접수일
: 2018
년8
월23
일,
게재승인일: 2018
년9
월19
일 책임저자:
최유리,
광주시 광산구 첨단월봉로99
62284,
광주보훈병원 재활의학과Tel: 062-602-6253, Fax: 062-602-6230 E-mail: [email protected]
편측성 슬관절 골관절염이 있는 노인환자에서 동적균형운동의 효과
광주보훈병원 재활의학과
이봉연ㆍ신우용ㆍ안민지ㆍ윤서라ㆍ최유리
Effect of Dynamic Balance Exercise in Elderly Patients with Unilateral Knee Osteoarthritis
Bong-Yeon Lee, M.D., Woo-Yong Shin, M.D., Min-Ji An, M.D., Seo-Ra Yoon, M.D. and Yuri Choe, M.D.
Department of Physical Medicine and Rehabilitation, Gwangju Veterans Hospital, Gwangju, Korea
Objective: To evaluate the effectiveness of dynamic balance exercise after intra-articular injection of hyaluronic acid (HA) therapy in elderly patients with unilateral knee osteoarthritis. Method: 30 patients with unilateral knee osteoarthritis were enrolled in this study. The patients were randomly divided into two groups: dynamic balance exercise after HA injection group (group A) and only HA injection group (group B). Both groups administered intra-articular HA injection and group A patients continued 20-session exercises for 4 weeks. The assessments were measured before injection and 4 weeks after treatment using the visual analog scale (VAS) for pain, the Western Ontario and McMaster University Osteoarthritis Index (WOMAC) for physical function, Berg balance scale (BBS), and computerized dynamic posturography using SMART Balance Master system for balance function. Results: In both groups, significant improvements in VAS, WOMAC and balance function were observed. Compared between groups, group A showed significant improvements compared to group B in WOMAC and balance function. Conclusion:
It is suggested that dynamic balance exercise may result in improved balance function and physical function in elderly patients with unilateral knee osteoarthritis. (Clinical Pain 2019;18:16-23)
Key Words:
Osteoarthritis, Knee; Exercise; Hyaluronic acid; RehabilitationINTRODUCTION
Osteoarthritis (OA) is a chronic and degenerative disease characterized by high prevalence with increasing age.
Prevalences of radiographic knee OA and symptomatic knee OA are 37.3% and 24.2% in elderly community resi- dents in Korea.
1Knee OA is a common cause of knee pain, disability of the knee joint movement and degrading quality of life. Patients with knee OA experience a gradual loss of function with increased dependence on walking, stair climbing and other extremity tasks.
2Conservative treatments for knee OA consist of lifestyle modification, exercise, weight reduction, knee brace for varus or valgus instability, oral medications including acet- aminophen, non-steroidal anti-inflammatory drugs and opioids, thermal modalities, transcutaneous electrical nerve
stimulation and intra-articular hyaluronic acid (HA) and corticosteroid injections.
3Patients with knee OA show decreased strength of quad- riceps muscles
4-6and lack of knee joint proprioception.
7,8These impairments, coupled with the ageing process, may be more harmful to the balance function and increase risk of falls in OA patients compared with age-matched healthy population.
9,10Kinesthesia, balance and agility exercise have the pur- pose of improving joint stability, muscular recruitment and neuromuscular control. These exercises challenge the so- matosensory, visual and vestibular systems.
11Furthermore, considering poor dynamic balance function and neuro- muscular control in patients with knee OA, recent studies emphasized the importance of eccentric strength in balance function
12,13and targeted balance training for patients with knee OA was recommended.
Many clinicians recommend exercise for patients with
knee OA and the effect of exercise is obvious to physical
function.
14Some researchers showed that balance training
not only improves function capacity or postural control but
also reduces perceived knee pain.
15,16However, it is not
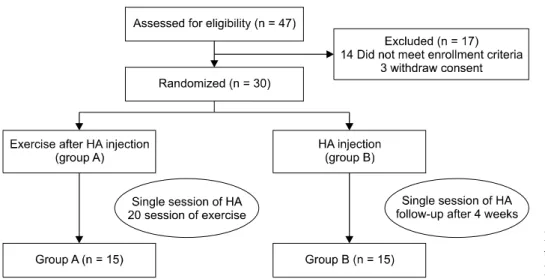
Fig. 1. Flow diagram, showing the
treatment process and assessment.HA: Hyaluronic acid.
clear whether the improvement of physical function is due to effect of balance training itself or decreasing pain.
