46
Anatomical Assessment of the Distal Femur and Tibia for Optimal Femoral Rotational Alignment
in Total Knee Arthroplasty
Chong Bum Chang, M.D.1,2, Sang Cheol Seong, M.D.1, Sahnghoon Lee, M.D.1 and Myung Chul Lee, M.D.1
1Department of Orthopedic Surgery, Seoul National University College of Medicine, Seoul,
2Department of Orthopedic Surgery, Seoul National University Bundang Hospital, Seongnam, Korea
Received: September 23, 2009
Revised: (1st) October 11, 2009, (2nd) January 31, 2010 Accepted: February 2, 2010
Corresponding author: Myung Chul Lee, M.D.
Departments of Orthopedic Surgery, Seoul National University College of Medicine, 28, Yeongeon-dong, Jongno-gu, Seoul 110-411, Korea TEL: 82-2-2072-3212, FAX: 82-2-764-2718
E-mail: [email protected]
This study was supported by grant (04-2003-026-0) from the Seoul National University Hospital Research Fund.
Purpose: This study aimed 1) to identify the rotational axis of the femur that provides a balanced 90o flexion space in TKA, 2) to assess the changes in the flexion space in deep flexion, and 3) to assess the changes in rotational alignment, with using the posterior condylar axis (PCA) as a guide, and as the changes are related to asymmetric cartilage erosion of the posterior condyle.
Materials and Methods: The axial MR images of the distal femur in knee extension and the coronal images of the distal femur and the entire tibia at 90 and 130o were examined in 40 healthy adults.
Results: The clinical transepicondylar axis (TEA) provides a balanced 90o flexion space on average. The balanced flexion space in 90o became an asymmetrical space with relative narrowing of the medial side in 130o. Every 1 mm of asymmetrical cartilage erosion between the posterior condyles changed the femoral rotation by approximately 1o when using the PCA as a guide.
Conclusion: This study suggests that the clinical TEA is the rotational reference that provides a balanced flexion space. When using the PCA as a rotational reference, a surgeon should consider the potential change in the rotational angle that is caused by asymmetrical cartilage erosion.
Key Words: Total knee arthroplasty, Femoral component rotation, 90 degree flexion gap, 130 degree flexion gap, Asymmetrical cartilage erosion
INTRODUCTION
Rotational alignment of the femoral component is an
important surgical factor for successful total knee ar- throplasty (TKA)1-3,5,6,18,19). Since an anatomical study demonstrated that the average tibial slope in the frontal plane was 3o of varus versus the mechanical axis of the tibia20), 3o external rotation of the femoral component relative to the posterior condylar surface has been re- garded as reasonable rotational alignment to create a rectangular flexion gap when using the classic bone re- section method. In addition, some degrees of external rotation of the femoral component is well known to be critical to prevent patellofemoral complications such as lateral tracking, subluxation and patellar component
failure1,3,5,6,25). However, there’s controversy in the liter- ature regarding the amount of external rotation and the ideal anatomical axis for optimal rotational alignment of the femoral component2,3,4,7,10,12,14,15,21,23,26,28,29,31,32). The contemporary movement toward the concept of a fixed flexion-extension axis began with TKA, and the fixed axis was reported to closely approximate the epi- condylar axis; thus, the transepicondylar axis (TEA) has attracted attention as an ideal rotational reference that provides functional kinematics10,12,32). Furthermore, sev- eral authors also reported that the TEA most con- sistently recreates a balanced flexion gap18,22,23). Never- theless, two different TEAs, i.e. the surgical TEA and the clinical TEA, have been described in the liter- atures7,11,32). Although more than 3o of discrepancy be- tween the two TEAs was reported9,28,31), controversy still exists regarding the relative merits of the two TEAs, in terms of which one is more optimal2,7,10,12,13,18,19,28,31,32). Because of the traditional 3o external rotation of the femoral component stemming from the previous ana- tomical study20), the posterior condylar axis (PCA) is generally believed to be the reasonable and practical reference axis, which also has been thoroughly in- tegrated into instrumentation systems. However, several studies have demonstrated that 3o external rotation rela- tive to the PCA is not sufficient with respect to both achieving a balanced flexion gap and physiologic pa- tellofemoral tracking3,24,29). In addition, its reliability has been questioned due to individual variations of the pos- terior femoral condyle and the anatomical changes of the condyles in arthritic knees22). Among the anatomical changes of the posterior femoral condyle, it is our anec- dotal experience that asymmetrical cartilage erosion in varus osteoarthritis, that is, the complete loss of carti- lage on the medial femoral condyle with preservation of cartilage on the lateral femoral condyle, is the common- est finding during TKA. For this type of case, as many total knee replacement systems provide PCA guides which have two bars that rest on the medial and lateral posterior condyles to set the rotational angle, we ex-
pected more external rotation of the femoral component than the setting angle of the PCA guides.
