영리 목적으로 이용할 수 없습니다. 변경금지. 귀하는 이 저작물을 개작, 변형 또는 가공할 수 없습니다.
Doctoral Thesis in
Effect of ulinastatin on postoperative renal
function in patients undergoing
robot-assisted laparoscopic partial nephrectomy:
a randomized trial
Ajou University Graduate School
Major in Medicine
Department of Anesthesiology
Bora Lee
Effect of ulinastatin on postoperative renal
function in patients undergoing
robot-assisted laparoscopic partial nephrectomy:
a randomized trial
Supervised by
Sook Young Lee, M.D., Ph.D.
A Dissertation Submitted to The Graduate School of Ajou University in
Partial Fulfillment of the Requirements for The Degree of Ph.D. in
Medicine
Ajou University Graduate School
Major in Medicine
Department of Anesthesiology
Bora Lee
This certifies that the doctoral dissertation
of Bora Lee is hereby approved.
SUPERVISORY COMMITTEE
________________________
Committee President : Jin Soo Kim
________________________
Member : Sook Young Lee
________________________
Member : Wyun Kon Park
________________________
Member : Yun Jeong Chae
________________________
Member : Ji Eun Kim
Ajou University Graduate School
December, 22, 2017
ACKNOWLEDGEMENTS
This dissertation could not be fructified without the supports, advices,
and encouragements of many people and colleagues. I would like to
express my gratitude to those who have contributed to this work in
various ways.
First of all, I’d like to thank all patients who generously decided to
participate in this study.
I would also like to express sincere gratitude to my thesis supervisor,
Professor Sook Young Lee, who provided the best tutelage and support
possible and allowed me to develop. I am also grateful to Professor Jin
Soo Kim, Professor Wyun Kon Park, Professor Yun Jeong Chae and
Professor Ji Eun Kim for their encourage and constructive comments
throughout my years at graduate school.
Likewise, I sincerely thank Professor So Yeon Kim, who, despite my
lack of knowledge and experience on a thesis at the start of the doctoral
degree program, gave me advice and guidance in many ways during the
writing of this paper.
Lastly, my family always gave me love, support and encouragement,
and I would like to thank all of them.
i
ABSTRACT
Effect of ulinastatin on postoperative renal function in patients
undergoing robot-assisted laparoscopic partial nephrectomy: a
randomized trial
Background: Robot-assisted laparoscopic partial nephrectomy (RLPN) is an emerging technique for treating small renal masses. Although RLPN has many advantages, ischemic kidney injury is inevitable during renal artery clamping. The overall incidence of acute kidney injury (AKI) after partial nephrectomy has been reported to be up to 39%. Moreover, effective pharmacological protection against AKI after partial nephrectomy has not yet been demonstrated. Ulinastatin has been shown to protect the kidney from ischemia/reperfusion injury via its anti-inflammatory and anti-oxidant activities. Therefore, this study aimed to evaluate the effect of ulinastatin on postoperative kidney function in patients undergoing RLPN. Methods: In this randomized, double-blinded, placebo-controlled study, patients undergoing RLPN received either intravenous ulinastatin (100,000 units/10 kg; ulinastatin group, n=35) or the same volume of normal saline (control group, n=35) for 1 h starting 10 min before renal artery clamping. The primary outcome was incidence of postoperative AKI. Secondary outcomes were levels of serum creatinine, estimated glomerular filtration rate (eGFR), cystatin C, and inflammatory markers
ii
and were measured before operation and at 1, 24, 48, and 72 h postoperatively. Results: The incidence of postoperative AKI was 18% in the ulinastatin group, whereas it was 30% in the control group (p=0.251). No significant differences in postoperative changes of serum creatinine, eGFR, or cystatin C were observed between the two groups. Postoperative inflammatory markers including C-reactive protein, white blood cell count, and neutrophil percentage were significantly increased until 72 h after operation compared to the preoperative values in both groups, with no significant differences between the groups.
Conclusions: Administration of ulinastatin (100,000 units/10 kg) during the warm ischemia and reperfusion periods did not show any beneficial effects on postoperative kidney function or inflammatory responses in patients undergoing RLPN.
