생체간이식에서 담도 문합 방법: 국내 9개 간이식 병원 설문 조사 분석
Surgical Technique of Biliary Reconstruction in Adult-to-Adult Living Donor Liver Transplantation: Survey of 9 Major Centers in Korea
Purpose: Despite refinements in the surgical techniques for adult-to-adult living donor liver transplantation (ALDLT), biliary complications still remain the Achilles’ heel of ALDLT. Moreover, there is no consensus for the ideal technique of biliary reconstruction to reduce the rate of complications to an acceptable range. We strove to collate the available data of the current surgical techniques for biliary reconstruction in ALDLT in Korea.Methods: A questionnaire concerning the surgical techniques for biliary reconstruction was sent to 9 surgeons who performed biliary anastomosis in the major LDLT centers of Korea (the response rate was 100%).
Results: MR cholangiography (n=7) and/or intra-operative cholangiography (n=5) were routinely performed to evaluate the donor biliary anatomy. All the participants (n=9) preferred duct-to-duct anastomosis to hepatico-jejunostomy. Anastomosis was usually made on the whole layer (n=7 epithelium, n=2) of recipient’s common hepatic duct under loupe magnification (n=8); only one center reconstructed the anastomosis on the 2nd order hepatic duct under view of a surgical microscope. There were various techniques for biliary reconstruction as follows: suture material (absorbable: n=5, non-absorbable: n=4), suture method (continuous: n=4, interrupted: n=3, mixed:
n=3) and the use of a biliary stent (routine: n=3, sometimes: n=5, rare: n=1). Ductoplasty was performed on the back table (n=7) for the cases with a very close distance (<5 mm) between the bile ducts’ openings, but each duct was separately anastomosed to the recipients’ bile duct (n=8) or a roux-en-Y limb (n=1) was done in cases with a distance more than 10 mm.
Conclusion: In 9 LDLT centers of Koreas, duct-to-duct was preferred; however, there was no unique consensus, among the major centers, for the biliary reconstruction techniques that might reduce complications.
이남준1
, 권준혁
2, 김건국
3, 김봉완
4,
유영경5, 최진섭
6, 하태용
7, 한영석
8,
이광웅1,91서울대학교 의과대학 외과학교실,
2성균관대학교 의과대학 삼성의료원 외과학교실, 3가천의과학대학교 길병원 외과학교실, 4아주대학교 의과대학 아주대학교병원 외과학교실,
5가톨릭대학교 의과대학 외과학교실,
6연세대학교 의과대학 외과학교실,
7울산대학교 의과대학 서울아산병원 외과학교실, 8대구가톨릭대학교 의과대학 외과학교실, 9국립암센터 간암센터
Nam-Joon Yi, M.D.
1, Choon Hyuck David Kwon, M.D.
2, Keon Kuk Kim, M.D.
3, Bong-Wan Kim, M.D.
4, Young Kyoung You, M.D.
5, Jin Sub Choi, M.D.
6, Tae-Yong Ha, M.D.
7, Young Seok Han, M.D.
8, Kwang-Woong Lee, M.D.
1,9Deparment of Surgery, 1Seoul National University College of Medicine, 2Sam- sung Medical Center, Sungkyunkwan University School of Medicine, 3Gachon Medical School, Gil Medical Center,
4Deparment of Surgery, Ajou University Hospital, Ajou University School of Medicine, 5The Catholic University of Korea, College of Medicine, 6Yonsei University College of Medicine, 7Asan Medical Center, University of Ulsan College of Medicine, 8Catholic Univer- sity of Daegu, School of Medicine,
9Center for Liver Cancer, National Cancer Center
책임저자 이 광 웅
서울시 종로구 대학로 101 서울대학교 의과대학 외과학교실 우편번호 110-744
Tel: 02-2072-2511 Fax: 02-766-3975
E-mail: kwleegs@korea.com
*본 논문은 2010년 한국간담췌외과학회 춘계학술대회에서 패널심포지엄으로 발표하였음.
Key Words : Biliary, Complications, Living donor liver Transplantation, Survey, Korea 중심단어 : 담도합병증, 생체 간이식, 설문조사, 한국
Received: 2010. 9. 14.
Accepted: 2010. 10. 5.