Accordingly, we aimed to investigate the effect of balance training on patients with knee OA who treated by in- tra-articular HA injection.
Intra-articular HA injection becomes accepted as an ef- fective and safe treatment for elderly patients with knee OA, but according to our knowledge, there is only two studies that evaluate effect of intra-articular HA injection on balance function in knee OA patients.
17,18There is no study about whether dynamic balance exercise after in- tra-articular HA injection will result in enhanced outcomes over intra-articular HA injection alone in patients with knee OA. Therefore, the aim of this study was to investigate ef- fectiveness of dynamic balance exercise after intra-articular HA injection in elderly patients with unilateral knee OA.
MATERIALS AND METHODS 1. Study design
Study was a prospective, single-blind, randomized con- trolled trial. Participants were randomly distributed into 2 groups, dynamic balance exercise after intra-articular HA injection group (Group A) or only intra-articular HA in- jection group (Group B). Randomization was performed by using computerized random number generator. This re- search was approved by the Institutional Review Board of author’s hospital (2017-12-1).
2. Subjects
We recruited patients with unilateral knee pain who vis- ited author’s hospital from September 2017 to February 2018. Inclusion criteria were (1) age> 65; (2) patients di- agnosed with knee OA according to the clinical and radio- graphic criteria of the American College of Rheumatology (ACR)
19; (3) radiographic grade II or III OA confirmed ac- cording to the Kellgren-Lawrence grading scale; (4) in- volvement of unilateral knee joint through bilateral radiog- raphy and clinical exam. Exclusion criteria were (1) patients with comorbidities of neurologic diseases, cardiac disorder or hemodynamically unstable systems; (2) patients who had history of traumatic injury, surgeries, cancer or malignant tumors of lower extremities; (3) patients who received in- tra-articular injection treatment within the past 6months; (4) inability to ambulate without a gait aid. Of the 47 patients we recruited, 17 patients were excluded because they re- fused to participate or did not meet enrollment criteria and 30 participants were randomly assigned to the 2 groups (Fig. 1). All participants were informed about the study and consent form was obtained from each participants. No pa- tients were dropped out during treatment and follow-up.
3. Intra-articular HA injection
All participants received single US-guided intra-articular
HA injection (Synovian, LG life sciences, South Korea,
BDDE cross-linked sodium hyaluronate, 60 mg/3 mL, >
10000 kDa) into affected knee joint. Patients were placed
in a supine position on the table and knee joint was fixed
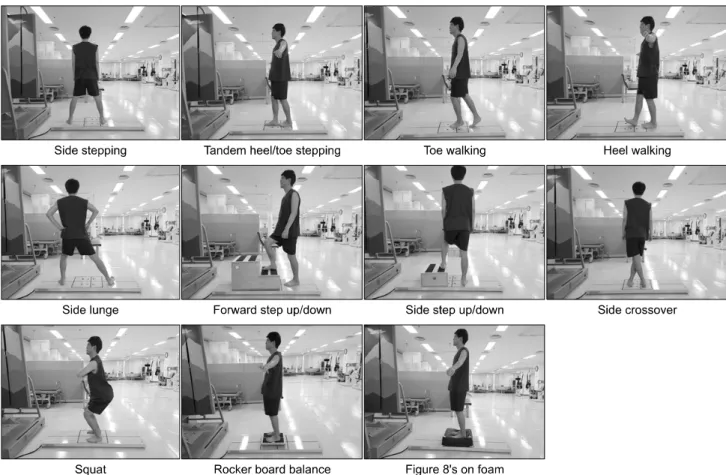
Fig. 2. Dynamic balance exercises.
in slightly flexed position. The ultrasound prove was trans- versely placed on the level of the suprapatellar bursa. After aseptic preparation, needle was inserted directly into supra- patellar bursa using in-plane lateral approach. Before in- jecting the hyaluronic acid, aspiration of joint fluid was conducted.