Key words: acute kidney injury; nephrectomy; reperfusion injury; robotic surgical procedures; ulinastatin
iii
TABLE OF CONTENTS
ABSTRACT ... i
TABLE OF CONTENTS ... iii
LIST OF FIGURES ... iv
LIST OF TABLES ... v
I. INTRODUCTION ... 1
II. METHODS ... 3
1. Interventions ... 3
2. Data collection ... 4
3. Statistical analysis ... 6
III. RESULTS ... 7
IV. DISCUSSION ... 14
V. REFERENCES ... 20
iv
LIST OF FIGURES
Figure 1. Consort diagram flowchart ... 9
Figure 2. Changes in (A) serum creatinine level, (B) estimated
glomerular filtration rate (eGFR), and (C) cystatin C level during the
first 72 h after operation. ... 12
v
LIST OF TABLES
Table 1. Patient characteristics and intraoperative variables 10
Table 2. Postoperative kidney function parameters ... 11
Table 3. Perioperative changes in inflammatory markers….13
1
I. INTRODUCTION
Robot-assisted laparoscopic partial nephrectomy (RLPN) is an emerging technique for treating small renal masses [1]. The advantages of RLPN are stable motion without tremor and easier and more precise resection and repair compared with laparoscopic partial nephrectomy, all of which may reduce postoperative complications [1]. Nevertheless, renal artery clamping, which causes ischemic kidney injury, is inevitable during RLPN in most cases [2]. Although the incidence of acute kidney injury (AKI) after RLPN has not been analyzed, the overall
incidence of AKI after partial nephrectomy has been reported to be up to 39% [3, 4]. Since postoperative renal insufficiency is an independent predictor of overall and cardiovascular-specific survival after nephrectomy [5], several methods such as cold ischemia using ice, remote ischemia preconditioning, and unclamping technique have been investigated to reduce ischemic kidney injury in laparoscopic partial nephrectomy and RLPN [6-8]. Pharmacological protection with mannitol or fenoldopam has also been investigated; however, these therapeutics were not effective in preserving kidney function after partial nephrectomy [9-11].
Ulinastatin is a glycoprotein found in urine and inhibits various proteases,
including trypsin, chymotrypsin, elastase, and pancreatic enzymes [12]. Ulinastatin also inhibits the release of neutrophil elastase, secretion of proinflammatory cytokines, and production of oxygen free radicals [13-17]. Due to its
anti-2
inflammatory and anti-oxidant activities, ulinastatin has shown protective effects against ischemia/reperfusion injury in many organs, including the brain, heart, lung, and liver [13-19]. Ulinastatin was also shown to significantly reduce the serum creatinine elevation and kidney ultrastructure damage produced by renal ischemia -reperfusion [20]. Moreover, ulinastatin has been shown to reduce the incidence of AKI after cardiac surgery and liver transplantation [21, 22]. However, no data have yet been obtained regarding the efficacy of ulinastatin for renal protection in partial nephrectomy.
Therefore, this randomized, double-blinded, placebo-controlled study aimed to evaluate the effect of ulinastatin on postoperative kidney function in patients undergoing RLPN.
3
II. METHODS
This study was approved by the Institutional Review Board (protocol number: 4-2014-0633) and was registered at ClinicalTrials.gov (NCT02258906). We enrolled 70 consecutive patients, aged 20-79 years with an American Society Anesthesiologist physical status I to III, who were scheduled to undergo elective RLPN for renal mass between October 2014 and July 2016. Written informed consent was obtained from all patients before randomization. The exclusion criteria were severe respiratory or cardiovascular disease, preoperative serum creatinine >2 mg/dL, and preoperative C-reactive protein (CRP) >10 mg/L.
1. Interventions
Patients were randomly allocated to either the ulinastatin group (n=35) or the control group (n=35) by computer-generated randomization table
(http://www.random.org). Randomization and group assignment were performed by an anesthesiologist who did not participate in the data collection. The ulinastatin group received 100,000 units/10kg of ulinastatin [23] (Ulistin, 100,000 units/2 mL, Hanlim Pharm. Co., Ltd, Seoul, Korea). For infusions, the ulinastatin was diluted with normal saline to a total volume of 50 mL. The solution was infused for 1 h starting 10 min before renal artery clamping. The control group received an
4
equivalent volume of normal saline infusion as a placebo. All study medications were prepared in syringes of identical appearance by an anesthesiologist who did not participate in the data collection. The investigator, attending anesthesiologists, surgeons, and patients were all blinded to group assignment.
Anesthesia was induced with 2 mg/kg of propofol (Fresofol MCT 1 %, Fresenius Kabi Korea Ktd, Seoul, Korea), 1.2 mg/kg of rocuronium (Esmeron, MSD Korea Ltd, Seoul, Korea), and 0.5-1 µg/kg of remifentanil (Ultiva, GlaxoSmithKline Korea, Seoul, Korea). Subsequently, a radial artery catheter was inserted, and a peripheral line was placed via the external jugular vein. Anesthesia was maintained with desflurane 0.8-1 age-adjusted minimal alveolar concentration in 50% O2/air and remifentanil 0.05-0.15 µg/kg/min. Hypotension, defined as a decrease in mean arterial pressure >20% from the preoperative value, was treated with intravenous ephedrine at 4 mg increments.
After a nasogastric tube and a 16 F urethral catheter were inserted, the patient was placed in the semilateral position. RLPN was preformed transperitoneally with the da Vinci robot system (Intuitive Surgical Inc., Sunnyvale, CA, USA) and carbon dioxide pneumoperitoneum (12-15 mmHg). All surgical procedures were performed as previously reported [24]. The renal hilar vessels were clamped with laparoscopic bulldog clamps through the assistant port without application of ice (warm ischemia).