서 론
간이식 수혜자의 장기 생존율이 향상되면서, 간이식 후 가 장 흔한 합병증인 담도 합병증은 간이식을 하는 외과의들과 수혜자의 삶의 질을 저해하는 가장 큰 골칫거리가 되었고, 간 이식의 아킬레스 건이라고도 불린다.1,2 최근 그 빈도가 줄었 다고는 하지만 생체 간이식에서 아직 30% 내외의 높은 유병 률을 보이고 있다.3-6 특히 우간을 주로 사용하는 성인간 생체 간이식에서는 전간을 이식하는 뇌사자 이식편에 비해서 담도 가 상대적으로 작고 짧으며 때로는 다발성이기 때문에 뇌사자 간이식에 비해 담도 합병증 발생율이 높다.6-8
담도 합병증의 위험 인자로는 이식편의 종류, 수혜자의 중 증도, 내경이 4 mm보다 작은 담도, 여러 개의 담도, 허혈 시 간 등이 알려져 있는데 이들 요인은 복합적으로 작용하며,4,6-10 술자의 노력으로 합병증 발생을 예방하기 어려운 요소이다.
기술적인 면에서 담도 합병증을 줄일 수 있는 방법이 여러 논 문에서 소개되고 있으나,11,12 여러 요인이 복합적으로 작용하 는 담도합병증의 특성상 아직까지도 담도 합병증 발생을 획기 적으로 줄일 수 있는 방법은 제시되지 못했다.
우리 나라는 단위 병원당, 단위 인구당 세계에서 가장 많은 생체 간이식을 시행하고 있으며, 이식 성적도 세계적으로 가 장 좋은 성적을 보이고 있다.13-18 이에 저자들은 우리나라에서 생체 간이식을 시행하는 주요 병원들의 담도 문합 기법에 관 한 설문을 실시하고 이를 공유하여, 담도 문합 술기의 발전에 도움이 되고자 본 연구를 시행하였다.
방 법
2008년 국립장기이식병원(KONOS) 연보상 연간 20개 이상 의 간이식을 시행한 국내 9개 병원(국립암센터, 길병원, 대구 가톨릭병원, 삼성서울병원, 서울대학교병원, 서울성모병원, 세브란스병원, 서울아산병원, 아주대병원, 이상 가나다 순)을 국내 주요 간이식 센터로 선정하였다. 이들 9개 병원에서 간 이식 중 담도 문합을 주로 담당하고 있는 9명의 외과의에게 설문을 시행하였다. 설문 응답률은 100%였으며 각 문항별 응 답률 역시 100%였다. 설문은 총 19문항으로 생체 간이식 중 담도 수술에 관해 다음과 같은 3가지 내용으로 분류하였다 (Table 1): 1) 담도 문합법 선호도(담도대 담도 문합법: 담도공
장 문합법, 2문항), 2) 공여자 담도 검사 및 수술 방법(4문항), 3) 수혜자 담도대 담도 문합에 관한 구체적인 술기(13문항).
결 과
1. 담도 문합법 선호도: 담도대 담도 문합과 담도공장 문합법(Table 2)
9개 병원 모두에서 생체 간이식에서 담도대 담도문합법을 선호하여 담도 문합술 시 우선적으로 고려하였다. 8개 병원에 서는 담도공장 문합이 전체 담도 문합의 10% 미만이라 답하 였고, 1개 병원에서만 10∼50%라고 답하였다.
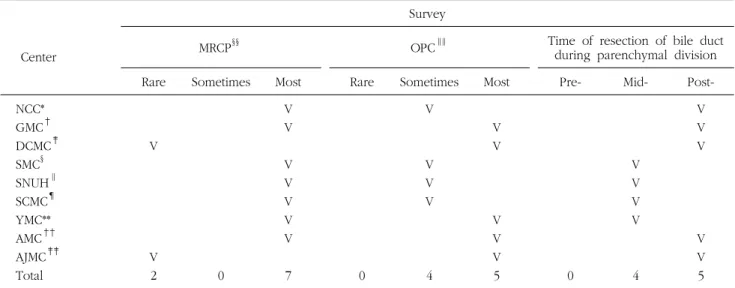
2. 공여자 수술 중 담도 검사 및 수술 방법(Table 3) 수술 전 자기공명검사(MR cholangiography, MRCP)는 7개 병원에서는 거의 모든 예에서 시행하였고, 2개 병원은 거의 시행하지 않았다. 수술 중 담도조영술(operative cholangio- graphy, OPC)은 5개 병원에서는 거의 모든 예에서 시행하였 고, 나머지 4개 병원에서는 필요한 경우에만 시행하였다. 9개 병원 모두에서 간절리 전 담도를 미리 박리하지 않고 간절리 가 중간 이상 진행되었을 때 담도를 절리하였으며, 이 중 5개 병원에서는 간절리를 완전히 마친 후 담도를 절리하였다. 공 여자 담도 절리시 담도 혈류를 보존하기 위해서 전기 소작기 를 사용하지 않거나 Glissonian sheath를 보존한다고 하였다.
