| Abstract |
Purpose: The purpose of this study was to demonstrate the effects of proprioceptive neuromuscular facilitation (PNF) stability techniques on walking speed, trunk stability, and balance in stroke patients.
Methods: Ten stroke patients volunteered to participate in the study, and each of subjects was randomly assigned to either the stability technique (ST) group (n=5) or to the treadmill (TM) group (n=5). Each therapeutic exercise program was provided for 30 minutes a day, 5 days per week for 4 weeks. The ST group performed a PNF pattern combined with stabilizing reversal and rhythmic stabilization of the PNF stability technique. Walking speed (measured using a 10-meter walking test), trunk stability (TIS), and balance (BBS, FRT) were evaluated before and after training. All data were analyzed using SPSS version 18.0. The significance level for statistical inspection was set at 0.05.
Results: Both groups showed improvements on the 10-meter walking test, the trunk impairment scale, the Berg balance scale, and the functional reaching test.
Conclusion: PNF stability techniques are effective for improving trunk stability, balance, and walking speed in stroke patients.
For stroke patients, PNF stability techniques are very useful and effective, including in clinical practice.
Key Words: Stabilizing reversal, Rhythmic stabilization, Splinter skate pattern, Stroke, Treadmill, Walking speed, Balance
†Corresponding Author : Gwan-Cheol Maeng ([email protected])
Original Article Open Access
PNF의 안정적 반전과 율동적 안정화 기법이 뇌졸중 환자의 보행 및 균형에 미치는 영향
김진인⋅강혜원
1⋅지민
2⋅황상수
3⋅맹관철
4†1)안산조은재활요양병원,
1순천향대학교부천병원,
2인천백병원,
3예은병원,
4미추홀재활전문병원
The Effect of Stabilizing Reversal and Rhythmic Stabilization in PNF on Walking and Balance in Patients with Stroke
Jin-In Kim⋅Hye-Won Kang
1⋅Min Ji
2⋅Sang-Su Hwang
3⋅Gwan-Cheol Maeng
4†Dept. of Physical Therapy, Ansan joun Hospital
1
Dept. of Physical Therapy, Soonchunhyang University Bucheon Hospiatal
2
Dept. of Physical Therapy, Incheon Baek Hospital
3
Dept. of Physical Therapy, Yeeun Hospital
4
Dept. of Physical Therapy, Michuhall Hospital
Received: March 21, 2018 / Revised: August 9, 2018 / Accepted: August 9, 2018
ⓒ 2018 Journal of Korea Proprioceptive Neuromuscular Facilitation Association
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License
(http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction
in any medium, provided the original work is properly cited.
Ⅰ. 서 론
인간 수명의 증가와 뇌졸중 발생율의 증가로 재활 서비스에 대한 수요가 증가되고 뇌졸중 관련 장애의 치료와 관련된 의료 자원 효율성의 최적화는 점점 더 우선순위로 간주된다(Balaban et al., 2011). 뇌졸중은 뇌에 혈액공급 방해를 받아 뇌 기능을 빠르게 잃어버 리는 것으로 막힘 (혈전 또는 동맥 색전)으로 인한 허혈 (뇌혈류 부족) 또는 출혈 때문이다(Chung & Lee, 2013).
뇌졸중은 여러 나라에서 성인장애를 일으키는 첫 번 째이며 사망의 원인도 암과 심장질환 다음 순서이다 (Sims et al., 2010). 뇌졸중 환자는 운동장애, 인지 및 지각장애, 언어장애 등으로 인해 일상생활동작에서 많은 장애를 동반할 수 있다 (Gowland et al., 1992). 편마 비로 인한 운동장애는 균형반응 장애, 비대칭적 자세, 보행능력의 저하, 섬세한 기능을 수행하는 운동능력 상실 등과 같은 문제점을 보이게 된다 (Carr et al., 1985).
이러한 문제점은 환자의 독립적인 일상생활에 제한을 가져오게 되고 낙상과 같은 이차적인 손상을 초래하 기도 한다(Perry & Jon, 1992).