5
The primary outcome of this study was incidence of AKI, defined as an abrupt (within 48 h) reduction in kidney function. Reduction in kidney function was defined as an absolute increase in serum creatinine level ≥0.3 mg/dL, a 50% (1.5-fold) increase in serum creatinine level from baseline, or a reduction in urine output (documented oliguria <0.5 mL/kg/h for >6 h) [25]. AKI was further classified into three stages according to the Acute Kidney Injury Network (AKIN) classification: stage 1, increase in serum creatinine level ≥0.3 mg/dL or increase ≥150-200% (1.5-2.0-fold) from baseline; stage 2, increase in serum creatinine level >200-300% (>2–3-fold) from baseline; and stage 3, increase in serum creatinine level >300% (>3-fold) from baseline [25]. The secondary outcomes were estimated glomerular filtration rate (eGFR), cystatin C level, and various postoperative inflammatory markers (CRP, white blood cell [WBC] count, neutrophil percentage).
Serum creatinine, eGFR, cystatin C, CRP, WBC count, and neutrophil percentage were measured before operation (baseline) and at 1, 24, 48, and 72 h
postoperatively. eGFR was calculated by the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation [26]. If the patient was discharged before 72 h after operation, these values were assessed only until 48 h after operation.
Nephrometry scores were generated by the R.E.N.A.L.-Nephrometry scoring system (www.Nephrometry.com) [27].
6
3. Statistical analysis
Sample size was determined by serum creatinine level, since the incidence of AKI after RLPN was not known, and the serum creatinine level was used in the definition of AKI. We considered a serum creatinine decrease ≥0.2 mg/dL in the ulinastatin group compared to the control group to be clinically relevant [28]. With a
significance level of 5% and a power of 80%, 32 subjects were required in each group. We included 35 patients per group to allow for a 10% dropout rate. All values are expressed as mean ± standard deviation (SD), median (interquartile range), or number of patients. Parametric data were analyzed using the independent t-test, whereas nonparametric data were analyzed using the Mann–Whitney U test. Categorical variables were evaluated using the χ2 test or Fisher’s exact test, as appropriate. Repeatedly measured variables were analyzed by a linear mixed model with group, time, and group-by-time as fixed effects; post hoc analysis was performed with Bonferroni correction to adjust for multiple comparisons. A P value <0.05 was considered statistically significant. All analyses were performed using SPSS 22.0 (IBM, Armonk, NY, USA) and SAS 9.4 (SAS Inc., Cary, NC, USA).
7
III. RESULTS
Of the 72 patients assessed for eligibility, 70 were enrolled and randomly assigned to groups. Of these 70 patients, 66 (94%) completed the study (Fig. 1). Four patients were excluded because of changes in surgical methods: an
unclamping method was used in two patients, and conversion to radical nephrectomy was performed in two patients. The patient characteristics and intraoperative variables were similar between the groups (Table 1).
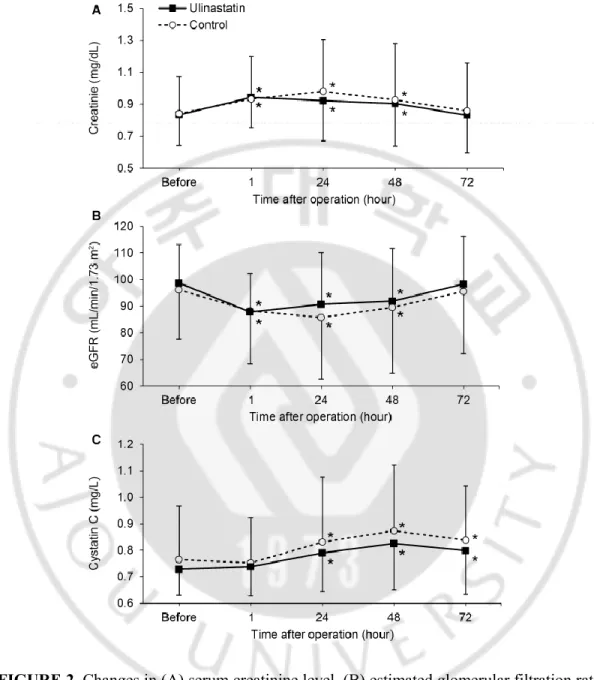
The incidence of postoperative AKI was 18% in the ulinastatin group, whereas it was 30% in the control group (p=0.251; Table 2). All patients with AKI were in AKIN classification stage I. Urine output during the first 48 h postoperatively was similar between the groups, and no patients had oliguria within the same time period (Table 2). No significant differences in postoperative changes of serum creatinine, eGFR, or cystatin C level were observed between the two groups (Fig. 2). The highest serum creatinine level during the first 48 h postoperatively was 1.00 ± 0.24 mg/dL in the ulinastatin group and 1.03 ± 0.33 mg/dL in the control group (p=0.750). The postoperative serum creatinine increase and eGFR decrease both recovered to preoperative values within 72 h postoperatively in both groups.
