INTRODUCTION
Reconstructive surgical soft tissue coverage of the distal leg and ankle region is a challenge due to paucity of adjacent soft tissues. Although conventional local flaps such as sural flap or free flap could be safely used with good results, surgeons have to consider the donor site morbidity while choosing the best reconstructive option for the patients.
Nowadays, with wide application of perforator flaps in lower leg reconstruction, we can mainly rely on the perforators from the three main lower leg arteries: posterior tibial artery perforator (PTAP), peroneal artery perforator (PAP), and
anterior tibial artery perforator (ATAP). Among them, PAP flap (PAPF) and PTAP flap (PTAPF) are most commonly used for the reconstructions and the PAPF use has been reported twice as much as that of PTAPF.1 When considering the various anatomical advantages of PTAP over PAP, the option for applying PTAPF should not be overlooked.
Islanded propeller flap has become the method of choice for reconstruction of the distal lower leg defects since its introduction in 1991 by Hyakusoku et al.2 This conventional propeller form also has a shortcoming aesthetically in that it leaves a long scar on the proximal lower leg. However, island flap elevated from just next to the defect, though it may not be
Close-by Islanded Posterior Tibial Artery Perforator Flap:
For Coverage of the Ankle Defect
Sujin Bahk, SeungHwan Hwang, Chan Kwon, Euicheol C. Jeong1, Su Rak Eo*
Department of Plastic and Reconstructive Surgery, Dongguk University Ilsan Medical Center, Goyang,
1Department of Plastic Surgery, SMG-SNU Boramae Medical Center, Seoul, Korea
CC This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright © 2016 by the Korean Society for Microsurgery. All Rights Reserved.
Received April 24, 2016 Revised July 31, 2016 Accepted August 17, 2016
*Correspondence to: Su Rak Eo
Department of Plastic and Reconstructive Surgery, Dongguk University Ilsan Medical Center, 27 Dongguk-ro, Ilsandong-gu, Goyang 10326, Korea
Tel: +82-31-961-7342 Fax: +82-31-961-7347 E-mail: [email protected]
ORCID: http://orcid.org/0000-0002-4221-2613
Financial support: None.
Conflict of interest: None.
Purpose: Soft tissue coverage of the distal leg and ankle region represents a surgical challenge. Beside various local and free flaps, the perforator flap has recently been replaced as a reconstructive choice because of its functional and aesthetic superiority. Although posterior tibial artery perforator flap (PTAPF) has been reported less often than peroneal artery perforator flap, it also provides a reliable surgical option in small to moderate sized defects especially around the medial malleolar region.
Materials and Methods: Seven consecutive patients with soft tissue defect in the ankle and foot region were enrolled. After Doppler tracing along the posterior tibial artery, the PTAPF was elevated from the adjacent tissue. The average size of the flap was 28.08±9.31 cm2 (range, 14.25 to 37.84 cm2). The elevated flap was acutely rotated or advanced.
Results: Six flaps survived completely but one flap showed partial necrosis because of overprediction of the perforasome. No donor site complications were observed during the follow-up period and all seven patients were satisfied with the final results.
Conclusion: For a small to medium-sized defect in the lower leg, we conducted the close- by islanded PTAPF using a single proper adjacent perforator. Considering the weak point of the conventional propeller flap, this technique yields much better aesthetic results as a simple and reliable technique especially for defects of the medial malleolar region.
Key Words: Surgical flaps, Perforator flap, Posterior tibial artery, Ankle
ARMS
Archieves of Reconstructive Microsurgery https://doi.org/10.15596/ARMS.2016.25.2.37suitable for large defects, can show much better aesthetic results when covering small to moderated sized defects. Accordingly we suggest a simple and reliable method using a small islanded PTAPF close by the defect as ideal for the reconstruction of relatively small distal leg and ankle defects.