뇌졸중 환자의 약 30%는 영구적인 장애를 갖게 되 며 약 75%는 보행 능력이 저하 된다(Jorgensen et al., 1995). 이에 뇌졸중 환자의 재활 과정에서 보행 능력의 향상은 환자의 독립성과 직결되는 중요한 요소이며 (Taylor et al., 2012), 기능적 독립성을 이루는데 가장 중요한 항목으로 치료의 중요한 목표가 된다(Turnbull et al., 1995). 보행 속도는 건강한 성인과 뇌졸중 환자의 기능장애를 분별하는 지표로써(Taylor et al., 2012), 뇌 졸중 환자들은 느린 보행속도와 낮은 지구력으로 인해 독립적 이동이 어렵게 되며(Hill et al., 1997) 느린 보행속도는 기능적 독립수준과 삶의 질에 부정 적인 역할을 주게 되어 보행속도의 개선은 안전하게 집과 지역사회에서 활동하기 위한 필수 요소이다 (Dickstein, 2008).
보행은 일반적으로 균형능력 협응능력 운동감각 고유수용감각 관절 및 근육의 통합적 작용으로 나타 나며 보행의 안정성을 확보하기 위하여 시각, 운동감
각 , 촉각, 전정감각은 서로 자동적인 보행 패턴 전략을 가지고 조절 된다. 균형 조절 기능은 신체 이동 시 중력에 대항하여 무게 중심을 조절하고 보행 시 보폭 이나 보행을 안정적으로 유지함으로써 다양한 자세를 취하게 하는 자동운동 조절 능력이라 할 수 있다 (Berg et al., 1992). 뇌졸중 환자는 몸통의 근력과 고유수용성 감각 등의 결손으로 인하여 몸통을 조절하는 능력이 감소하게 되어 보행과 균형능력에 영향을 미치게 된 다(Ryerson et al., 2008). 뇌졸중 환자에서 보행능력과 동적 균형 능력은 일상생활동작과 상관관계가 상당히 높으며(Langhammer et al., 2006), 뇌졸중 환자에게서 균형조절은 일상생활에서 가장 필요하며 보행에 있어 기본적인 기술이다.
체간은 자세 반응과 조절에서 신체의 중심 역활을 하며 다양한 일상생활 활동을 위해서는 균형을 유지 하기 위한 체간 조절 능력이 필요하다(Dean &
Shepherd, 1997). 체간의 적절한 안정화 없이는 상, 하 지 근육의 수축이 체간에 영향을 미쳐 척추구조와 연 부조직에 과도한 부하가 발생되는 움직임을 야기하며 이로 인해 자세조절, 균형 및 보행에 장애가 유발될 수 있다 (Song & Kim, 2010). 체간조절 능력을 기르는 것이 보행을 개선시키기 위한 중요한 인자가 될 수 있을 것이다(Chung et al., 2012).
이러한 보고들을 바탕으로 고전적 물리치료 방법 뿐만 아니라 트레드밀 훈련(Polese et al., 2013), 측방보 행훈련(Kim et al., 2013), 보행적응 훈련(Timmermans et al., 2016) 등의 다양한 치료가 행해지고 있다. 이러한 다양한 치료 중 기능적 활동 능력을 향상시키기 위해 적절한 치료법이 필요하며 이를 위해서는 운동성 및 근력 지구력을 높이는 치료 프로그램이 강조되고 있 다(Lord et al., 2004).