4. Balance exercise
Balance exercise program on the SMART Balance Master system (NeuroCom Inc., Clackamas, OR, USA) was conducted 1 week after injection in Group A. The SMART Balance Master system consists of dual force plates, long force plate, a display monitor, a visual surround environ- ment and a safety harness and is used for balance test and balance exercise. Participants stood on long force plate and exercised following instructions at screen in front of them.
Dynamic exercise program (Fig. 2, Table 1) consisted of ex- ercises enhancing balance control, eccentric muscle strength and core stability.
20Exercise program was applied as each
time or numbers with physical therapist. Participants per- formed all exercise 5 times a week for 4 weeks.
5. Outcome measures
1) Balance function test: Balance function data was obtained using SMART Balance Master system and Berg balance scale (BBS). Patients stood on the dual force plates and gazed cursor as their center of gravity (COG) on the display monitor. Assessment items were composed of sensory organization test (SOT) for sensory limitation assessment and rhythmic weight shift test (RWST) for motor limitation assessment. The SMART Balance Master system showed moderate to good reliability and validity for assessing balance function.
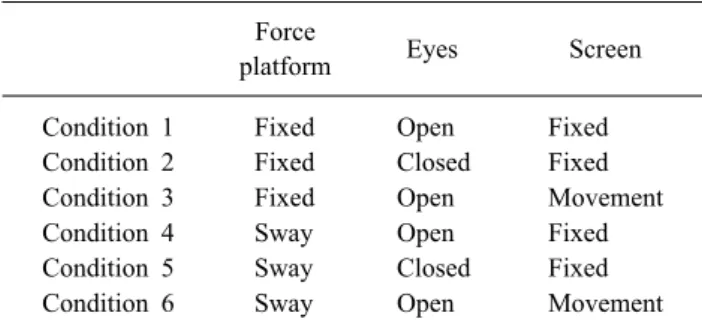
21-23SOT was administered for assessing ability to maintain
static standing balance. Participants were asked for stand-
ing on dual force plates and keep their cursor of COG on
center of monitor under following six conditions for 20
seconds (Table 2). Participants carried out each trial three
Table 1. Dynamic Balance Exercises Description
Exercise Description Time/reps
Side stepping Subjects step to side with left leg and move Right leg to left. Subjects repeat in opposite direction.
1∼2 min Tandem heel/toe
stepping
Subjects walk with the toes of the back foot touching the heel of the front foot at
each step. 1∼2 min
Toe walking Subjects stand on toes and walk forward on toes. 1∼2 min
Heel walking Subjects stand on heels and walk forward on heels. 1∼2 min
Side lunge Subjects stretch one leg laterally and widely while the other leg bends slightly. 12∼15 reps/3sets Forward step
up/down
Subjects go up one stair in front of them and go down anteriorly. Stair height varies
based on their ability. 1∼2 min
Side step up/down Subjects go up one stair sideways, stand with both legs and go down sideways. Stair
height varies based on their ability. 1∼2 min
Side crossover
stepping Subjects step with left leg crossing in front of right leg and move right leg far to the right. 1∼2 min Squat Subjects bends their knees at the prescribed angle of knee based on their ability. 12∼15 reps/3sets Rocker board
balance training Subjects stand on a rocker board with both legs and keep a balance for 30∼60 seconds. 1∼2 min Figure 8’s on foam Subjects stand on soft foam and move center of gravity in figure 8 form. 1∼2 min Reps: repetitions, min: minute.
Table 2. Six Conditions of Sensory Organization Test
Forceplatform Eyes Screen
Condition 1 Fixed Open Fixed
Condition 2 Fixed Closed Fixed
Condition 3 Fixed Open Movement
Condition 4 Sway Open Fixed
Condition 5 Sway Closed Fixed
Condition 6 Sway Open Movement
times and average SOT score was recorded from 0 to 100, with high score representing high stability.
RWST was administered for assessing ability to move center of gravity forward and backward or left to right.