3. 수혜자 담도대 담도문합
담도대 담도 문합의 구체적인 방법에 관한 설문은 수혜자 담도 준비, 담도 문합의 실제, 2개 이상의 담도 문합으로 구분 하였다.
1) 수혜자 담도 준비(Table 4)
수혜자의 전간절제술 시 일반적으로 절리하는 담도의 위치 는 9개 병원 모두에서 담도의 1차 분지(좌우 간관) 이상으로, 이 중 4개 병원에서는 대개 2차 분지 이상의 담도를 절리한다 고 답하였다. 그러나 실제로 공여자의 담도를 연결하는 수혜 자 담도의 위치는 8개 병원에서는 수혜자의 총간관(common hepatic duct)에 시행하였고, 이 중 2개 병원에서는 자주 좌우 간관을 이용한다고 하였다. 대부분의 경우 2차 분지 이상의 담도를 이용하는 병원도 1개 있었다. 담도 문합시 대개 미세 현미경 수술을 시행하지 않았으나, 2차 분지 이상의 담도를 이용하는 1개 병원에서는 미세현미경 수술을 시행한다고 답
Table 1. Survey of biliary reconstruction in adult-to-adult living donor liver transplantation
Duct-to-duct biliary reconstruction vs. Hepatico-jejunostomy 1. What is your preferred method for biliary reconstruction
during ALDLT?
A. Duct-to-duct anastomosis (DD) B. Hepatico-jejunostomy (HJ)
2. What is percentage of HJ in your biliary reconstruction in ALDLT?
A. <10%
B. 10∼50%
C. 50∼90%
D. ≥90%
Evaluation and resection of donor bile duct during donor operation
1. Do you performo pre-operative MRCP (MR cholangiogra- phy) routinely?
A. Never B. Sometimes C. Almost all cases
D. Other opinion ( )
2. When do you divide donor bile duct during donor opera- tion?
A. Before parenchymal division, i.e., during hilar dissec- tion
B. On midterm of parenchymal division C. After completion of parenchymal division D. Other opinion ( )
3. Do you perform operative cholangiography in order to get precise diving point?
A. Never B. Sometimes C. Almost all cases
D. Other opinion ( )
- Describe your technical tips for preserving biliary microcirculation during donor hepatectomy.
Technique of DD biliary reconstruction
1. Which level of the recipient bile duct do you get during recipient hepatectomy?
A. Common hepatic duct
B. 1st order branch; Right and left hepatic duct C. 2nd order branch; Right anterior and posterior hepatic
duct
D. More proximal intrahepatic bile duct than the 2nd order branch
2. Which level of the recipient bile duct do you prefer for anastomosis?
A. Common hepatic duct
B. 1st order branch; Right and left hepatic duct
Table 1. Continued 1
C. 2nd order branch; Right anterior and posterior hepatic duct
D. Other opinion ( )
3. Do you perform microsurgical technique for biliary recon- struction?
A. Never B. Sometimes C. Almost all cases
D. Other opinion ( )
4. Which string is your choice for DD biliary anastomosis?
A. 6-0 Prolene or compatible B. 6-0 PDS or compatible C. 6-0 Vicryl or compatible D. 7-0 Prolene or compatible E. 7-0 PDS or compatible F. 7-0 Vicryl or compatible G. Others ( )
5. Which technique do you perform for DD biliary anasto- mosis?
A. Interrupt sutures for both anterior and posterior walls B. Continuous sutures for both anterior and posterior walls C. Mixed technique, e.g. continuous sutures for posterior
wall but interrupted sutures for anterior wall) D. Other opinion ( )
6. Which layer do you bite for DD biliary anastomosis?
A. Whole layer B. Inner epithelial layer
C. Inner epithelial and subserosal layer
D. Other opinion ( ) 7. Do you put a biliary stent during biliary reconstruction?
A. Sometimes (Move to questionnaire 8) B. Almost all cases (Move to questionnaire 9) C. Never (Move to questionnaire 10)
8. When do you put a biliary stent during biliary recon- struction?
A. When the diameter of donor or recipient bile duct is very small
B. When the tension of anastomosis impairs the security C. When redundant biliary anastomosis disturbs bile flow D. Other opinion ( ) 9. Which type of a biliary stent do you prefer?