MATERIALS AND METHODS
Seven patients underwent islanded PTAPF between 2013 and 2014. Surgical indication was limited by size and location of the defect. Only small to moderate-sized defects around the ankle area, especially medial malleolar region and achilles tendon-exposed region were selected for this flap technique.
Angiography was performed before the reconstruction to exclude vascular anomalies. Patient details are summarized in Table 1.
Surgical technique
Preoperatively, perforators of the posterior tibial artery (PTA) near the defect were marked on the skin with hand- held Doppler. The patient was positioned in supine position and a temporary elliptical design was made around the medial malleolar region near the defect. A pneumatic tourniquet was cautiously placed around the thigh to prevent excess bleeding.
Under loupe magnification, the margin of the flap closer to the defect was raised first and dissection proceeded in a suprafascial plane while paying attention to the expected location of the traced perforator. Once a suitable perforator was found, the flap was again designed adjacent to the defect while the main perforator was located at the center of the flap. Designed outline of the flap was incised and islanded on the selected perforator.
Excessive skeletonization of the perforator was avoided and moderate intermuscular dissection was performed to obtain adequate release and additional length. After complete elevation of the flap, perfusion within the flap was evaluated and it was rotated randomly according to the defect. Secondary defects were covered with split thickness skin graft in two cases and closed primarily in one case.
RESULTS
Seven cases of islanded PTAPF were performed. Mean operation time was 79 minutes. Size of the flaps varied from
Table 1. Summary of the patient characteristics Patient No.Age (yr)SexCause of injuryLocation of defectDefect size (cm2 )Flap dimension (cm2 )Exposed structureComplication 158MaleTraffic accidentAnteromedial lower tibial area14.7037.84Extensor hallucis longusNone 229MaleTraffic accidentAchilles tendon (heel)4.2914.25Achilles tendonMinimal wound dehiscence 359FemaleTraffic accidentMedial malleolar area10.33 with adjacent skin defect35.79Metal hardware and tibiaPartial venous congestion 445MaleBurn injuryAchilles tendon (heel)12.1034.58Achilles tendonNone 556MaleTraffic accidentMedial malleolar area11.4626.37Metal hardware and tibiaNone 650MaleWound infectionMedial malleolar area9.4530.71TibiaNone 759MaleTraffic accidentMedial malleolar area6.9317.02TibiaNone
14.25 to 37.84 cm2. Average size of the flap was 28.08±9.31 cm2. Out of 7 flap donor sites, 4 were repaired by primary closure and 3 were repaired with skin grafting. Small marginal wound dehiscence was present in Case 2 and it was managed with simple re-suture. Complications like osteomyelitis or soft tissue infection were not encountered. However, patient in Case 3 developed partial flap necrosis due to venous congestion, which was managed with subsequent debridement and local transposition flap. Short leg splinting was maintained for 3 weeks and then ambulation was started. No other flap complications were encountered and patients were satisfied with the final results.
Case 1
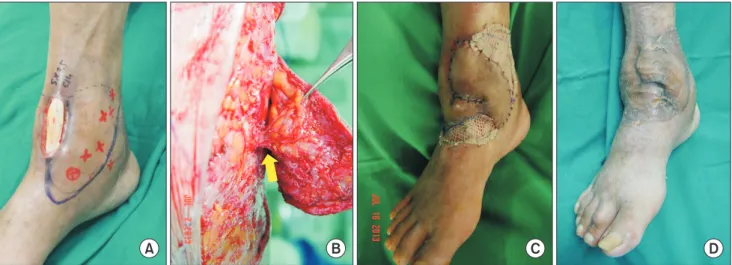
A 58-year-old man developed a 14.70 cm2 soft tissue defect
with exposure of the extensor hallucis longus tendon after repetitive course of cellulitis (Fig. 1A). Debridement was performed and the defect was covered with a 37.84 cm2 island PTAPF that was elevated and 60-degree rotated. Secondary defect was covered with split thickness skin graft (Fig. 1B, C).