The postoperative inflammatory markers (CRP, WBC count, and neutrophil percentage) were significantly increased until 72 h postoperatively compared to their preoperative values in both groups; no significant differences were observed
8
between the groups (Table 3).
No surgical complications occurred in either group. The postoperative hospital stay (median [IQR]) was 4 (3-6) days in the ulinastatin group and 4 (4-6) days in the control group (p=0.192).
9 FIGURE 1. Consort diagram flowchart.
10
Table 1. Patient characteristics and intraoperative variables
Values are expressed as mean ± SD, median (interquartile range), or number of patients. Ulinastatin (n=33) Control (n=33) p value
Age (years) 49 ± 9 52 ± 12 0.179 BMI (kg/m2) 24.7 ± 3.2 25.2 ± 3.8 0.592 Sex (male/female) 22/11 23/10 0.792 Coexisting disease Hypertension 11 8 0.415 Diabetic mellitus 3 5 0.708 Tumor size (cm) 3.4 ± 1.6 3.7 ± 1.3 0.409 Nephrometry score 8 (7-9) 7 (6-10) 0.645
Duration of pneumoperitoneum (min) 129 ± 25 134 ± 36 0.516 Duration of operation (min) 161 (148-183) 174 (143-192) 0.577 Duration of warm ischemia (min) 24.2 ± 6.3 24.9 ± 6.3 0.653 Intraoperative fluid intake (mL) 1500 (1250-2150) 1700 (1200-2250) 0.748 Crystalloid 1000 (750-1650) 1200 (750-1675) 0.743
Colloid 500 (500-500) 500 (500-575) 0.408
Intraoperative urine output (mL) 450 (175-700) 600 (295-800) 0.202 Intraoperative blood loss (mL) 150 (100-400) 100 (100-500) 0.907 Intraoperative dose of remifentanil
(μg)
860 (605-963) 760 (655-927) 0.710
Pathology
Clear cell renal cell carcinoma 24 27 0.378
Papillary renal cell carcinoma 4 2 0.672
Chromophobe renal cell carcinoma 2 0 0.492
11 Table 2. Postoperative kidney function parameters
Ulinastatin (n = 33)
Control (n = 33)
p value
Acute kidney injury 6 10 0.251 0-24 h postoperation urine output (mL) 1998 ± 501 2074 ± 613 0.583 24-48 h postoperation urine output (mL) 2157 ± 721 1947 ± 665 0.233 Oliguria within 48 h postoperationa 0 0 >0.999 Values are expressed as mean ± SD or number of patients.
12
FIGURE 2. Changes in (A) serum creatinine level, (B) estimated glomerular filtration rate (eGFR), and (C) cystatin C level during the first 72 h after operation. Values are expressed as mean ± SD. No differences were found between the groups. *p <0.05 versus ‘before operation’ in each group (Bonferroni-corrected).
13
Table 3. Perioperative changes in inflammatory markers
Values are expressed as mean ± SD or median (interquartile range).
a‘72 h postoperation’ values include data from only 31 patients in the ulinastatin group and
26 patients in the control groupbecause of discharge before 72 h postoperation.
bBetween-group comparison (Bonferroni-corrected). *p <0.01 versus ‘before operation’ in
each group (Bonferroni-corrected).
Ulinastatin (n=33) Control (n=33) Adjusted p valueb C-reactive protein (mg/L) Before operation 0.7 (0.5-1.1) 1.0 (0.5-1.7) 0.615 1 h postoperation 0.8 (0.4-1.1) 0.8 (0.4-1.6) >0.999 24 h postoperation 28.6 (14.6-40.7)* 27.9 (15.1-34.9)* >0.999 48 h postoperation 79.2 (37.4-110.7)* 77.7 (56.8-109.1)* >0.999 72 h postoperationa 87.6 (42.2-133.4)* 116.9 (86.6-141.8)* 0.110 White blood cell count (/µL)
Before operation 6646 ± 1553 6287 ± 1699 >0.999 1 h postoperation 14934 ± 3505* 14447 ± 4275* >0.999 24 h postoperation 10012 ± 2221* 10272 ± 3559* >0.999 48 h postoperation 10085 ± 3209* 10459 ± 3155* >0.999 72 h postoperationa 8743 ± 2559* 8932 ± 2625* >0.999 Neutrophil percentage (%) Before operation 58.6 ± 8.1 59.1 ± 8.4 >0.999 1 h postoperation 85.4 ± 5.6* 85.2 ± 6.5* >0.999 24 h postoperation 81.0 ± 5.6* 81.7 ± 5.8* >0.999 48 h postoperation 78.4 ± 5.2* 79.6 ± 5.7* >0.999 72 h postoperationa 72.9 ± 7.8* 75.1 ± 5.5* >0.999
14
IV. DISCUSSION
This randomized study was the first trial to investigate the effects of intraoperative administration of ulinastatin on kidney function after partial nephrectomy. Administration of ulinastatin 100,000 units/10kg did not significantly reduce the incidence of postoperative AKI following RLPN. In addition, this treatment did not show any beneficial effects on serum biomarkers of kidney function or inflammatory responses.