A. Short internal stent B. Long internal stent C. I-type external stent D. T-tube
E. Others ( )
9-1. Describe the material of a biliary stent you use?
Table 2. Preference of biliary reconstructionin adult-to-adult living donor liver transplantation
Center
Survey
Preference Incidence of hepaticojejunostomy Duct-to-
dcut
Hepati- cojejunos-
tomy
<10% 10∼50% 50∼90%
NCC*
GMC† DCMC‡ SMC§ SNUH∥ SCMC¶ YMC**
AMC††
AJMC‡‡
Total
V V V V V V V V V
9 0
V V V V V V V V 8
V
1 0
*National cancer center; †Gil medical center; ‡Catholic medical center of daegu; §Samsung medical center; ∥Seoul national university hospital; ¶Catholic medical center of seoul; **Yonsei medical center; ††Asan medical center; ‡‡Ajou medical center Table 1. Continued 2
10. How do you perform biliary reconstruction in the graft of dual bile ducts with distance of 5∼10 mm between two ducts?
A. One-to-one anastomosis after ductoplasty of the two donor bile ducts.
B. Two-to-one anasomosis without ductoplasty of donor bile ducts
C. Two-to-two anastomosis without ductoplasty of donor bile ducts
D. Other opinion ( )
11. How do you perform biliary reconstruction in the graft of dual bile ducts with distance more than 10 mm between two ducts?
A. One-to-one anastomosis after ductoplasty of the two donor bile ducts
B. Two-to-one anasomosis without ductoplasty of donor bile ducts
C. Two-to-two anastomosis without ductoplasty of donor bile ducts
D. Other opinion ( )
12. How do you overcome big size discrepancy between donor (too small) and recipient (too big) bile duct?
A. DD reconstruction via plication (folding) of the recipi- ent bile duct
B. DD reconstruction after size reduction (i.e., edge sutu- re) of the recipient bile duct
C. DD reconstruction via eversion suture technique of the recipient bile duct
D. DD reconstruction using the recipient cystic duct or HJ E. Other opinion ( )
하였다.
2) 담도 문합법(Table 5)
문합에 사용하는 봉합사는 5개 병원에서 Prolene을 사용하 였고, 4개 병원에서는 PDS를 사용하였다. 구체적인 문합 방식 은 담도 앞벽과 뒤벽 모두 연속 봉합하는 병원이 4개, 뒤벽은 연속 봉합을 하고 앞벽은 단속 봉합을 하는 병원이 2개, 앞뒤 모두 단속 봉합을 하는 병원이 2개였다. 문합 시 7개 병원에서 는 수혜자 담도의 전층을 봉합하였으며, 2개 병원에서는 상피 층만을 봉합하였다. 담도 문합 중 담도관(stent)을 삽입하는지 에 대해서는, 대부분의 경우 사용하는 경우가 3개 병원, 경우 에 따라서 사용하는 경우가 5개 병원, 전혀 사용하지 않는 경 우가 1개 병원이었다. 경우에 따라 사용한다고 답변한 경우 주로 담도 내경이 작거나, 담도가 짧아서 긴장도(tension)가
증가하거나, 담도 문합부가 예각으로 만나 꺾이는 경우 (angulation)에 담도관을 사용하였고, 주로 담도내관(internal stent)를 사용하였다. 담도 문합시 대부분의 경우 담도관을 사 용한다고 답변한 3개 병원에서는 T관이 아닌 I자 모양의 담도 외관(external stent)를 사용한다고 하였다. 사용하는 담도관 의 종류는 모두 silastic 재질이었으며 고무 재질(rubber tube) 을 사용하지 않았다. 담도 문합시 이식편 담도의 크기가 수혜 자 담도 크기에 비해 작은 경우, 9개 병원 모두 수혜자 담도에 단단문합하였다. 수혜자 담도에 문합할 때에 직경 차이를 극 복하는 방법으로 수혜자 담도를 주름지워서 문합하거나, 수혜 자 담도의 점막층만 봉합하거나, 수혜자 담도 일부를 봉합하 여 직경을 줄여 사용하거나, 이식편 담도의 장막층을 문합하 거나, 선택적으로 공장문합법하기도 하였다.