Rotational alignment of the femoral component dur- ing deep knee flexion is another concern. Deep knee flexion after TKA has become a major challenge be- cause more patients wish to continue sports and leisure activities that require an adequate range of motion30). Many studies have been performed to identify the opti- mal rotational references that ensure a balanced flexion space at 90o of flexion18,20,22,23,26,29), yet little information is available on optimal rotational alignment for the flex- ion space during deep knee flexion.
This study had three goals: 1) To assess the relation- ships between the femoral component rotation reference axes in normal subjects, and to identify the axis that provide a balanced flexion space at 90o flexion; 2) To assess the changes in the flexion space at 130o flexion for determining the optimal rotational alignment in deep knee flexion; 3) To assess the changes in rotational alignment related to asymmetric cartilage erosion of the posterior condylar surfaces when the PCA is used as a rotational reference.
MATERIALS AND METHODS
Forty normal knees in 20 female and 20 male healthy volunteers were evaluated using MRI (1.5 Tesla, Sym- phony, Siemens Medical Solutions, Erlangen, Germany).
None of the subjects had a history of knee trauma or infection or any obvious knee deformity. The male sub- jects had a mean age of 22.1 years (range: 20 to 24 years), a mean weight of 68.2 kg (range: 58 to 86 kg), a mean height of 173.6 cm (range: 164 to 184 cm). The female subjects had a mean age of 25.8 years (range:
23 to 31 years), a mean weight of 51.4 kg (range: 42 to 66 kg), a mean height of 162.5 cm (range: 157 to 173 cm). We obtained axial MR images by using a cus- tom knee coil with the knees in full extension, while obtained the coronal MR images of the whole length of the tibia with the distal femur at 90 and 130o of knee
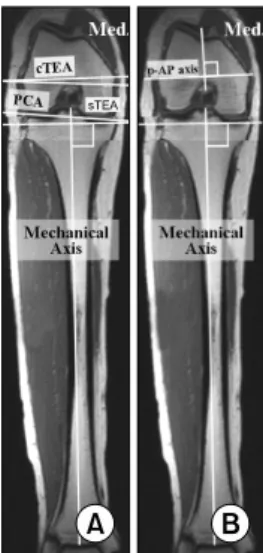
Fig. 1. MRI scans show the coronal views of the distal femur and entire tibia at 90o of knee flexion (the images were reconstructed using suitable images that contained the reference points). cTEA: clinical transepicondylar axis - a line connecting the vertices of the medial and lateral epicon- dyles. sTEA: surgical transepicondylar axis - a line connecting the sulcus of the medial epicondyle and the vertex of the lateral epicondyle. PCA: posterior condylar axis - a line connecting the vertices of the articular surfaces on the medial and lateral posterior femoral condyles. AP axis: - a line through the deepest part of the patellar groove anteriorly and the center of the intercondylar notch posteriorly. (A) Assessment of the relationships between the line perpen- dicular to the tibial mechanical axis and the two trans- epicondylar axes and the posterior condylar axis. (B) Assessment of the relationship between the line perpen- dicular to the tibial mechanical axis and the line perpen- dicular to the AP axis (the p-AP axis).
flexion by using a body coil. During the whole exami- nation, the flexion angle of the knee was controlled us- ing a goniometer by one of the authors. The MR im- ages at 90 and 130o of knee flexion were obtained using the following protocol: two signals were acquired using the coronal T1-weighted spin echo (SE) mode (repetition time msec/echo time msec, 750/20) with a 2-mm section thickness over a 400-mm field of view (adjusted according to leg length), and a 512×512 matrix.
The measurements were subsequently carried using the digital images on a 21-inch LCD monitor (ME315L;
Totoku, Nagaoka, Japan) with employing M-viewTM ver.