PNF는 1940년 이후로 물리치료 분야에서 많이 알
려진 치료법 중 하나이다. Kabat 박사와 Margaret
(Maggi) Knott는 치료적 기법과 절차를 지속적으로 개
발하고 확장하기 시작하였다 . 오늘날 신경학적 환자,
외상환자 뿐만 아니라, 근골격계 증상을 가진 환자들
도 이 치료 개념으로 치료를 받고 있다(Adler et al.,
2013). PNF에는 기능적 활동 능력을 향상시키기 위해 여러 가지 기법들이 있으며 안정성과 균형 향상을 위 하여 안정적 반전과 율동적 안정화 기법을 많이 사용 하고 있다. Dietz (2009)는 보행주기 중 일어나는 운동 패턴과 동작을 PNF 개별 패턴과 통합하여 보행을 분 석하고 치료하는 것을 소개하였는데 이것을 달리는 사람(sprinter)과 스케이트 타는 사람(skater)의 동작으 로 분석하고 치료하였다 . 이는 몸통의 안정성을 전제 로 하고, 직립 보행을 묘사한다.
이러한 이유로 본 연구에서는 뇌졸중 환자들의 보 행과 균형 능력 향상을 위해 임상에서 흔히 사용되고 있는 treadmill을 이용한 트레드밀 훈련과(Oujamaa et al., 2009) 균형능력을 증진시키기 위한 PNF의 안정적 반전과 율동적 안정화 기법을 직립 보행을 묘사한 스 프린터, 스케이터 패턴에 적용하여 뇌졸중 환자를 치 료하였을 때를 비교하여 어느 치료 방법이 뇌졸중 환 자의 보행과 균형 능력을 향상시키는데 보다 더 효과 적인 방법인지를 확인하고자 한다.
Ⅱ. 연구 방법
1. 연구 대상
본 연구의 대상자는 인천광역시 B구 소재의 G 병원 에 입원하고 있는 환자를 대상으로 실시하였다 . 대상 자는 뇌졸중으로 인한 편마비를 진단받고 독립적으로
10m 보행이 가능하며, 연구자가 지시하는 내용을 이 해하고 따를 수 있도록 한국판 간이 정신상태 검사 (mini mental state examination-Korea, MMSE-K) 점수가 24점 이상인 자로 본 연구에 대한 목적과 절차의 설명 을 충분히 숙지하고 동의서를 받은 10명을 대상으로 하였다. 이들은 각각 PNF 안정성 기법을 적용한 실험 군(n=5)과 트레드밀 훈련을 실시한 대조군(n=5)으로 배정하였다. 연구대상자의 신체적 특징을 Table 1과 같다.
2. 측정 방법 및 도구
1) 10미터 걷기 검사(10 meter walking test, 10MWT)
본 연구에서는 보행 능력을 측정하기 위해 10m 걷 기 검사를 실시하였다. 10MWT는 보행 능력를 알아보 기 위한 측정도구로서 10M를 걷게 한 후 소요된 시간 을 측정하는 것이다. 바닥에 줄자를 이용하여 총 14M 거리를 설정하여 시작 지점과 끝 지점에 테이프를 이 용하여 표식을 하고 시작 지점과 끝 지점으로부터 각 각 2M 지점에 표식을 하여 그 구간을 걷게 한 후 중간 의 10M 지점을 경과한 시간을 초시계를 이용하여 측 정하였다 . 이 측정의 측정자 내 신뢰도는 r=0.95, 측정 자 간 신뢰도는 r=0.90으로 나타났다(Mehrholz et al., 2007).
ST group (n=5) TM group (n=5)
Sex Male 4 2
Female 1 3
Age (yrs) 59.8±9.81 56.6±11.48
Height (cm) 169.40±6.66 168.20±8.81
Weight (kg) 71.20±11.97 68.20±4.76
On set duration (month) 40.60±26.81 55.60±21.82
Values=means±SD
ST: stability technique, TM: treadmill
Table 1. General characteristics of study subjects (n=10)
2) 버그균형척도 검사(Berg balance scale, BBS)
BBS 검사는 뇌졸중환자의 낙상 위험도 및 동적 균 형을 측정하기 위하여 사용되는 임상측정 방법이다.