The incidence of AKI after partial nephrectomy has been reported to range from 9% to 39% [3, 4], which is much higher than the 1% incidence reported after noncardiac surgery [29, 30]. RLPN was introduced relatively recently and has been shown to be superior to laparoscopic partial nephrectomy with respect to improving warm ischemia time and complications [1]. However, even RLPN is unable to avoid kidney injury caused by warm ischemia [1]. Patients with postoperative AKI had a 4.2-fold higher risk of new-onset chronic kidney disease 3 years after nephrectomy [31]. Postoperative AKI is also associated with increased all-cause mortality after nephrectomy as well as general surgery [5, 29, 30]; therefore, it is important to prevent AKI. Several trials have been conducted to reduce ischemic kidney injury in laparoscopic partial nephrectomy and RLPN. One study showed that intracorporeal renal hypothermia using ice slush was technically feasible during RLPN and yielded a 12.9% greater preservation of eGFR on postoperative days 1-3 compared to the conventional warm ischemia method [6]. Remote ischemia preconditioning using
15
transient lower limb ischemia has also shown favorable results in terms of eGFR measured at 1 month after laparoscopic partial nephrectomy. Specifically, the decrease of eGFR was 15% in the control group versus 8.8% in the remote ischemia preconditioning group [7]. However, these two methods did not show any beneficial effects at 6 months after surgery [6, 7]. The unclamping method has been shown to be safe and feasible in RLPN, with shorter operative times and smaller decreases in eGFR within the first 6 months after surgery; however, this method was associated with higher blood loss [8]. Pharmacological intervention with mannitol or fenoldopam did not preserve kidney function in open or minimally invasive partial nephrectomy [9-11]. There is currently no consensus regarding the most appropriate renal protection method in RLPN [32].
Ulinastatin is a glycoprotein and a nonspecific protease inhibitor found in urine [12]. Ulinastatin has been shown to have protective effects against ischemia/reperfusion injury to various organs in clinical and experimental studies [13-20]. These protective effects were mediated by a reduction of the inflammatory response by suppressing neutrophil infiltration, neutrophil elastase release, and proinflammatory cytokine release [13-16, 18, 20, 22]. In addition to its anti-inflammatory properties, ulinastatin has anti-oxidant and anti-apoptotic properties [14, 17, 20, 22]. Moreover, ulinastatin has been shown to exert myocardial protective effects by preventing mitochondrial dysfunction and maintaining energy production in a rat model of hemorrhagic shock [33]. Of particular note, ulinastatin has shown
16
renal protective effects in both experimental and clinical studies [20-22]. Administration of ulinastatin prior to renal ischemia and at the beginning of reperfusion has been shown to reduce the creatinine elevation and renal ultrastructure damage following ischemia-reperfusion injury in rats [20]. Moreover, a bolus intravenous administration of ulinastatin 500,000 units after induction of anesthesia was shown to reduce the incidence of AKI and renal replacement therapy after cardiac surgery with cardiopulmonary bypass [21]. In multivariate logistic regression analysis, the administration of ulinastatin was found to be beneficial for protecting against AKI after cardiac surgery (odds ratio 0.71, 95 % confidence interval 0.56– 0.90, P = 0.005) [21]. Li et al. demonstrated the renal protective effects of ulinastatin in both clinical and experimental settings of orthotopic liver transplantation [22]. In the clinical setting, patients who received intravenous ulinastatin 5,000-8,000 U/kg during the skin incision and a repeated dose at 4 h into surgery showed lower incidence of AKI, lower serum cystatin C level, and lower serum and urinary β2 microglobulin levels following liver transplantation. Furthermore, intensive care unit length of stay and duration of mechanical ventilation were reduced in patients receiving ulinastatin. In the experimental setting with rats, ulinastatin application was shown to reduce renal pathological damage and elevation of serum cystatin C and creatinine levels following liver transplantation by inhibiting inflammation reactions and oxidative stress. However, in contrast to the favorable results mentioned above, administration of ulinastatin (1,000,000 units) had no cardiac or
17
renal protective effects in patients undergoing aortic valve replacement with cardiopulmonary bypass [34].