While standing on dual force plates, participants leaned for moving their cursor of COG in line with a moving target on screen at 3 distinct speeds (slow, medium, and fast). Test was performed three times each (1) front and back and (2) left and right. Measurements were recorded in (1) on-axis velocity (º/s), indicating the velocity of movement toward a target; and (2) directional control (DCL) (%), indicating percentage of how accurately move along the axis. On-axis velocity reflects the agility of subject’s COG movement and DCL reflects accuracy of subject’s COG movement.
BBS consists of 14 items to measure static and dynamic balance abilities in the elderly. It is a 56-point scale and higher scores represent better balance. BBS scale has ex- cellent inter-rater and intra-rater relative reliability.
242) Secondary measurement: Physical function was assessed by WOMAC, validated and reliable self- reporting questionnaire for knee OA.
26WOMAC consist of five questions for pain, two for stiffness and seventeen for physical function. WOMAC score range from o to 96, with high score representing worse symptom severity. To
evaluate the physical function, we used a WOMAC- physical function subscale.
Pain was assessed using a WOMAC-pain subscale and a visual analog scale (VAS). Participants were asked to ex- press the average pain of affected knee with 0 indicating no pain and 10 indicating maximal pain for evaluating VAS.
25SOT, on-axis velocity, directional control, BBS, VAS score and WOMAC score were measured at baseline and follow-up (group A: after 4-week exercise program, group B: 4 weeks after injection) by the same assessors for both groups.
6. Statistical analysis
A student t-test and a chi-squared test were used to com-
pare the baseline variables between two groups. Wilcoxon
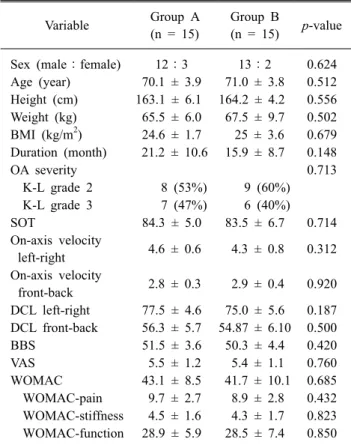
Table 3. Demographic and Baseline Clinical Characteristics of
SubjectsVariable Group A (n = 15)
Group B
(n = 15)
p-value
Sex (male:female) 12:3 13:2 0.624
Age (year) 70.1 ± 3.9 71.0 ± 3.8 0.512 Height (cm) 163.1 ± 6.1 164.2 ± 4.2 0.556 Weight (kg) 65.5 ± 6.0 67.5 ± 9.7 0.502 BMI (kg/m2) 24.6 ± 1.7 25 ± 3.6 0.679 Duration (month) 21.2 ± 10.6 15.9 ± 8.7 0.148
OA severity 0.713
K-L grade 2 8 (53%) 9 (60%)
K-L grade 3 7 (47%) 6 (40%)
SOT 84.3 ± 5.0 83.5 ± 6.7 0.714
On-axis velocity
left-right 4.6 ± 0.6 4.3 ± 0.8 0.312 On-axis velocity
front-back 2.8 ± 0.3 2.9 ± 0.4 0.920 DCL left-right 77.5 ± 4.6 75.0 ± 5.6 0.187 DCL front-back 56.3 ± 5.7 54.87 ± 6.10 0.500
BBS 51.5 ± 3.6 50.3 ± 4.4 0.420
VAS 5.5 ± 1.2 5.4 ± 1.1 0.760
WOMAC 43.1 ± 8.5 41.7 ± 10.1 0.685
WOMAC-pain 9.7 ± 2.7 8.9 ± 2.8 0.432 WOMAC-stiffness 4.5 ± 1.6 4.3 ± 1.7 0.823 WOMAC-function 28.9 ± 5.9 28.5 ± 7.4 0.850 Values are presented as numbers or mean ± standard deviation, n (%), or as otherwise indicated.
BMI: body mass index, OA: osteoarthritis, K-L grade: Kellgren- Lawrence grade, SOT: sensory organization test, DCL: direc- tional control, BBS: Berg balance scale, VAS: visual analogue scale, WOMAC: Western Ontario and McMaster University Osteoarthritis Index.
signed-rank test was used to compare the changes between pre- and post-treatment in each group and Mann-Whitney U test was used to compare the changes between two groups. p values <0.05 were considered statistically signi- ficant. SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA) was used for all statistical analyses.