4.0 (Marotech, Seoul, Korea), the working software of the picture archiving and communication system (PACS).
One of the study’s authors performed all the measure- ments and the intra-observer reliability of the obtained measurements was assessed by repeating the measure- ments three times at weekly intervals. The average an- gles of the three measurements between the individual axes were regarded as the true values.
This study was approved by the institutional review board of the hospital.
1. Evaluation of relationship between the femo- ral rotational axes and the flexion space at 90 degrees
To determine which axis most consistently provides a balanced flexion space at 90o flexion, the angles be- tween the four femoral axes, i.e. the clinical and surgi- cal TEAs, the anteroposterior axis of the distal femur (AP axis) and the PCA, and the line perpendicular to the tibial mechanical axis (p-TMA), which is parallel to the tibial cutting plane in conventional TKA, were measured on the images acquired at 90o of knee flexion.
To define the p-TMA, the mechanical axis of the tibia was drawn first as a line connecting the center of the talus and the center of the intercondylar eminences of the tibia, and then the line perpendicular to the tibial mechanical axis was drawn from the medial edge of the medial tibial plateau (Fig. 1A, B).
2. Evaluation of difference in the flexion space between 90 and 130 degrees of knee flexion
To evaluate changes in the flexion space during deep knee flexion, we measured the angles between the clini- cal TEA and p-TMA at 130o of knee flexion (Fig. 2).
By comparing this data with that acquired at 90o flex- ion, we assessed the change in rotational alignment on further flexing the knees from 90 to 130o.
Fig. 2. MRI scans showing coronal views of the distal femur and the entire tibia at 90 and 130o of knee flexion (the images were reconstructed from the images that contained the reference points).
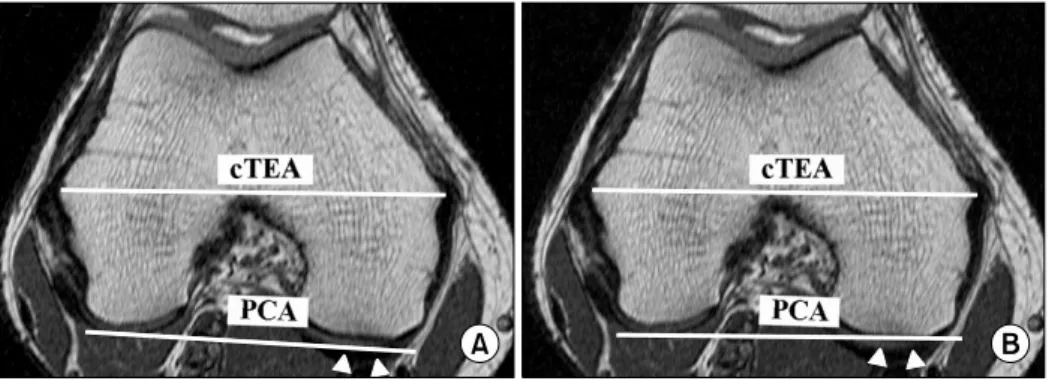
Fig. 3. The MR images to assess the changes in the rotational alignment, as determined by PCA, due to the asymmetric cartilage erosion that’s expected in varus osteoarthritis patients. (A) The PCA was drawn with assuming the preservation of cartilage of the lateral and medial (arrow heads) condyles. (B) The PCA was drawn assuming the complete erosion of the medial side cartilage (arrow heads) with the preserved lateral side. PCA: Posterior condylar axis, cTEA: Clinical transepicondylar axis.
3. Evaluation of the changes on the rotational alignment determined by the PCA due to asymmetric cartilage erosion
To assess the rotational alignment changes related to asymmetrical cartilage erosion of the posterior femoral condyles, which is expected in varus osteoarthritis, we measured the angle between the clinical TEA and the PCA with assuming complete erosion of the articular cartilage on the posterior part of the medial femoral
condyle with preservation of the lateral femoral condyle cartilage (Fig. 3A, B). We then calculated the amount of rotational angle change relative to the differences of the eroded cartilage thickness between the medial and lateral femoral condyles when the PCA was used as a reference axis.