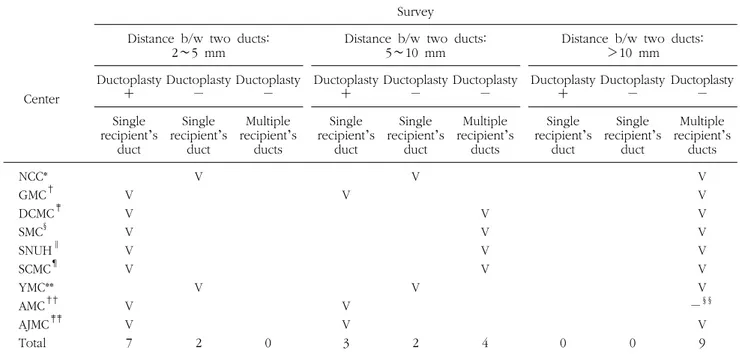
3) 2개 이상의 이식편 담도 문합(Table 6)
이식편에 2개 이상의 담도가 있을 때 각 담도 사이의 간격 에 따라 문합 방법을 달리 선택하였다. 각 담도가 2∼5 mm 간격으로 가까운 경우에는 9개 병원 모두 수혜자 담도 1개에 연결하며, 7개 병원에서는 2개의 담도를 하나로 만드는 이식 편 담도성형술(ductoplasty)을 시행하였다. 이식편 담도가 5
Table 4. Preparation of recipients’ bile duct in adult-to-adult living donor liver transplantation
Center
Survey
Level of resected bile duct Level of anastomosis Microscopic surgery 2nd order 1st order CHD* 2nd order 1st order CHD§§ Rare Sometimes Most NCC*
GMC† DCMC‡ SMC§ SNUH∥ SCMC¶ YMC**
AMC††
AJMC‡‡
Total
V V V
V 4
V V V V V V
6 0
V
1
V V
2
V V V V V V V V 8
V V V V V V V V 8
V
1 0
*National cancer center; †Gil medical center; ‡Catholic medical center of daegu; §Samsung medical center; ∥Seoul national university hospital; ¶Catholic medical center of seoul; **Yonsei medical center; ††Asan medical center; ‡‡Ajou medical center;
§§CHD=common hepatic duct
Table 3. Evaluation and operation of live donor bile duct
Center
Survey
MRCP§§ OPC∥∥ Time of resection of bile duct
during parenchymal division
Rare Sometimes Most Rare Sometimes Most Pre- Mid- Post-
NCC*
GMC† DCMC‡ SMC§ SNUH∥ SCMC¶ YMC**
AMC††
AJMC‡‡
Total
V
V
2 0
V V V V V V V
7 0
V
V V V
4
V V
V V V
5 0
V V V V
4
V V V
V V 5
*National cancer center; †Gil medical center; ‡Catholic medical center of daegu; §Samsung medical center; ∥Seoul national university hospital; ¶Catholic medical center of seoul; **Yonsei medical center; ††Asan medical center; ‡‡Ajou medical center;
§§MRCP=MR cholangiopancreatogratogphy; ∥∥OPC=operative cholangiopraphy
∼10 mm 간격인 경우에는 5개 병원에서는 역시 수혜자 담도 1개에 연결하였고, 4개 병원에서는 2개의 수혜자 담도(좌우간 관, 우전후간관, 담낭관 등)에 각각 연결하였다. 이식편 담도 를 1개의 수혜자 담도에 연결하는 경우 3개 병원에서는 가능 한 한 담도성형술을 시행한다고 하였다. 10 mm 이상 이식편 담도 간격이 먼 경우에는 8개 병원에서 수혜자 담도 2개에
각각 연결하였으며, 1개 병원에서는 담도공장문합술을 시행 하였다.