We determined the dose of ulinastatin based on a previous study of patients undergoing liver resection. In this study, a single dose of ulinastatin (100,000 units/10 kg) given before allogenic blood transfusion reduced the risk of systemic inflammatory response syndrome and the release of proinflammatory cytokines associated with intraoperative blood transfusion [23]. This dose is comparable to those used in previous studies demonstrating renal protective effects of ulinastatin in cardiac surgery (500,000 units, administered once) and liver transplantation (5,000-8,000 units/kg, administered twice) [21, 22]. However, in the current study, administration of ulinastatin 100,000 units/10 kg did not show renal protective effects or anti-inflammatory effects in patients undergoing RLPN. One possible explanation for the lack of observed protective effects of ulinastatin in our study might be that our patients had less severe ischemic injury and weaker inflammatory responses in RLPN (all of our patients with AKI were AKIN classification stage I) compared to previous studies of patients undergoing cardiac surgery or liver transplantation [21, 22]. Although it was not statistically significant, the AKI incidence tended to be lower in the ulinastatin group (18.2%) than in the control group (30.3%), and the CRP level at 72 h postoperation tended to be lower in the ulinastatin group (87.6 [42.2-133.4], median [IQR]) than in the control group (116.9 [86.6-141.8]). Further studies enrolling more patients are needed to reach more
18
definite conclusions regarding the effects of ulinastatin in RLPN.
There are some limitations to our study. First, we included patients with a preoperative serum creatinine level <2 mg/dL. The highest level of preoperative serum creatinine was 1.35 mg/dL in the ulinastatin group and 1.50 mg/dL in the control group. Further studies are needed in patients with preoperative kidney function impairment, a solitary kidney, old age (≥56 years), and diabetes mellitus who may be more susceptible to AKI [30, 35]. Second, sample size was determined by serum creatinine level instead of the incidence of AKI since there was no prior pilot study to guide the power calculation. Therefore, the reason for no significant difference in AKI between the ulinastatin and control groups (18% vs. 30%) can be a chance of type II error. Further study with large number of patients is needed for definitive conclusion. Third, we administered ulinastatin as a single dose. Specifically, we infused ulinastatin for 1 h starting 10 min before renal artery clamping to cover the warm ischemia and reperfusion periods. Since the mean duration of warm ischemia was 24.2 min and the longest warm ischemia time was 39.2 min in the ulinastatin group, all patients could receive ulinastatin during the renal ischemia and reperfusion periods. However, since serum creatinine was elevated compared to the baseline value until 2 days after RLPN, repeated administration of ulinastatin in the immediate postoperative period might better preserve kidney function.
19
ischemia and reperfusion periods did not show any beneficial effects on postoperative kidney function or inflammatory responses in patients undergoing RLPN. Further studies with a large number of patients or a higher dose may be needed for the definite conclusion of the effects of ulinastatin on postoperative kidney function after partial nephrectomy.
20
V. REFERENCES
1. Shiroki R, Fukami N, Fukaya K, Kusaka M, Natsume T, Ichihara T, Toyama H (2016) Robot-assisted partial nephrectomy: Superiority over laparoscopic partial nephrectomy. Int J Urol 23(2):122-131.
2. Zargar H, Akca O, Ramirez D, Brandao LF, Laydner H, Krishnan J, Stein RJ, Kaouk JH (2015) The impact of extended warm ischemia time on late renal function after robotic partial nephrectomy. J Endourol 29(4):444-448.
3. Rajan S, Babazade R, Govindarajan SR, Pal R, You J, Mascha EJ, Khanna A, Yang M, Marcano FD, Singh AK, Kaouk J, Turan A (2016) Perioperative factors associated with acute kidney injury after partial nephrectomy. Br J Anaesth 116(1):70-76.
4. Takagi T, Kondo T, Iizuka J, Tomita E, Kobayashi H, Hashimoto Y, Tanabe K (2012) Predictors for postoperative renal function after open partial nephrectomy: including postoperative biomarkers. Int J Urol 19(9):823-828.
5. Weight CJ, Larson BT, Fergany AF, Gao T, Lane BR, Campbell SC, Kaouk JH, Klein EA, Novick AC (2010) Nephrectomy induced chronic renal insufficiency is
associated with increased risk of cardiovascular death and death from any cause in patients with localized cT1b renal masses. J Urol 183(4):1317-1323.
6. Ramirez D, Caputo PA, Krishnan J, Zargar H, Kaouk JH (2016) Robot-assisted partial nephrectomy with intracorporeal renal hypothermia using ice slush: step-by-step technique and matched comparison with warm ischaemia. BJU Int 117(3):531-536.
21
7. Huang J, Chen Y, Dong B, Kong W, Zhang J, Xue W, Liu D, Huang Y (2013) Effect of remote ischaemic preconditioning on renal protection in patients undergoing laparoscopic partial nephrectomy: a 'blinded' randomised controlled trial. BJU Int 112(1):74-80.
8. Kaczmarek BF, Tanagho YS, Hillyer SP, Mullins JK, Diaz M, Trinh QD, Bhayani SB, Allaf ME, Stifelman MD, Kaouk JH, Rogers CG (2013) Off-clamp robot-assisted partial nephrectomy preserves renal function: a multi-institutional propensity score analysis. Eur Urol 64(6):988-993.
9. Power NE, Maschino AC, Savage C, Silberstein JL, Thorner D, Tarin T, Wong A, Touijer KA, Russo P, Coleman JA (2012) Intraoperative mannitol use does not improve long-term renal function outcomes after minimally invasive partial nephrectomy. Urology 79(4):821-825.