RESULTS
There were no significant differences between groups with regard to demographic and clinical characteristics at baseline (Table 3). Five patients complained of local pain at the lateral knee region after the injection, which dis- appeared after the next few days spontaneously.
1. Comparison of balance function
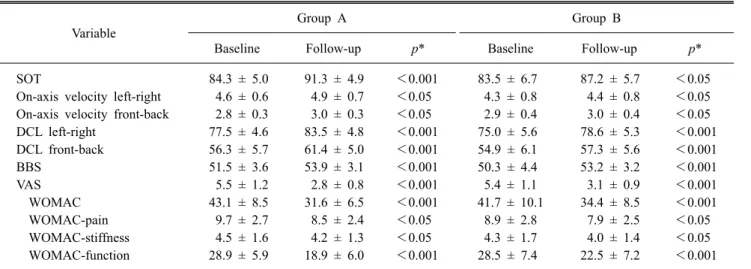
Table 4 shows a summary of outcome measurements.
Group A and B showed significant improvements in SOT (group A: from 84.3 ± 5.0 to 91.3 ± 4.9; p<0.001, group B: from 83.5 ± 6.7 to 87.2 ± 5.7; p<0.05), on-axis velocity left-right (group A: from 4.6 ± 0.6 to 4.9 ± 0.7; p<0.05, group B: from 4.3 ± 0.8 to 4.4 ± 0.8; p<0.05), on-axis velocity front-back (group A: from 2.8 ± 0.3 to 3.0 ± 0.3;
p<0.05, group B: from 2.9 ± 0.4 to 3.0 ± 0.4; p<0.05), DCL left-right (group A: from 77.5 ± 4.6 to 83.5 ± 4.8;
p<0.001, group B: from 75.0 ± 5.6 to 78.6 ± 5.3; p<
0.001), DCL front-back (group A: from 56.3 ± 5.7 to 61.4 ± 5.0; p<0.001, group B: from 54.9 ± 6.1 to 57.3 ± 5.6; p<
0.001) and BBS (group A: from 51.5 ± 3.6 to 53.9 ± 3.1;
p<0.001, group B: from 50.3 ± 4.4 to 53.2 ± 3.2; p<
0.001). Table 5 shows difference in each outcome measure- ments between two groups. Improvement in SOT, on-axis velocity left-right, DCL left-right and DCL front-back was significantly higher in group A than in group B (p<0.05), although improvement in on-axis velocity front-back and BBS was not different statistically between two groups (on-axis velocity front-back: p=0.459, BBS: p=0.420).
2. Comparison of pain intensity and physical function
Relative to their baseline values, both groups showed significant improvements in VAS scores (group A: from 5.5 ± 1.2 to 2.8 ± 0.8; p<0.001, group B: from 5.4 ± 1.1 to 3.1 ± 0.9; p<0.001), WOMAC scores for pain (group A: from 9.7 ± 2.7 to 8.5 ± 2.4; p<0.05, group B: from
8.9 ± 2.8 to 7.9 ± 2.5; p<0.05), stiffness (group A: from 4.5 ± 1.6 to 4.2 ± 1.3; p<0.05, group B: from 4.3 ± 1.7 to 4.0 ± 1.4; p<0.05) and physical function (group A:
from 28.9 ± 5.9 to 18.9 ± 6.0; p<0.001, group B: from
28.5 ± 7.4 to 22.5 ± 7.2; p<0.001) (Table 4). In compar-
ison between groups, improvements in WOMAC scores for
physical function were significantly higher in group A than
in group B (p<0.05), although improvements in VAS,
WOMAC scores for pain and stiffness were not different
statistically (VAS; p=0.127, WOMAC-pain; p=0.713,
WOMAC-stiffness; p=0.775) (Table 5).