4. Reliability tests and statistical analysis
The intra-rater reliability for all measurements was assessed using the intraclass correlation coefficient (ICC) and found that the measurements agreed well (ICC=
0.77∼0.89). Student’s t-test was used to determine whether the angles between the rotational references in the male group were different with those in the female groups. In addition, paired t-test was used to examine the significance of changes in the angle of the clinical TEA vs. the p-TMA between 90o and 130o of knee flexion in each gender. All the statistical analysis was performed using SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Among the evaluated axes, the clinical TEA most con- sistently showed a parallel relationship with the p-TMA at 90o of knee flexion, which means a balanced flexion space at 90o. The mean angles between the clinical TEA
Table 1. The Angles between the Line Perpendicular to the Tibial Mechanical Axis and the Four Femoral Rotational Axes at 90 Degrees of Flexion
Reference axis
Male Female
p-value*
Mean SD (range) Mean SD (range)
cTEA† sTEA† PCA† p-AP axis†
0.8o 3.9o 5.1o 0.9o
1.3o (−2.2∼2.7o) 1.3o (1.5∼5.9o) 1.6o (1.7∼8.2o) 2.6o (−4.8∼5.0o)
0.2o 4.0o 6.6o 0.2o
2.2o (−5.6∼4.3o) 2.1o (−0.7∼6.9o) 2.2o (1.4∼10.5o) 2.8o (−5.0∼6.0o)
0.335 0.982 0.020 0.434 SD: Standard deviation, cTEA: Clinical transepicondylar axis, sTEA: Surgical transepicondylar axis, PCA: Posterior condylar axis, p-AP axis: Perpendicular line to the anteroposterior axis of the femur.
*The p-value with statistical significance (p<0.05) are shown in bold. †The plus value indicates that each axis requires external rotation to be set parallel to the line perpendicular to the tibial mechanical axis.
Table 2. The Relationship between the Perpendicular Line of the Tibial Mechanical Axis and the Clinical TEA as the Knee Flexed is from 90 Degrees to 130 Degrees
Male Female
p-value
Mean SD (range) Mean SD (range)
90o flexion*
130o flexion*
Amount of change†
0.8o 3.1o 2.3o
1.3o (−2.2∼2.7o) 1.0o (0.0∼4.2o) 0.7o (1.1∼3.8o)
0.2o 2.2o 2.0o
2.2o (−5.6∼4.3o) 2.4o (−3.1∼8.4o)
0.6o (1.2∼4.1o)
0.335 0.171 0.211 SD: Standard deviation.
*The plus valueindicates that the clinical TEA requires external rotation to be set parallel to the line perpendicular to the tibial mechanical axis, †The changes are statisticallysignificant (p<0.001 in both genders).
and the p-TMA were 0.8o (range: −2.2 to 2.7, SD:
1.3), in the men and 0.4o (range: −2.0 to 4.3, SD: 1.8) in the women (the plus value indicates that the clinical TEA requires external rotation to adopt a position par- allel to the p-TMA). The average angles between the posterior condylar axis (PCA) and the p-TMA were 5.1o in the men and 6.6o in the women (Table 1).
Compared with the relationship at 90o flexion, the clinical TEA was significantly internally rotated relative to the p-TMA during deep knee flexion (p<0.001 in both gender), which means that relative medial flexion space narrowing occurred compared to the lateral flex- ion space. The mean angles of internal rotation were 2.3o in the men and 2.0o in the women (Table 2).
When assuming the presence of expected asym-
metrical cartilage erosion on the posterior condyles in varus osteoarthritis, the average changes of the clinical TEA/PCA angles were 1.9o in both genders (Table 3);
the measured average thicknesses of the cartilage on the posterior part of the medial femoral condyle on the MR imaging was 1.8 mm in the men and 1.6 mm in the women. Therefore, a 1mm difference of cartilage ero- sion of the posterior condyles causes a change of 1.1o of rotation in the men and 1.2o in the women when using a PCA guide with two bars that rest on the medial and lateral posterior condyles to set the femoral component rotation. Based on the amount of change, the calculated average angles between the PCA and the p-TMA that were expected in varus osteoarthritis were 3.3o in the men and 4.7o in the women (Table 3).