10. O'Hara JF, Jr., Mahboobi R, Novak SM, Bonilla AM, Mascha EJ, Fergany AF, Campbell SC, Kaouk JH, Kaple KM, Gill IS, Ziegman SA, Sessler DI (2013) Fenoldopam and renal function after partial nephrectomy in a solitary kidney: a randomized, blinded trial. Urology 81(2):340-345.
11. Omae K, Kondo T, Takagi T, Iizuka J, Kobayashi H, Hashimoto Y, Tanabe K (2014) Mannitol has no impact on renal function after open partial nephrectomy in solitary kidneys. Int J Urol 21(2):200-203.
12. Umeadi C, Kandeel F, Al-Abdullah IH (2008) Ulinastatin is a novel protease inhibitor and neutral protease activator. Transplant Proc 40(2):387-389.
22
13. Bingyang J, Jinping L, Mingzheng L, Guyan W, Zhengyi F (2007) Effects of urinary protease inhibitor on inflammatory response during on-pump coronary revascularisation. Effect of ulinastatin on inflammatory response. J Cardiovasc Surg (Torino) 48(4):497-503.
14. Koga Y, Fujita M, Tsuruta R, Koda Y, Nakahara T, Yagi T, Aoki T, Kobayashi C, Izumi T, Kasaoka S, Yuasa M, Maekawa T (2010) Urinary trypsin inhibitor suppresses excessive superoxide anion radical generation in blood, oxidative stress, early
inflammation, and endothelial injury in forebrain ischemia/reperfusion rats. Neurol Res 32(9):925-932.
15. Xu CE, Zou CW, Zhang MY, Guo L (2013) Effects of high-dose ulinastatin on inflammatory response and pulmonary function in patients with type-A aortic dissection after cardiopulmonary bypass under deep hypothermic circulatory arrest. J Cardiothorac Vasc Anesth 27(3):479-484.
16. Wu YJ, Ling Q, Zhou XH, Wang Y, Xie HY, Yu JR, Zheng SS (2009) Urinary trypsin inhibitor attenuates hepatic ischemia-reperfusion injury by reducing nuclear factor-kappa B activation. Hepatobiliary Pancreat Dis Int 8(1):53-58.
17. Liu B, Huang W, Xiao X, Xu Y, Ma S, Xia Z (2015) Neuroprotective Effect of Ulinastatin on Spinal Cord Ischemia-Reperfusion Injury in Rabbits. Oxid Med Cell Longev 2015:624819.
18. Yano T, Anraku S, Nakayama R, Ushijima K (2003) Neuroprotective effect of urinary trypsin inhibitor against focal cerebral ischemia-reperfusion injury in rats.
23 Anesthesiology 98(2):465-473.
19. Cao ZL, Okazaki Y, Naito K, Ueno T, Natsuaki M, Itoh T (2000) Ulinastatin attenuates reperfusion injury in the isolated blood-perfused rabbit heart. Ann Thorac Surg 69(4):1121-1126.
20. Chen CC, Liu ZM, Wang HH, He W, Wang Y, Wu WD (2004) Effects of ulinastatin on renal ischemia-reperfusion injury in rats. Acta Pharmacol Sin 25(10):1334-1340.
21. Wan X, Xie X, Gendoo Y, Chen X, Ji X, Cao C (2016) Ulinastatin administration is associated with a lower incidence of acute kidney injury after cardiac surgery: a
propensity score matched study. Crit Care 20:42.
22. Li X, Li X, Chi X, Luo G, Yuan D, Sun G, Hei Z (2015) Ulinastatin ameliorates acute kidney injury following liver transplantation in rats and humans. Exp Ther Med 9(2):411-416.
23. Shu H, Liu K, He Q, Zhong F, Yang L, Li Q, Liu W, Ye F, Huang W (2014) Ulinastatin, a protease inhibitor, may inhibit allogeneic blood transfusion-associated pro-inflammatory cytokines and systemic pro-inflammatory response syndrome and improve postoperative recovery. Blood Transfus 12 Suppl 1:s109-118.
24. Jeong W, Park SY, Lorenzo EI, Oh CK, Han WK, Rha KH (2009) Laparoscopic partial nephrectomy versus robot-assisted laparoscopic partial nephrectomy. J Endourol 23(9):1457-1460.
24
C, Shah SV (2007) Improving outcomes of acute kidney injury: report of an initiative. Nat Clin Pract Nephrol 3(8):439-442.
26. Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF, 3rd, Feldman HI, Kusek JW, Eggers P, Van Lente F, Greene T, Coresh J (2009) A new equation to estimate glomerular filtration rate. Ann Intern Med 150(9):604-612.
27. Kutikov A, Uzzo RG (2009) The R.E.N.A.L. nephrometry score: a
comprehensive standardized system for quantitating renal tumor size, location and depth. J Urol 182(3):844-853.
28. Cho JE, Shim JK, Chang JH, Oh YJ, Kil HK, Rha KH, Kwak YL (2009) Effect of nicardipine on renal function after robot-assisted laparoscopic radical prostatectomy. Urology 73(5):1056-1060.