Table 4. Changes at Baseline and Follow-up within Each Group
Variable Group A Group B
Baseline Follow-up
p*
Baseline Follow-upp*
SOT 84.3 ± 5.0 91.3 ± 4.9 <0.001 83.5 ± 6.7 87.2 ± 5.7 <0.05
On-axis velocity left-right 4.6 ± 0.6 4.9 ± 0.7 <0.05 4.3 ± 0.8 4.4 ± 0.8 <0.05 On-axis velocity front-back 2.8 ± 0.3 3.0 ± 0.3 <0.05 2.9 ± 0.4 3.0 ± 0.4 <0.05
DCL left-right 77.5 ± 4.6 83.5 ± 4.8 <0.001 75.0 ± 5.6 78.6 ± 5.3 <0.001
DCL front-back 56.3 ± 5.7 61.4 ± 5.0 <0.001 54.9 ± 6.1 57.3 ± 5.6 <0.001
BBS 51.5 ± 3.6 53.9 ± 3.1 <0.001 50.3 ± 4.4 53.2 ± 3.2 <0.001
VAS 5.5 ± 1.2 2.8 ± 0.8 <0.001 5.4 ± 1.1 3.1 ± 0.9 <0.001
WOMAC 43.1 ± 8.5 31.6 ± 6.5 <0.001 41.7 ± 10.1 34.4 ± 8.5 <0.001
WOMAC-pain 9.7 ± 2.7 8.5 ± 2.4 <0.05 8.9 ± 2.8 7.9 ± 2.5 <0.05
WOMAC-stiffness 4.5 ± 1.6 4.2 ± 1.3 <0.05 4.3 ± 1.7 4.0 ± 1.4 <0.05
WOMAC-function 28.9 ± 5.9 18.9 ± 6.0 <0.001 28.5 ± 7.4 22.5 ± 7.2 <0.001
Values are presented as mean ± standard deviation or as otherwise indicated.
SOT: sensory organization test, DCL: directional control, BBS: Berg balance scale, VAS: visual analogue scale, WOMAC: Western Ontario and McMaster University Osteoarthritis Index.
*Wilcoxon signed-rank test.
Table 5. Difference in Each Outcome Measures between Two
GroupsVariables Group A Group B
p*
△SOT 7.0 ± 3.2 3.7 ± 1.8 <0.05
△On-axis velocity
left-right 0.3 ± 0.1 0.1 ± 0.1 <0.05
△On-axis velocity
front-back 0.2 ± 0.1 0.1 ± 0.1 0.459
△DCL left-right 6.0 ± 1.3 3.6 ± 1.8 <0.05
△DCL front-back 5.1 ± 1.3 2.4 ± 1.4 <0.05
△BBS 2.3 ± 1.5 2.9 ± 1.8 0.420
△VAS −2.7 ± 0.5 −2.3 ± 0.3 0.127
△WOMAC −11.5 ± 4.6 −7.3 ± 4.4 <0.05
△WOMAC-pain −1.3 ± 1.0 −1.1 ± 1.0 0.713
△WOMAC-stiffness −0.3 ± 0.5 −0.3 ± 0.5 0.775
△WOMAC-function −10.0 ± 4.5 −5.9 ± 4.1 <0.05 Values are presented as mean ± standard deviation or as other- wise indicated.
SOT: sensory organization test, DCL: directional control, BBS:
Berg balance scale, VAS: visual analogue scale, WOMAC:
Western Ontario and McMaster University Osteoarthritis Index.
*Mann-Whitney U test.
DISCUSSION
According to our knowledge, this is the first randomized controlled trial to compare the effects of dynamic balance exercise after HA injection with that of only HA injection in the treatment of unilateral knee OA. Findings of this study showed that dynamic balance exercise after HA in- jection improved pain, balance function and physical func- tion, moreover dynamic balance exercise after HA injection had additive effects compared to only HA injection except pain.
Sun et al
.17reported that intra-articular HA injection for patients with knee OA significantly improve in pain, phys- ical function and balance function as single-leg stance test, functional reach test, up-and-go test and Berg balance scale. These results are similar to those of the control group in our study.
Previous studies reported that balance training is an ef- fective treatment for knee OA. Diracoglu et al.
27compared patients with kinesthesia and balance exercises in addition to strengthening exercises and patients with only strength- ening exercises, and additive kinesthesia and balance ex- ercises showed significantly greater improvements in meas- ures of function (WOMAC, SF-36 Form, 10 stairs climbing and 10m walking times) than only strengthening exercises.
Sekir et al.