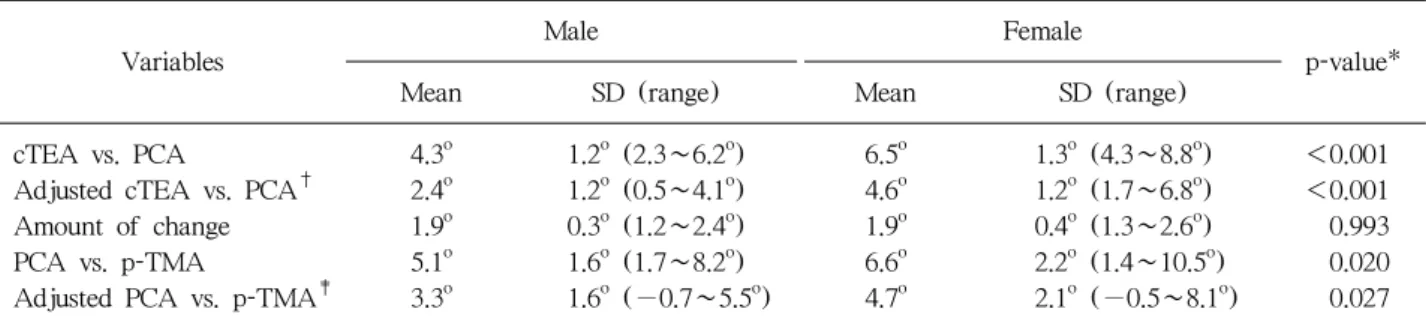
Table 3. Comparison of Angles between the Clinical TEA and the PCA, and the PCA and the Line Perpendicular to the Tibial Mechanical Axis (p-TMA) before, and after Assuming Asymmetrical Cartilage Erosion on Posterior Condyles Expected in Varus Osteoarthritis
Variables
Male Female
p-value*
Mean SD (range) Mean SD (range)
cTEA vs. PCA
Adjusted cTEA vs. PCA† Amount of change PCA vs. p-TMA
Adjusted PCA vs. p-TMA‡
4.3o 2.4o 1.9o 5.1o 3.3o
1.2o (2.3∼6.2o) 1.2o (0.5∼4.1o) 0.3o (1.2∼2.4o) 1.6o (1.7∼8.2o) 1.6o (−0.7∼5.5o)
6.5o 4.6o 1.9o 6.6o 4.7o
1.3o (4.3∼8.8o) 1.2o (1.7∼6.8o) 0.4o (1.3∼2.6o) 2.2o (1.4∼10.5o) 2.1o (−0.5∼8.1o)
<0.001
<0.001 0.993 0.020 0.027 SD: Standard deviation, cTEA: Clinical transepicondylar axis, PCA: Posterior condylar axis.
*The p-value with statistical significance (p<0.05) are shown in bold. †The angle between the cTEA and the PCA measured on the axial MR imaging assuming complete erosion of the articular cartilage on the posterior part of the medial femoral condyle with preservation of the lateral femoral condyle cartilage. ‡The calculated average angles between the PCA and the p-TMA based on the amount of change between the cTEA and the PCA.
DISCUSSION
Despite that there is more than 3o of discrepancy be- tween the two TEAs9), it’s still debatable which is the more reproducible and functional axis, i.e., the clinical or the surgical TEA2,7,10,12,18,28,31,32). Regarding the func- tional aspect of the patellofemoral joint, Akagi et al.
suggested that the clinical TEA might be closer to the functional axis for patellofemoral articulation because the average AP axis is perpendicular to the clinical TEA2,28), which was also confirmed in our previous study9). Concerning the flexion gap, some authors have reported that the surgical TEA most consistently recre- ates a balanced flexion gap, based on the intraoperative measurement data22), whereas others have demonstrated that the clinical TEA has a parallel relationship with the line perpendicular to the tibial mechanical axis, which corresponds with our results18,23).
Our assessments of the MR images acquired at 130o of flexion implies that even a symmetrical flexion space at 90o changes to become asymmetrical with narrowing of the medial flexion gap relative to the lateral gap for TKA. We found a similar phenomenon by comparing the measurements of the medial and lateral flexion gaps at 90 and 130o in 20 osteoarthritic patients (36 knees),
who participated in another rotational alignment study with performing TKA. The obtained measurements showed that a flexion space that’s balanced at 90o be- comes asymmetric with narrowing of the medial flexion gap at 130o of flexion (mean: 2.7 mm, SD: 1.2 mm, range: 1∼6 mm)8). Having reviewed the available data, we are concerned that aligning the femoral component to the surgical TEA potentially aggravates such an im- balance with the knee in deep flexion, which might lead to excessive stress on the medial side of the tibial insert after TKA, or this requires excessive medial soft tissue release that’s more than physiologic tension, and this might lead to flexion instability after TKA. Taken to- gether, aligning the femoral component to the clinical TEA, rather than the surgical TEA, would be advanta- geous in terms of restoration of patellofemoral kine- matics and balancing the flexion gap not only at 90o but also in deep flexion during TKA.