고 찰
생체 간이식에서 담도 문합 후 발생하는 담도 합병증은 공
Table 5. Biliary reconstruction in adult-to-adult living donor liver transplantation
Center
Survey
Type of thread Mode of anastomosis suture Recipient’s bile duct
layer of anastomosis Use of biliary stent Prolene PDS Interrupted continuous Mixed type§§ Whole Epithelium Rare Sometimes∥∥ Most¶¶
NCC*
GMC† DCMC‡ SMC§ SNUH∥ SCMC¶ YMC**
AMC††
AJMC‡‡
Total
6-0 6-0 6-0
6-0 7-0 5
6-0 6-0 7-0 6-0 4
V V
V 3
V
V V
V 4
V V
V
3
V V V V V V V 7
V
V 2
V
1
V V V V V
5
V
V V 3
*National cancer center; †Gil medical center; ‡Catholic medical center of daegu; §Samsung medical center; ∥Seoul national university hospital; ¶Catholic medical center of seoul; **Yonsei medical center; ††Asan medical center; ‡‡Ajou medical center;
§§Posterior=continuous/anterior: interrupted; ∥∥internal stent; ¶¶external stent
Table 6. Biliary reconstruction in cases with multiple donor bile ducts in adult-to-adult living donor liver transplantation
Center
Survey Distance b/w two ducts:
2∼5 mm Distance b/w two ducts:
5∼10 mm Distance b/w two ducts:
>10 mm Ductoplasty
+ Ductoplasty
− Ductoplasty
− Ductoplasty
+ Ductoplasty
− Ductoplasty
− Ductoplasty
+ Ductoplasty
− Ductoplasty
− Single
recipient’s duct
Single recipient’s
duct
Multiple recipient’s
ducts
Single recipient’s
duct
Single recipient’s
duct
Multiple recipient’s
ducts
Single recipient’s
duct
Single recipient’s
duct
Multiple recipient’s
ducts NCC*
GMC† DCMC‡ SMC§ SNUH∥ SCMC¶ YMC**
AMC††
AJMC‡‡
Total
V V V V V V V 7
V
V
2 0
V
V V 3
V
V
2
V V V V
4 0 0
V V V V V V V
−§§
V 9
*National cancer center; †Gil medical center; ‡Catholic medical center of daegu; §Samsung medical center; ∥Seoul national university hospital; ¶Catholic medical center of seoul; **Yonsei medical center; ††Asan medical center; ‡‡Ajou medical center;
§§Hepaticojejunostomy
여자 및 수혜자의 상태, 허혈 시간등 이식편의 상태, 수술 기 법 등 여러 요인들에 의해 영향을 받는다. 따라서 담도 합병증 을 없앨 수 있는 완전한 수술 술기는 없을 지도 모른다. 그러 나 담도 합병증을 줄일 수 있는 수술 술기의 개선은 가능하리 라 생각되며, 이러한 이유로 여러 병원의 술자들이 여러 방법 들이 제시된 바 있다. 기존 논문들에서 제시된 생체 간이식에 서 담도 합병증을 줄일 수 있는 여러 기술적인 방법들을 종합 해 보면,19-21 먼저 공여자 수술에서 이식편 구득 시 하나의 건 강하고 혈류가 잘 보존된 담도(우간동맥이나 좌간동맥에서 내 려오는 작은 담관 혈류 유지)를 얻는 것이 중요하다. 이를 위 해 공여자 담도 끝부분의 길이를 가능한 짧게 하고, 담도 주위 를 최소한으로 박리하고, 담도 방향과 수직으로 절단한다. 담 도 구조의 여러 해부학적인 변형을 정확히 알기 위해 수술 전 MRCP 또는 OPC를 시행한다. 본 설문 조사 결과에서도 9개 모든 병원에서 병원 특성에 따라 공여자에서 MRCP나 OPC를 시행하여 수술 중 발생할 수 있는 오류를 최소화하였고, 가능 한 한 1개의 건강하고 혈류가 잘 보존된 이식편 담도를 얻기 위해 노력하였다.
성인간 생체 간이식에서는 주로 사용하는 우간은 담도 변형 이 많아서7,22-24 여러 개의 담도가 있는 경우에는 담도 내경이 작은 문제가 있다. 이를 극복하기 위해서 벤치 수술 중 작은 2개(혹은 그 이상)의 담도를 모아서 1개로 만드는 담도성형술 을 하기도 하며,24 작은 담도를 정교하게 문합하기 위해 미세 현미경 하에 수술을 진행하기도 하지만,25 이러한 수술 방법의 변화가 합병증 예방에 도움이 될 지는 아직 이견이 있다. 대부 분의 병원(7개 병원)에서 두 개의 담도가 가까이 있을 때(<5 mm)는 담도성형술을 시행한다고 답하였으나, 두 담도 사이가 5∼10 mm 사이로 떨어져 있는 경우는 4개 병원에서만 담도 성형술을 시행하고, 10 mm 이상 떨어져 있는 경우는 모든 병원에서 무리하게 담도성형술을 하지 않는다고 답하였다.