28reported that 4-week proprioceptive exercise
program resulted in a significant improvement in pain, pos- tural control and functional capacity in patients with bi- lateral knee OA. Similar to previous studies, this study showed that balance function and physical function were significantly improved after dynamic balance training in patients with knee OA. Balance function, pain score, and functional status were significantly improved in both group A and group B. In measurement of balance function, most assessments using Balance Master system and WOMAC scores for physical function showed significant improve- ments in group A than in group B. VAS score and WOMAC scores for pain and stiffness were not sig- nificantly improved in group A than in group B. Therefore, Dynamic balance training improved the physical function in elderly patients with knee OA. However, Improvement of front-back control on axis velocity of two groups was similar. We should have assessed the strength or range of motion of ankle of the patients. It was one of limitation of this study. In addition, BBS score was not significantly improved. It may be affected by the ceiling effect of BBS scale
29because all patients scored over 40 points consid- ered a good balance at baseline and 14 patients scored a full mark at follow-up.
Rehabilitation of patients with arthritis emphasizes train- ing to restore or maintain joint motility and strength, and to enhance functional independence. Because knee OA has a nature of chronic disease, it is important that exercise for patients with knee OA does not put burden on knee joint by approaching from the viewpoint of management rather than treatment. Therefore, we focused on high adherence of dynamic balance exercise and evaluated whether dynam- ic balance exercise after intra-articular HA injection have additional effect for improved symptom, functional ability and dynamic balance.
There were several limitations in this study. First, HA injection group did not conducted any exercise inter- vention. Because the contact time of researcher can affect outcomes, different contact time with researchers may in- fluence final findings. Second, the number of participants was relatively small. Third, intervention period and fol- low-up period were short. Therefore long-term effects of intervention are unknown. Thus, future researches includ- ing control group conducting active intervention in regard to general exercise program, larger sample size and longer follow-up period should be performed.
In conclusion, dynamic balance exercise after HA in- tra-articular injection in unilateral knee OA patients was more effective in balance and physical function compared to the injection without exercise.
REFERENCES
1. Kim I, Kim HA, Seo YI, Song YW, Jeong JY, Kim DH.
The prevalence of knee osteoarthritis in elderly community residents in Korea. J Korean Med Sci 2010; 25: 293–298 2. Peat G, McCamey R, Croft P. Knee pain and osteoarthritis
in older adults: a review of community burden and current use of primary healthcare. Ann Rheum Dis 2001; 60: 91–
97
3. Zhang W, Moskowitz RW, Nuki G, Abramson S, Altman RD, Arden N, et al. OARSI recommendations for the man- agement of hip and knee osteoarthritis, Part II: OARSI evi- dence-based, expert consensus guidelines. Osteoarthritis Cartilage 2008; 16: 137–162
4. Wessel J. Isometric strength measurements of knee ex- tensors in women with osteoarthritis of the knee. J Rheumatol 1996; 23: 328–331
5. Fisher NM, Pendergast DR. Reduced muscle function in patients with osteoarthritis. Scand J Rehabil Med 1997; 29:
213–221
6. O'Reilly SC, Jones A, Muir KR, Doherty M. Quadriceps weakness in knee osteoarthritis: The effect on pain and disability. Ann Rheum Dis 1998; 57: 588–594
7. Pai Y‐C, Rymer WZ, Chang RW, Sharma L. Effect of age and osteoarthritis on knee proprioception. Arthritis Rheum 1997; 40: 2260–2265
8. Sharma L, Pai Y‐C, Holtkamp K, Rymer WZ. Is knee joint proprioception worse in the arthritic knee versus the un- affected knee in unilateral knee osteoarthritis? Arthritis Rheum 1997; 40: 1518–1525