Case 2
A 29-year-old man was referred to our department due to the soft tissue defect of the posterior ankle. He had been injured in a traffic accident and Achilles tendon of the left ankle was ruptured. He was treated in a local clinic by repetitive tenorrhaphy and primary closure. But the wound dehiscence progressed resulting in a 4.29 cm2 sized defect (Fig. 2A). A 14.25 cm2 sized PTAPF was elevated from a near site and advanced posteriorly to cover the defect (Fig. 2B). A branch of
A B C D
Fig. 1. A case of anterior ankle defect. (A) Ankle defect with exposure of extensor hallucis longus tendon. (B) Perforator from posterior tibial artery (arrow).
(C) Immediate appearance after surgery. (D) Appearance of 3 weeks after surgery.
A B C D E
Fig. 2. A case of posterior ankle defect. (A) Defect with exposure of the Achilles tendon. (B) Perforator from posterior tibial artery (arrow). (C) Close-by flap is advanced posteriorly and a branch of the small saphenous vein is preserved. (D) Immediate appearance after surgery. (E) Appearance of 3 weeks after surgery.
the small saphenous vein was preserved during the dissection for the augmentation of venous drainage (Fig. 2C). Secondary defect was closed primarily without additional skin graft (Fig.
2D).
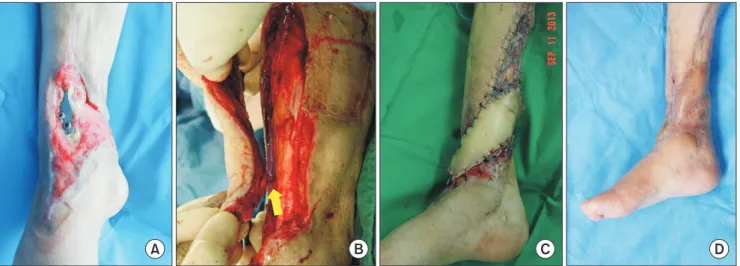
Case 3
A 59-year-old woman was referred to our department with a 10.33 cm2 sized soft tissue defect accompanying exposure of the metal fixator after the surgery for an open tibial fracture (Fig. 3A). The defect had been previously managed with PAPF but partial necrosis was encountered. After the course of debridement and conservative treatment, conventional propeller flap based on PTAP was planned. Longitudinal, 35.79 cm2 sized flap was elevated in a suprafascial plane from her middle lower leg and 120-degree rotated to cover the defect (Fig.
3B). Secondary defect was covered with split thickness skin graft (Fig. 3C). However, partial flap necrosis was encountered and this was managed with local transposition flap afterwards.
DISCUSSION
Since Taylor3 introduced the concept of angiosomes, various techniques of perforator based local flaps in the leg have been developed.4-6 Main advantage of this procedure over the conventional flap resides in the preservation of the source vessel, high mobility and minimal donor site morbidity, avoiding the debulking procedure and maintaining high
mobility. It also provides for a like-for-like tissue in color, texture and thickness that is very similar to the missing tissue. For the technique, we simply search for suitable perforators in close proximity to the defect in the foot and ankle region and we describe as being “close-by”. Harvesting the local perforator flap requires microsurgical dissection, however, it does not require vascular anastomosis and can be defined as a microsurgical non-microvascular flap.7
In the lower leg and ankle region, perforators of the main three arteries, anterior tibial artery (ATA), PTA, and peroneal artery, can be chosen according to the defect site. This might aid in the design of pedicled perforator flaps of the lower leg as the most clinically useful one in each case. Gir et al.1 systematically reviewed the pedicled-perforator flaps in the lower extremity defects and noted that the PAPF and the PTAPF were the most frequently used flaps. However, compared to the PAPF, PTAPF has rarely been reported in the literature until now. This is assumed to result from the fact that lateral aspect of lower leg is more frequently injured or ulcerated than the medial aspect, or that there is the bias of surgeon’s relative familiarity of fibular bone free flap. Because ATA perforators are clustered in the proximal rather than the distal segment of the lower leg, ATAPF has been rarely used in the lower leg and ankle reconstructions.8
Schaverien and Saint-Cyr9 analyzed the locations of the reliable perforators from the three main arteries in the lower leg and found that those of the PTA were distributed evenly compared to the other two arteries. PTA perforators are
A B C D
Fig. 3. Ankle defect with metal fixator exposure. (A) Ankle defect with exposure of the metal fixator. peroneal artery perforator flap had been performed previously. (B) Flap is elevated based on a perforator of the posterior tibial artery (arrow). (C) Immediate appearance after surgery. (D) Appearance of 6 months after surgery.