수혜자 수술에서도 전간절제 시 충분한 길이의 혈류가 잘 유지된 담도를 확보하는 것이 중요하다고 알려져 있다. 수혜 자 간절제 시 확보되는 담도의 수준은 5개 병원에서 1차 분지 수준인 좌우담도를 확보한다고 답하였고, 나머지 4개 병원은 2차 분지 이상의 담도를 확보한다고 답하여 비교적 높은 수준 의 담도를 확보하고 있음을 알 수 있었다. 삼성서울병원에서 는 혈류가 유지되는 높은 수준의 담도를 확보하기 위해 high hilar dissection이라는 수혜자 수술기법을 제안한 바 있다.26 이번 설문에서는 수혜자 담도의 혈류 유지에 관한 기법에 대
해서는 구체적 질의가 이루어지지 않았다.
담도 합병증을 줄이기 위한 문합 방식에 있어서도 논란이 있으나, 기존 연구에서 단속 봉합은 담즙 누출이 많고, 연속 봉합은 담즙 누출이 적은 대신 담도 협착이 많다는 보고가 있 다.27 그 중간으로 후벽은 연속 봉합으로 하고, 전벽은 단속 봉합으로 하는 병합기법을 이용하기도 한다. 국내에서 대부분 이식 병원은 위의 세가지 기법들이 비슷한 비율로 이용되고 있었다.
대개의 병원에서는 담도 문합시 수혜자 담도의 전층을 문합 하는데, 두 병원에서 담도대 담도 문합시 전층을 문합에 이용 하지 않고, 담도상피층을 이용한다고 답하였다. 수혜자의 담 도를 외번시킨 후, 담도상피층을 이용하는 방법은, 수혜자 담 도 말단 전층에 비해 혈류 공급이 비교적 잘 유지된 상피층을 이용한다는 장점이 있다.11,12
담도관 삽입은 한 병원을 제외하고 거의 모든 병원에서 경 우에 따라 혹은 거의 모든 문합에서 사용한다고 답하였다. 거 의 모든 경우에 담도관을 삽입한다고 답한 3개 병원에서는 담 즙을 외부로 배출시키는 I자 외담도관을 사용한다고 답하였 고, 경우에 따라 사용한다고 답한 5개 병원에서는 담도 문합 부를 지나는 짧은 내담도관을 사용한다고 하였다.
문합에 사용되는 실도 비흡수성 봉합사인 Prolene과 흡수 성 봉합사인 PDS가 반반씩 사용되었다. 비흡수성 봉합사는 추후 담도 협착 시 담관 확장 등에 방해가 되는 단점이 있으 나, 문합 부위 염증을 덜 일으켜, 조직 반응을 줄임으로써, 누 출이나 협착을 줄일 수 있다는 이론적인 장점이 있으며,28 흡 수성 봉합사는 몇 개월이 지난 후 봉합사가 녹은 후에는 필요 에 따라 담관이 확장될 수 있는 여지가 있다는 장점이 있다.
성인간 생체 간이식에 있어서 공여자 담도에 대한 준비 방법, 그리고 실제 담도 문합시 어떠한 봉합사를 선택하고, 어떤 층 을 봉합하며, 어떤 수혜자 담도를 선택하여, 몇 개의 담도에, 어떤 방식으로 문합해야 하는지에 대해서 국내 술자들 사이에 서도 이견이 있다. 다만 이러한 간이식 외과의들이 노력이 다 기관 공동 연구를 통해 합의점을 찾고 좋은 성적을 제시할 수 있어야 하겠으며, 본 연구가 이러한 초석이 되기를 기대한다.
참 고 문 헌
1. Furukawa H. Role of endoscopic retrograde cholangiopan- creatography in late biliary tract complications after
orthotopic liver transplantation. J Gastroenterol Hepatol 2000;15:577-578.
2. Calne RY. A new technique for biliary drainage in orthotopic liver transplantation utilizing the gall bladder as a pedicle graft conduit between the donor and recipient common bile ducts. Ann Surg 1976;184:605-609.
3. Iida T, Ogura Y, Oike F, et al. Surgery-related morbidity in living donors for liver transplantation. Transplantation 2010;89:1276-1282.
4. Park JB, Kwon CH, Choi GS, et al. Prolonged cold ischemic time is a risk factor for biliary strictures in duct-to-duct biliary reconstruction in living donor liver transplantation. Trans- plantation 2008;86:1536-1542.
5. Yi NJ, Suh KS, Cho JY, Kwon CH, Lee KU. In adult-to-adult living donor liver transplantation hepaticojejunostomy shows a better long-term outcome than duct-to-duct anastomosis.
Transpl Int 2005;18:1240-1247.