Traditionally, 3o of external rotation relative to the PCA is generally regarded as reasonable rotational alignment to create a rectangular flexion gap when us- ing the classic bone resection method20). In contrast, Tang et al. found that the medial inclination of the ti- bial plateau in Chinese patients was greater than the commonly reported 3o, suggesting that the tibial slope in
Fig. 4. Photograph showing the resected distal femur of a patient with varus osteoarthritis. Complete loss of cartilage on the medial femoral condyle (arrow) with preservation of cartilage on the lateral femoral condyle (arrow head) was observed.
the frontal plane might be race dependent29). We also found that the mean external rotation of 6.6o in women and 5.1o in men relative to the PCA provides a rec- tangular flexion gap at 90o, which are 2 or 3o more de- grees of external rotation compared to the traditional 3o relative to the PCA. However, we found that, approx- imately, every 1 mm of asymmetrical cartilage erosion can change the femoral rotation by 1o when using a PCA guide. Considering the majority of the patients warranting TKA have advanced varus OA of the knee, which would have erosion of the cartilage on the medial posterior condyle with relatively intact lateral condyle (Fig. 4), a surgeon can expect that aligning component rotation using a PCA guide in these patients caused more external rotation relative to the setting angle of the PCA guides. In view of this finding, conventional 3o of external rotation relative to the PCA would be close to an optimal angle in advanced varus OA of the knee, which is conducive to setting the femoral-component ro- tation closer to the clinical TEA.
We believe that the data presented by this study is useful for determining the optimal rotational alignment of the femoral component, and especially in an Asian population. However, as there are considerable in-
dividual deviations, these anatomic variations should be considered when treating individual knees. To assess the rotational profile of the individual knees before TKA, MRI or computed tomography would be the most useful tools. However, routine use of these methods has its drawbacks, which include high cost and/or radiation.
Instead, the use of recently developed axial radiographs, which allow measurement of the angle between the PCA and TEA16,27), might be a practical alternative method to assess the rotational profile of the individual knees. Nevertheless, as the axial radiographs only pro- vide the angle between the TEA and the PCA as a bo- ny geometry, operative information on the asymmetrical cartilage erosion should be considered when final rota- tional angle was determined during TKA.
Several limitations should be noted in this study. A major limitation involved that our study was conducted in the young healthy volunteers, thus the results may be different from those in the osteoarthritic patients.
However, our another study found that the relationship among the rotational axes in the osteoarthritic patients was almost identical with the results in this study8).
Furthermore, most related studies which have been per- formed in Asian countries have reported similar rela- tionships of rotational axes with our study1,2,17,18,21,28,29,31,32). Thus, our findings would not be unique in young healthy subjects. Another limitation is that we did not consider mechanical alignment during our study.
Although our study subjects had no significant de- formity of their lower limbs (mean anatomic tibiofe- moral angles: valgus 4.2o, SD: 1.7, range: valgus 1o to 7o), as individual variations in the tibial and femoral mechanical alignments may influence the flexion gap conditions, consideration of the mechanical alignments might provide additional information. Finally, intra-ob- server reliabilities of the measurements in this study were satisfactory, but as one examiner carried out all measurements, we cannot comment on inter-observer reliability.
CONCLUSION
Our study suggests that the clinical TEA, rather than the surgical TEA, would be the rotational reference provides a more balanced flexion space not only in 90o but also in deep knee flexion. When using the PCA as a rotational reference, a surgeon should consider the po- tential change in the rotational angle caused by asym- metrical cartilage erosion.
REFERENCES
1. Akagi M, Matsusue Y, Mata T, et al: Effect of rotational alignment on patellar tracking in total knee arthroplasty. Clin Orthop Relat Res, 366: 155-163, 1999.
2. Akagi M, Yamashita E, Nakagawa T, Asano T, Nakamura T: Relationship between frontal knee align- ment and reference axes in the distal femur. Clin Orthop Relat Res, 388: 147-156, 2001.