found to be the largest of the lower leg and easier to dissect compared to the PAP. They are predominantly septocutaneous, arising from within the intermuscular septum between soleus and flexor hallucis longus.10 Ozdemir et al.11 also performed comprehensive cadaver studies to conclude that distal lower leg is suitable for PTAPF elevation because PTA perforators are larger and concentrated in the lower leg and ankle region which they categorized zone I and II. Moreover, Jakubietz et al.12 recently described that the PTA perforator was most favorable as source vessel due to its constant subfascial directionality, which is almost always about 90~100 degrees. The PTA perforators are connected in an axial network and this enables the surgeon to raise large flaps reported up to 19×13 cm.5,13
In terms of location, the largest PTA perforators are clustered in the middle third, at 6 to 8 cm and 10 to 12 cm from the tip of the medial malleolus, and the flap can be reliably harvested within 10 cm of the popliteal crease.14 On this anatomical basis, propeller flap based on the perforators of the middle clusters has been widely studied and used clinically. However, conventional islanded-propeller type of flap leaves a long scar on the proximal lower leg and these results in rather unsatisfactory aesthetic outcome and the possibility of venous congestion followed by partial necrosis always exists. We also experienced partial flap necrosis after venous congestion in Case 3. This was assumed to be caused by suprafascial elevation design of the flap over the perforasome and kinking of the pedicle. Though it is unclear which factors matter most, this provides a lesson that if tendon, bone or hardware is exposed, it is important to include maximal amount of fascia in the proximal portion of the flap when elevating a conventional propeller flap. Therefore, the best method is covering the defect with very near tissue and this means focus should be changed to the distal perforators.
Fortunately, though the largest perforators are clustered in the middle third, septocutaneous form of perforators, which are relatively large and easy to dissect distally. They can be adequately used for coverage of complex defects of the heel, medial malleolus and Achilles tendon as in our cases. We simply searched suitable perforators very near the defect, which we described as “close-by” above.
Once a suitable perforator was found, the flap was designed again as Robotti et al.15 described as “on demand” considering the arc of rotation and location of the defect. If a proper perforator was not encountered, initial island flap scheme was
abandoned and alternative random pattern transposition flap could be attempted. This situational progressing provides a guarantee against risk though needs surgeon’s experience.
As Taylor and Palmer16 divided septocutaneous perforators of the lower leg into three groups of medial, anterolateral, posterolateral, most medially located defects can be effectively reconstructed by using PTAP. However, the position and caliber of perforators are highly variable between individuals and are often asymmetric even within the same individual. If ATAP or PAP is superior to the PTAP, medial defects can be covered using them, location permitting. Accordingly, preoperative imaging study such as high-resolution computed tomography angiography or magnetic resonance angiography should be preceded to exclude patients with anatomic variations and to establish a surgical plan.
PTAPF is an anatomically excellent option though it is occasionally overlooked due to its low frequency of use compared to the PAPF. Close-by islanded perforator flap form has many advantages for the small to moderate-sized defect of the medial malleolar region compared to the previous methods.
In addition to the advantages of the perforator flap such as minimal donor-site morbidity, preservation of the main vessel which supplies to the foot, excellent color, texture and thickness match, it is aesthetically appealing. Close-by islanded PTAPF does not just provide more choice alternatives but it also gives an ideal solution for the small to medium-sized complex defect of the ankle, especially in the medial malleolar region.