9. Lim KB, Lee HJ. Computerized posturographic measure- ment in elderly women with unilateral knee osteoarthritis.
Ann Rehabil Med 2012; 36: 618-626
10. Kim HS, Yun DH, Yoo SD, Kim DH, Jeong YS, Yun JS, et al. Balance control and knee osteoarthritis severity. Ann Rehabil Med 2011; 35: 701-709
11. Taylor JB. Lower extremity perturbation training. Strength Cond J 2011; 33: 76-83
12. Takacs J, Carpenter MG, Garland SJ, Hunt MA. Factors as- sociated with dynamic balance in people with knee osteoarthritis. Arch Phys Med Rehabil 2015; 96:
1873-1879
13. Sanchez-Ramirez DC, van der Leeden M, Knol DL, van der Esch M, Roorda LD, Verschueren S, et al. Association
of postural control with muscle strength, proprioception, self-reported knee instability and activity limitations in pa- tients with knee osteoarthritis. J Rehabil Med 2013; 45:
192-197
14. Fransen M, McConnell S, Harmer AR, Van der Esch M, Simic M, Bennell KL. Exercise for osteoarthritis of the knee: a Cochrane systematic review. Br J Sports Med 2015;
49: 1554-1557
15. Clark S, Rose D, Fujimoto K. Generalizability of the limits of stability test in the evaluation of dynamic balance among older adults. Arch Phys Med Rehabil 1997; 78:
1078–1084
16. Difabio R, Badke M. Relationship of sensory organization to balance function in patients with hemiplegia. Phys Ther 1990; 70: 542–548
17. Sun SF, Hsu CW, Hwang CW, Hsu PT, Wang JL, Tsai SL, et al. Hyaluronate improves pain, physical function and balance in the geriatric osteoarthritic knee: a 6-month fol- low-up study using clinical tests. Osteoarthritis Cartilage 2006; 14: 696-701
18. Khalaj N, Abu Osman NA, Mokhtar AH, George J, Abas WA. Effect of Intra-Articular Hyaluronic injection on pos- tural stability and risk of fall in patients with bilateral knee osteoarthritis. Scientific World Journal 2014; 2014: 815184 19. Altman R, Asch E, Bloch D, Bole G, Borenstein D, Brandt
K, et al. Development of criteria for the classification and reporting of osteoarthritis. Classification of osteoarthritis of the knee. Diagnostic and Therapeutic Criteria Committee of the American Rheumatism Association. Arthritis Rheum 1986; 29: 1039-1049
20. Takacs J, Krowchuk NM, Garland SJ, Carpenter MG, Hunt MA. Dynamic balance training improves physical function in individuals with knee osteoarthritis: a Pilot randomized controlled trial. Arch Phys Med Rehabil 2017; 98:
1586-1593
21. Black F, Paloski W, Reshke M, Calkins D, Shupert C.
Vestibular ataxia following shuttle flights: effects of micro- gravity on otolith-mediated sensorimotor control of pos- ture. Am J Otol. 1993; 14: 9–17
22. Hageman P, Leibowitz J, Blanke D. Age and gender effects on posture control measures. Arch Phys Med Rehabil.
1995; 76: 961-965
23. Liston R, Brouwer B. Reliability and validity of measures obtained from stroke patients using the Balance Master.
Arch Phys Med Rehabil. 1996; 77: 425–429
24. Downs S, Marquez J, Chiarelli P. The Berg Balance Scale has high intra- and inter-rater reliability but absolute reli- ability varies across the scale: a systematic review. J Physiother. 2013; 59: 93-99
25. Jensen MP, Chen C, Brugger AM. Interpretation of visual analog scale ratings and change scores: a reanalysis of two clinical trials of postoperative pain. J Pain 2003; 4: 407–
414
26. Bellamy N, Campbell J, Stevens J, Pilch L, Stewart C, Mahmood Z. Validation study of a computerized version of the Western Ontario and McMaster Universities VA3.0 Osteoarthritis Index. J Rheumatol 1997; 24: 2413–2415 27. Diracoglu D, Aydin R, Baskent A, Celik A. Effects of kin-
esthesia and balance exercises in knee osteoarthritis. J Clin Rheumatol. 2005; 11: 303-310
28. Sekir U, Gür H. A multi-station proprioceptive exercise program in patients with bilateral knee osteoarthrosis: func- tional capacity, pain and sensoriomotor function. A randomized controlled trial. J Sports Sci Med. 2005; 4:
590-603
29. Blum L, Korner-Bitensky N. Usefulness of the Berg Balance Scale in stroke rehabilitation: a systematic review.
Phys Ther 2008; 88: 559-566