3. Anouchi YS, Whiteside LA, Kaiser AD, Milliano MT: The effects of axial rotational alignment of the femoral component on knee stability and patellar tracking in total knee arthroplasty demonstrated on autopsy specimens. Clin Orthop Relat Res, 287:
170-177, 1993.
4. Arima J, Whiteside LA, McCarthy DS, White SE:
Femoral rotational alignment, based on the anter- oposterior axis, in total knee arthroplasty in a valgus knee. A technical note. J Bone Joint Surg Am, 77:
1331-1334, 1995.
5. Barrack RL, Schrader T, Bertot AJ, Wolfe MW, Myers L: Component rotation and anterior knee pain after total knee arthroplasty. Clin Orthop Relat Res, 392: 46-55, 2001.
6. Berger RA, Crossett LS, Jacobs JJ, Rubash HE:
Malrotation causing patellofemoral complications after total knee arthroplasty. Clin Orthop Relat Res, 356:
144-153, 1998.
7. Berger RA, Rubash HE, Seel MJ, Thompson WH, Crossett LS: Determining the rotational alignment of the femoral component in total knee arthroplasty using the epicondylar axis. Clin Orthop Relat Res, 286:
40-47, 1993.
8. Chang CB, Seong SC, Lee S, Yoo JH, Han I, Lee MC: The influence of femoral component rotation on the flexion gap in deep knee flexion. presented in 52nd Orthopaedic research society meeting, 2006.
9. Chang CB, Seong SC, Lee S, Yoo JH, Rhee SH, Lee MC: Anatomical assessment of distal femur for optimal femoral component rotational alignment in TKA. J Korean Orthop Assoc, 40: 882-888, 2005.
10. Churchill DL, Incavo SJ, Johnson CC, Beynnon BD: The transepicondylar axis approximates the optimal flexion axis of the knee. Clin Orthop Relat Res, 356:
111-118, 1998.
11. Griffin FM, Math K, Scuderi GR, Insall JN, Poilvache PL: Anatomy of the epicondyles of the distal femur: MRI analysis of normal knees. J Arthroplasty, 15: 354-359, 2000.
12. Hollister AM, Jatana S, Singh AK, Sullivan WW, Lupichuk AG: The axes of rotation of the knee. Clin Orthop Relat Res, 290: 259-268, 1993.
13. Insall JN, Scuderi GR, Komistek RD, Math K, Dennis DA, Anderson DT: Correlation between condylar lift-off and femoral component alignment. Clin Orthop Relat Res, 403: 143-152, 2002.
14. Jenny JY, Boeri C: Low reproducibility of the intra- operative measurement of the transepicondylar axis during total knee replacement. Acta Orthop Scand, 75:
74-77, 2004.
15. Jerosch J, Peuker E, Philipps B, Filler T: Inter- individual reproducibility in perioperative rotational alignment of femoral components in knee prosthetic surgery using the transepicondylar axis. Knee Surg Sports Traumatol Arthrosc, 10: 194-197, 2002.
16. Kanekasu K, Kondo M, Kadoya Y: Axial radio- graphy of the distal femur to assess rotational align- ment in total knee arthroplasty. Clin Orthop Relat Res, 434: 193-197, 2005.
17. Matsuda S, Matsuda H, Miyagi T, Sasaki K, Iwamoto Y, Miura H: Femoral condyle geometry in the normal and varus knee. Clin Orthop Relat Res, 349: 183-188, 1998.
18. Matsuda S, Miura H, Nagamine R, Urabe K, Mawatari T, Iwamoto Y: A comparison of rotational landmarks in the distal femur and the tibial shaft. Clin Orthop Relat Res, 414: 183-188, 2003.
19. Miller MC, Berger RA, Petrella AJ, Karmas A,
Rubash HE: Optimizing femoral component rotation in total knee arthroplasty. Clin Orthop Relat Res, 392:
38-45, 2001.
20. Moreland JR, Bassett LW, Hanker GJ: Radiographic analysis of the axial alignment of the lower extremity. J Bone Joint Surg Am, 69: 745-749, 1987.
21. Nagamine R, Miura H, Inoue Y, et al: Reliability of the anteroposterior axis and the posterior condylar axis for determining rotational alignment of the femoral component in total knee arthroplasty. J Orthop Sci, 3:
194-198, 1998.