CONCLUSION
Posterior tibial artery perforator based propeller flaps is one of the most useful methods for repairing soft tissue defect or chronic wound in the medial malleolar area and in heel around ankle. It carries minimal donor site morbidity, and is a relatively simple surgical technique rather than a microsurgical free flap, and it conforms to replacement of tissue using “like-for-like”
principles.
REFERENCES
1. Gir P, Cheng A, Oni G, Mojallal A, Saint-Cyr M. Pedicled- perforator (propeller) flaps in lower extremity defects: a systematic review. J Reconstr Microsurg 2012;28:595-601.
2. Hyakusoku H, Yamamoto T, Fumiiri M. The propeller flap method. Br J Plast Surg 1991;44:53-4.
3. Taylor GI. The angiosomes of the body and their supply to perforator flaps. Clin Plast Surg 2003;30:331-42.
4. Venkataramakrishnan V, Mohan D, Villafane O. Perforator based V-Y advancement flaps in the leg. Br J Plast Surg 1998;51:
431-5.
5. Koshima I, Moriguchi T, Ohta S, Hamanaka T, Inoue T, Ikeda A. The vasculature and clinical application of the posterior tibial perforator-based flap. Plast Reconstr Surg 1992;90:643-9.
6. Lees V, Townsend PL. Use of a pedicled fascial flap based on septocutaneous perforators of the posterior tibial artery for repair of distal lower limb defects. Br J Plast Surg 1992;45:141-5.
7. Georgescu AV, Matei I, Ardelean F, Capota I. Microsurgical nonmicrovascular flaps in forearm and hand reconstruction.
Microsurgery 2007;27:384-94.
8. Panagiotopoulos K, Soucacos PN, Korres DS, Petrocheilou G, Kalogeropoulos A, Panagiotopoulos E, et al. Anatomical study and colour Doppler assessment of the skin perforators of the anterior tibial artery and possible clinical applications. J Plast Reconstr Aesthet Surg 2009;62:1524-9.
9. Schaverien M, Saint-Cyr M. Perforators of the lower leg: analysis of perforator locations and clinical application for pedicled perforator flaps. Plast Reconstr Surg 2008;122:161-70.
10. Whetzel TP, Barnard MA, Stokes RB. Arterial fasciocutaneous
vascular territories of the lower leg. Plast Reconstr Surg 1997;
100:1172-83.
11. Ozdemir R, Kocer U, Sahin B, Oruc M, Kilinc H, Tekdemir I.
Examination of the skin perforators of the posterior tibial artery on the leg and the ankle region and their clinical use. Plast Reconstr Surg 2006;117:1619-30.
12. Jakubietz RG, Schmidt K, Zahn RK, Waschke J, Zeplin PH, Meffert RH, et al. Subfascial directionality of perforators of the distal lower extremity: an anatomic study regarding selection of perforators for 180-degree propeller flaps. Ann Plast Surg 2012;69:307-11.
13. Heymans O, Verhelle N, Peters S. The medial adiposofascial flap of the leg: anatomical basis and clinical applications. Plast Reconstr Surg 2005;115:793-801.
14. Schaverien MV, Hamilton SA, Fairburn N, Rao P, Quaba AA.
Lower limb reconstruction using the islanded posterior tibial artery perforator flap. Plast Reconstr Surg 2010;125:1735-43.
15. Robotti E, Carminati M, Bonfirraro PP, Bocchiotti MA, Ortelli L, Devalle L, et al. "On demand" posterior tibial artery perforator flaps: a versatile surgical procedure for reconstruction of soft tissue defects of the leg after tumor excision. Ann Plast Surg 2010;64:202-9.
16. Taylor GI, Palmer JH. The vascular territories (angiosomes) of the body: experimental study and clinical applications. Br J Plast Surg 1987;40:113-41.