29. Kheterpal S, Tremper KK, Englesbe MJ, O'Reilly M, Shanks AM, Fetterman DM, Rosenberg AL, Swartz RD (2007) Predictors of postoperative acute renal failure after noncardiac surgery in patients with previously normal renal function. Anesthesiology 107(6):892-902.
30. Kheterpal S, Tremper KK, Heung M, Rosenberg AL, Englesbe M, Shanks AM, Campbell DA, Jr. (2009) Development and validation of an acute kidney injury risk index for patients undergoing general surgery: results from a national data set. Anesthesiology 110(3):505-515.
31. Cho A, Lee JE, Kwon GY, Huh W, Lee HM, Kim YG, Kim DJ, Oh HY, Choi HY (2011) Post-operative acute kidney injury in patients with renal cell carcinoma is a potent
25
risk factor for new-onset chronic kidney disease after radical nephrectomy. Nephrol Dial Transplant 26(11):3496-3501.
32. Cha EK, Lee DJ, Del Pizzo JJ (2011) Current status of robotic partial nephrectomy (RPN). BJU Int 108(6 Pt 2):935-941.
33. Masuda T, Sato K, Noda C, Ikeda KM, Matsunaga A, Ogura MN, Shimizu K, Nagasawa H, Matsuyama N, Izumi T (2003) Protective effect of urinary trypsin inhibitor on myocardial mitochondria during hemorrhagic shock and reperfusion. Crit Care Med 31(7):1987-1992.
34. Oh SY, Kim JC, Choi YS, Lee WK, Lee YK, Kwak YL (2012) Effects of ulinastatin treatment on myocardial and renal injury in patients undergoing aortic valve replacement with cardiopulmonary bypass. Korean J Anesthesiol 62(2):148-153. 35. Zhang Z, Zhao J, Dong W, Remer E, Li J, Demirjian S, Zabell J, Campbell SC (2016) Acute Kidney Injury after Partial Nephrectomy: Role of Parenchymal Mass Reduction and Ischemia and Impact on Subsequent Functional Recovery. Eur Urol 69(4):745-752.
26
ABSTRACT (IN KOREAN)
로봇-복강경하 부분신절제술을 받는 환자들에서 ulinastatin의 수술 후 신기능에 미치는 영향 <지도교수 이숙영> 아주대학교 대학원 의학과 이 보 라 로봇-복강경하 부분신절제술은 신장 종양을 치료하는데 최근에 널리 쓰이는 방법이다. 하지만, 이런 로봇-복강경하 부분신절제술은 여러 장점에도 불구하고, 신동맥의 흐름을 일시적으로 멈추어(clamping) 신절제술을 시행하기 때문에 허혈성 신손상을 유발시킨다. 부분신절제술 후에 급성 신손상에 대한 빈도는 최대 39%까지 보고되고 있다. 그러나 이를 예방하는 효과적인 약물학적 방법은 아직 밝혀지지 않고 있다. 우리나스타틴은 항염증작용과 항산화작용이 있어 허혈/재관류 손상에서 신장을 보호해주는 것으로 알려져 있다. 따라서, 이 연구에서는 로봇-복강경하 부분신절제술을 받는 환자에서 우리나스타틴이 수술 후 신기능에 미치는 영향을 알아보고자 한다. 이 연구는 무작위 이중맹검 위약 조절 연구로서, 로봇-복강경하
27 부분신절제술을 받는 환자들 중에서 우리나스타틴군 (35명)에 배정된 환자들에게는 신동맥을 고정하기 (clamping) 10분 전부터 1 시간 동안 정맥으로 우리나스타틴 (100,000 units/10kg)을 투여하였고, 대조군 (35명)에서는 같은 시간 동안 같은 양의 생리식염수를 투여하였다. 수술 후에 급성신손상의 빈도를 조사하였고, 수술 전, 수술 후 1시간, 24시간, 48시간, 72 시간 후의 혈중 크레아티닌, 사구체여과율, cystatin C, 염증 표시자들을 조사하였다. 급성신손상의 빈도는 우리나스타틴군에서는 18%, 대조군에서는 30%였다. 두 군간 수술 후 혈중 크레아티닌, 사구체여과율, cystatin C는 통계적으로 유의한 차이가 없었다. Cystatin C, 백혈구 수치, 중성구의 비율을 포함한 염증 수치는 수술 전보다 수술 후 72시간까지 통계적으로 유의하게 증가되었지만, 두 군간 차이는 없었다. 결론적으로 로봇-복강경하 부분신절제술을 받는 환자들에서 허헐/재관류 기간 동안 우리나스타틴 (100,000 units/10 kg)을 투여하는 것은 수술 후 신기능에 통계적으로 유의한 효과를 보이지는 못했다. 핵심어: 급성신손상; 로봇 수술; 신절제술; 우리나스타틴; 재관류 손상