본 측정은 총 14개의 항목으로 구성되어 있으며 자세 변화, 서기, 앉기의 3개의 하위영역으로 구분되어 0점 에서 4점까지 총 14개 항목에 대한 56점 만점으로 구성 된다. BBS 검사는 뇌졸중 환자에서 측정자 내 신뢰도 가 r=0.97이고 검사-재검사 신뢰도가 r=0.98에 해당하 는 매우 높은 신뢰도가 보고된 측정방법이다(Blum et al., 2008).
3) 기능적 팔뻗기 검사(functional reach test, FRT)
길이가 표시된 쇠자를 어깨 높이로 벽에 고정한 후 대상자가 측면으로 어깨관절의 어깨뼈 봉우리가 벽에 거의 닿도록 하였다. 어깨 관절은 90로 굴곡하고, 팔굽 관절은 완전히 신전한 후 손은 편 상태로 벽에 닿지 않도록 하였다. 대상자는 손을 평행하게 앞으로 뻗었을 때 세 번째 손 허리뼈의 끝을 측정하여 시작점 을 표시하였다. 대상자가 측정도구와 수평으로 가능 한 한 전방으로 뻗치도록 지시한 후 10초간 유지할 수 있는 지점에 표시하였다 . 대상자들이 발을 움직이 면 측정을 다시 하였다 총 대상자들에게 한 번의 연습 시도가 주어졌고 본 측정을 시행하였다 . 각 측정 사이 는 근육의 피로 유발을 방지하기 위하여 1분 동안 휴식 을 취하게 하였다(Duncan et al., 1990).
4) 체간 장애 척도(trunk impairment scale, TIS)
TIS는 뇌졸중 환자의 체간 움직임의 질을 관찰할 수 있다. 안정적인 앉은 자세 균형, 동적인 앉은 자세 균형, 체간조화로 측정을 하게 된다. 최대 점수는 안정 적 & 동적인 앉은 자세 균형과 체간조화의 각 점수는 7, 10, 6점이다. TIS는 최소 0점에서 최대 23점이며 점수가 높을 수록 체간 수행력이 좋은 것을 의미한다.
TIS는 측정자 간 신뢰도는 r=0.99 검사-재검사 신뢰도
가 r=0.96로 나타났다(Verheyden et al., 2010).
3. 실험 방법
1) 트레드밀 훈련 운동군
임상에서는 뇌졸중 환자들의 보행과 균형 능력 향 상을 위해 일반적인 트레드밀 훈련 방법이 주로 사용 되고 있다 (Oujamaa et al., 2009). 본 연구에서는 트레드 밀 보행훈련을 위하여 경사 트레드밀(Treksta, Jaeilfitness, Korea)을 사용하였다. 이 트레드밀은 0.1km/hour의 최저속도로부터 시작할 수 있게 되어 있다. 트레드밀은 환자가 편안하게 할 수 있는 속도로 보행운동을 하루 30분 주 5회, 4주간 실시하였다. 이때 보조하는 물리치료사 1명을 위치하여 안정감 있고 편 안한 상태에서 트레드밀을 탈 수 있도록 유도하였다 . 2) 고유수용성신경근촉진법 안정성 기법 운동군
중재기간 동안 실험군에게 준비운동으로 splinter
pattern을 10분간 실시하고 운동 프로그램은 sitting,
half standing에서 상하지 협응적 패턴자세를 취한 후
안정적 반전과 율동적 안정화 치료기법을 적용하였으
며 마무리 운동으로 splinter pattern을 10분간 실시하여
하루 30분 주 5회, 4주간 실시하였다. 협응적 패턴 자세
는 Dietz (2009)에 의해 소개되었던 스프린터(sprinter)
패턴으로 한쪽편 상지는 scapular anterior elevation,
shoulder flexion adduction external rotation, elbow flexion
supination를 하지는 pelvic posterior depression, knee
extension 자세를 취하고 반대측 상지는 scapular
posterior depression, shoulder extension abduction
internal rotation, elbow extension pronation를 하지는
pelvic anterior elevation, knee flexion 자세를 취하여
양쪽 교대적으로 수행하였다. 안정적 반전은 치료사
가 자신의 한손을 주동근과 반대손을 길항근에 교대
로 접촉하여 지속적으로 근육이 활성화 되도록 실시
하고 율동적 안정화는 양손을 주동근과 길항근이 동
시에 활성화 되도록 실시하였다. 자세한 운동방법은 Table 2에 제시 하였다.