22. Olcott CW, Scott RD: The ranawat award. Femoral component rotation during total knee arthroplasty. Clin Orthop Relat Res, 367: 39-42, 1999.
23. Poilvache PL, Insall JN, Scuderi GR, Font-Rodriguez DE: Rotational landmarks and sizing of the distal femur in total knee arthroplasty. Clin Orthop Relat Res, 331: 35-46, 1996.
24. Rhoads DD, Noble PC, Reuben JD, Tullos HS: The effect of femoral component position on the kinematics of total knee arthroplasty. Clin Orthop Relat Res, 286:
122-129, 1993.
25. Singerman R, Pagan HD, Peyser AB, Goldberg VM:
Effect of femoral component rotation and patellar design on patellar forces. Clin Orthop Relat Res, 334: 345- 353, 1997.
26. Stiehl JB, Cherveny PM: Femoral rotational alignment using the tibial shaft axis in total knee arthroplasty.
Clin Orthop Relat Res, 331: 47-55, 1996.
27. Takai S, Yoshino N, Isshiki T, Hirasawa Y:
Kneeling view: a new roentgenographic technique to assess rotational deformity and alignment of the distal femur. J Arthroplasty, 18: 478-483, 2003.
28. Tanavalee A, Yuktanandana P, Ngarmukos C: Surgical epicondylar axis vs anatomical epicondylar axis for rotational alignment of the femoral component in total knee arthroplasty. J Med Assoc Thai, 84(Suppl 1):
S401-S408, 2001.
29. Tang WM, Zhu YH, Chiu KY: Axial alignment of the lower extremity in Chinese adults. J Bone Joint Surg Am, 82: 1603-1608, 2000.
30. Weiss JM, Noble PC, Conditt MA, et al: What functional activities are important to patients with knee replacements? Clin Orthop Relat Res, 404: 172-188, 2002.
31. Yoshino N, Takai S, Ohtsuki Y, Hirasawa Y:
Computed tomography measurement of the surgical and clinical transepicondylar axis of the distal femur in osteoarthritic knees. J Arthroplasty, 16: 493-497, 2001.
32. Yoshioka Y, Siu D, Cooke TD: The anatomy and functional axes of the femur. J Bone Joint Surg Am, 69: 873-880, 1987.
인공 슬관절 전치환술 시 적절한 대퇴 치환물의 회전 정렬을 위한 원위 대퇴골과 경골의 해부학적 고찰
1서울대학교 의과대학 정형외과학교실, 2분당서울대학교병원 정형외과
장종범
1,2ㆍ성상철
1ㆍ이상훈
1ㆍ이명철
1목적: 본 연구는 1) 인공 슬관절 전치환술 시 균형잡힌 90o 굴곡 간격을 위한 대퇴 회전 정렬의 축과,
2) 90o와 130o 굴곡에서의 굴곡 간격 사이의 변화 및 3) posterior condylar axis (PCA) 이용 시 후방 대퇴과 의 비 대칭적 연골 소실에 의한 대퇴 회전 정렬의 변화를 알아보고자 하였다.
대상 및 방법: 건강한 성인 40명의 원위 대퇴골의 축상면 자기공명영상과 90o 굴곡 및 130o 굴곡 위에서의 원위 대퇴골과 경골 전장의 관상면 자기공명영상을 이용, 분석하였다.
결과: 임상적 transepicondylar axis (TEA)가 평균적으로 균형 잡힌 90도 굴곡 간격을 얻을 수 있는 축이었 으며, 90o에서 균형잡힌 굴곡 간격은 130o에서는 내측 구획이 외측 구획에 비하여 상대적으로 좁아지는 비대칭적인 간격이 되었다. PCA를 이용한 회전 정렬은 양측 후방 대퇴과의 비대칭적 연골 소실 1 mm당 약 1o의 변화가 생겼다.
결론: 임상적 TEA는 균형 잡힌 굴곡 간격을 얻는데 유리한 대퇴 회전 정렬 축임을 시사하며, PCA를 이용하여 대퇴 치환물의 회전 정렬을 정할 때 내, 외측 구획의 연골 소실 상태의 차이에 따라 회전 정렬이 변할 수 있음을 고려해야 한다.
색인 단어: 인공 슬관절 전치환술, 대퇴 치환물의 회전 정렬, 90o 굴곡 간격, 130o 굴곡 간격, 비대칭적 연골 마모