6. Chang JH, Lee IS, Choi JY, et al. Biliary stricture after adult right-lobe living-donor liver transplantation with duct-to-duct anastomosis: longt-term outcome and Its related factors after endoscopic treatment. Gut Liver 2010;4:226-233.
7. Hwang S, Lee SG, Sung KB, et al. Long-term incidence, risk factors, and management of biliary complications after adult living donor liver transplantation. Liver Transpl 2006;12:
831-838.
8. Shah SA, Grant DR, McGilvray ID, et al. Biliary strictures in 130 consecutive right lobe living donor liver transplant recipients: results of a Western center. Am J Transplant 2007;7:161-167.
9. Perkins JD. Biliary tract complications: the most common postoperative complication in living liver donors. Liver Transpl 2008;14:1372-1373.
10. Han JK. Radiologic diagnosis of benign biliary stricture.
Korean J Hepatobiliary Pancreat Surg 2008;12:91-95.
11. Kim BW, Bae BK, Lee JM, et al. Duct-to-duct biliary reconstructions and complications in 100 living donor liver transplantations. Transplant Proc 2009;41:1749-1755.
12. Kim SH, Lee KW, Kim YK, Cho SY, Han SS, Park SJ. Tailored telescopic reconstruction of the bile duct in living donor liver transplantation. Liver Transpl 2010;16:1069-1074.
13. Yi NJ, Suh KS, Lee HW, et al. An artificial vascular graft is a useful interpositional material for drainage of the right anterior section in living donor liver transplantation. Liver Transpl 2007;13:1159-1167.
14. Yi NJ, Suh KS, Lee HW, et al. Improved outcome of adult recipients with a high model for end-stage liver disease score and a small-for-size graft. Liver Transpl 2009;15:496-503.
15. Lee SG, Hwang S, Kim KH, et al. Toward 300 liver transplants a year. Surg Today 2009;39:367-373.
16. Lee SG, Hwang S, Moon DB, et al. Expanded indication criteria of living donor liver transplantation for hepatocellular carcinoma at one large-volume center. Liver Transpl 2008;14:935-945.
17. Moon JI, Kwon CH, Joh JW, et al. Safety of small-for-size grafts in adult-to-adult living donor liver transplantation using the right lobe. Liver Transpl 2010;16:864-869.
18. Hwang S, Lee SG, Lee YJ, et al. Lessons learned from 1,000 living donor liver transplantations in a single center: how to make living donations safe. Liver Transpl 2006;12:920-927.
19. Yi NJ, Suh KS, Cho JY, et al. Three-quarters of right liver donors experienced postoperative complications. Liver Transpl 2007;13:797-806.
20. Kashyap R, Bozorgzadeh A, Abt P, et al. Stratifying risk of biliary complications in adult living donor liver transplan- tation by magnetic resonance cholangiography. Transplan- tation 2008;85:1569-1572.
21. Gunji H, Cho A, Tohma T, et al. The blood supply of the hilar bile duct and its relationship to the communicating arcade located between the right and left hepatic arteries. Am J Surg 2006;192:276-280.
22. Liu CL, Lo CM, Chan SC, Tso WK, Fan ST. The right may not be always right: biliary anatomy contraindicates right lobe live donor liver transplantation. Liver Transpl 2004;10:811-812.
23. Marsh JW, Gray E, Ness R, Starzl TE. Complications of right lobe living donor liver transplantation. J Hepatol 2009;51:715- 724.
24. Fan ST, Lo CM, Liu CL, Tso WK, Wong J. Biliary reconstru- ction and complications of right lobe live donor liver trans- plantation. Ann Surg 2002;236:676-683.
25. Lin TS, Concejero AM, Chen CL, et al. Routine microsurgical biliary reconstruction decreases early anastomotic complica- tions in living donor liver transplantation. Liver Transpl 2009;15:1766-1775.
26. Lee KW, Joh JW, Kim SJ, et al. High hilar dissection: new technique to reduce biliary complication in living donor liver transplantation. Liver Transpl 2004;10:1158-1162.
27. Kasahara M, Egawa H, Takada Y, et al. Biliary reconstruction in right lobe living-donor liver transplantation: comparison of different techniques in 321 recipients. Ann Surg 2006;243:
559-566.
28. Azoulay D, Marin-Hargreaves G, Castaing D, RenéAdam, Bismuth H. Duct-to-duct biliary anastomosis in living related liver transplantation: the Paul Brousse technique. Arch Surg 2001;136:1197-1200.