4. 자료 처리
측정된 데이터는 SPSS 18.0 version (SPSS, Chicago, IL, USA) 프로그램을 사용하여 평균(M)과 표준편차 (SD)로 나타내었다. Shapiro-wilk로 정규성 검정을 하 였고 트레드밀 운동군과 PNF 안정성 기법 운동군의 중재 전 후의 집단 내 변화를 비교하기 위하여 Paired t-test, 집단 간 변화를 비교하기 위하여 independent t-test를 실시하였으며 모든 통계학적 유의수준은 α
=0.05로 설정하였다.
Ⅲ. 연구 결과
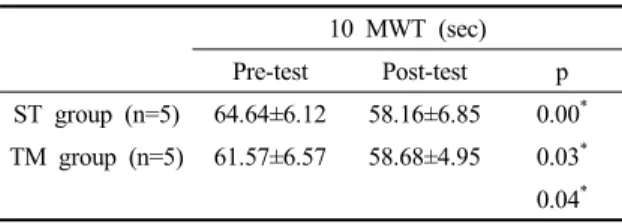
1. Change of 10meter walking test between ST group and TM group
10m 걷기 검사에서 ST 그룹은 중재 전 64.64±
6.12(sec)에서 중재 후 58.16±6.85(sec)로 유의한 감소 를 보였으며, TM 그룹에서도 중재 전 61.57±6.57(sec) 에서 중재 후 58.68±4.95(sec)로 유의한 감소를 보였다.
Program Repeated / set Time
Warm up Sprinter pattern 10min
Eexercise program
Position Pattern Technique
Sitting Sprinter SR, RS 10 repeated (2set) 5min
Half standing Sprinter SR, RS 10 repeated (2set) 5min
Cool down Sprinter pattern 10min
SR: stabilizing reversal, RS : rhythmic stabilization Table 2. Exercise program
Fig. 1. Splinter pattern in sitting position. Fig. 2. Splinter pattern combine with stability techniques.
그리고 훈련방법에 따른 그룹 간 차이 비교에서 ST 그룹은 TM 그룹과 유의한 차이가 있었다(Table 3).
2. Change of Berg balance scale between ST group and TM group
BBS 검사에서 ST 그룹은 중재 전 31.80±4.32(score) 에서 중재 후 33.80±3.96(score)로 유의한 차이를 보이 지 않았으며, TM 그룹에서도 중재 전 35.40±
4.45(score)에서 중재 후 35.20±3.63(score)으로 유의한 차이를 보이지 않았다. 그리고 훈련방법에 따른 그룹 간 차이 비교에서 ST 그룹은 TM 그룹과 유의한 차이 가 없었다(Table 4).
3. Change of functional reach test between ST group and TM group
FRT 검사에서 ST 그룹은 중재 전 17.82±2.41(cm)에 서 중재 후 19.88±2.21(cm)으로 유의한 증가를 보였으 며, TM 그룹에서는 중재 전 17.46±2.58(cm)에서 중재 후 17.62±1.85(cm)로 유의한 차이를 보이지 않았다.
그리고 훈련방법에 따른 그룹 간 차이 비교에서 ST 그룹은 TM 그룹과 유의한 차이가 있었다(Table 5).
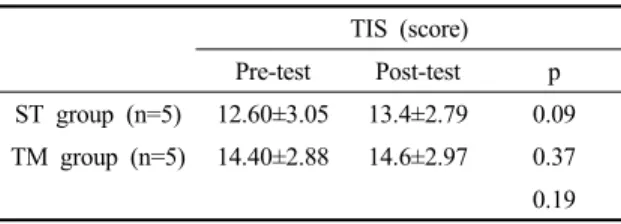
4. Change of trunk impairment scale between ST group and TM group
TIS 검사에서 ST 그룹은 중재 전 12.60±3.05(score) 에서 중재 후 13.4±2.79(score)로 유의한 차이를 보이지
10 MWT (sec)Pre-test Post-test p ST group (n=5) 64.64±6.12 58.16±6.85 0.00* TM group (n=5) 61.57±6.57 58.68±4.95 0.03* 0.04* Values=mean±SD
*p<0.05
10MWT: 10 meters walking test
Table 3. Change of 10MWT between ST group and TM group
BBS (score) Pre-test Post-test p ST group (n=5) 31.80±4.32 33.80±3.96 0.08 TM group (n=5) 35.40±4.45 35.20±3.63 0.74 0.25 Values=mean±SD
*p<0.05
BBS: Berg balance scale
Table 4. Change of BBS between ST group and TM group
Fig. 3. Result of 10meter walking test between ST group and TM group.
Fig. 4. Result of Berg balance scale between ST group and TM group.
않았으며, TM 그룹에서도 중재 전 14.40±2.88(score)에 서 중재 후 14.6±2.97(score)로 유의한 차이를 보이지 않았다 . 그리고 훈련방법에 따른 그룹 간 차이 비교에 서 ST 그룹은 TM 그룹과 유의한 차이가 없었다(Table 6).
Ⅳ. 고 찰
뇌졸중으로 인한 편마비 환자는 비정상적인 근긴 장도, 불안정한 균형, 근력 약화 등으로 인해 비대칭적 자세 보행능력 저하와 같은 운동능력의 상실을 가져 온다(Sharp et al., 1997). 이 중 근력약화는 편마비 환자 의 기능적 재활을 어렵게 하며(Bohannon & Richard, 1995) 특히 약화되는 근육 중 신체의 중심인 체간에 위치한 체간 근육은 일상생활 중 다양한 자세유지에
필수적으로 이 근육들의 적절한 근력과 지구력은 매 우 중요하다 (Handa et al., 2000). 체간 근육에 의해 결정 되는 체간 안정성은 팔, 다리의 움직임 동안 발생된 불안정에 대해 체간을 준비시켜 특정한 목적에 맞는 운동을 할 수 있도록 체간을 적응시키는 것이다 (Dickstein et al., 2004). 하지만 뇌졸중 환자들은 정상인 에 비해 체간의 안정성이 감소되어 있으며 이러한 체 간 안정성의 감소는 뇌졸중 환자의 균형과 전반적인 보행양상의 변화를 가져오게 된다(Tsuji et al., 2003).
PNF에서 제시한 각 분절 패턴을 통합하여 사지 간 협응 체계로 정형화 한 것이 스프린터 , 스케이터인데 이 동작은 몸통패턴 , 상지패턴, 하지 패턴, 머리와 목 패턴을 포함하고 있는 다면적 복합운동 프로그램이다 (Kim & Kim, 2013). 이러한 스프린터, 스케이터는 가장 효율적이고 기능적인 동작을 가장 잘 표현한 것이며 ,
FRT (cm)Pre-test Post-test p ST group (n=5) 17.82±2.41 19.88±2.21 0.00* TM group (n=5) 17.46±2.58 17.62±1.85 0.69 0.00* Values=mMean±SD
*p<0.05
FRT: functional reaching test
Table 5. Change of FRT between ST group and TM group
TIS (score) Pre-test Post-test p ST group (n=5) 12.60±3.05 13.4±2.79 0.09 TM group (n=5) 14.40±2.88 14.6±2.97 0.37 0.19 Values=mean±SD
*p<0.05
TIS: trunk impairment scale
Table 6. Change of TIS between ST group and TM group
Fig. 5. Result of functional reach test between ST group and TM group.
Fig. 6. Result of trunk impairment scale between ST group and TM group.