Osteochondritis dissecans (OCD) is a condition described in 1870 by König as an idiopathic focal lesion affecting the subchon
dral bone with possible compromise of the stability of the adja
cent cartilage. The condition can cause arthrosis at a young age1). The spectrum of lesions is broad and ranges from the superficial compromise of the cartilage to osteochondral collapse and the formation of intraarticular loose bodies2).
There has yet to be a consensus about the aetiology, and it has been associated with avascular necrosis of the subchondral bone, genetic causes, abnormal calcification patterns, and endocrine abnormalities2). Genetic studies have associated specific altera
tions with OCD, such as the ACAN gene; however, a pattern has
not yet been identified3).
The most commonly affected joint is the knee, specifically the medial femoral condyle. OCD mainly affects men (2:1 compared to women) in the adolescent stage between the second and third decades4). The most frequent clinical presentation is knee pain of increasing intensity during daily and sports activities that may be accompanied by a sensation of locking knee2,5).
Many classifications for OCD has been proposed. According to the review performed by Jacobs et al.1) the first classification proposed for OCD was the one proposed by Guhl y cols in 1979.
This classification consisted of 4 stages: grade 1, lesion is present yet intact; grade 2, superficial fissure of the cartilage; grade 3, par
tial detachment of the cartilage; and grade 4, complete detach
ment of the cartilage, loose bodies and the presence of a crater in the subchondral bone. Classification systems have been modified and adapted for magnetic resonance imaging (MRI)1). The treat
ment of grade 4 OCD lesions depends on the size, cartilage sta
bility, and the physeal status6).
This case report aims to present a novel technique to treat grade 4 OCD with good functional outcomes at oneyear followup.
Treatment of Osteochondritis Dissecans of the Knee with Autologous Iliac Bone Graft and Hyaluronic Acid Scaffold
Jaime Hinzpeter, MD
1, Alvaro Zamorano, MD
1, Maximiliano Barahona, MD
1, and Pablo Campos, MD
21Department of Orthopaedic Surgery, Clinical Hospital University of Chile, Santiago; 2Department of Orthopaedic Surgery, Hospital of Talca, Talca, Chile
Osteochondritis dissecans (OCD) is a condition that corresponds to an idiopathic focal lesion affecting the subchondral bone with possible compromise of the stability of the adjacent cartilage. Treatment depends on the size of the lesion, cartilage stability, and the physeal status. The case reported is about an 18yearold male patient who complained of suffering from knee pain for a period of ten months. Magnetic resonance imaging (MRI) revealed a lesion of 2 cm2 in the medial femoral condyle that compromised the subchondral bone, compatible with OCD. He underwent surgery that consisted of filling the subchonral defect with an iliac crest autograft and sealing the defect with a hyaluronic acid scaffold. At the 12month followup, the MRI shows complete healing and the patient has resumed sports activities. Management with autologous iliac crest graft and hyaluronic acid scaffold represents an effective alternative treatment for OCD.
Keywords: Knee, Osteochondritis dissecans, Bone graft, Hyaluronic acid, Tissue scaffold
Case Report
Knee Surg Relat Res 2019;31(2):143-146 https://doi.org/10.5792/ksrr.18.053 pISSN 2234-0726 · eISSN 2234-2451
Knee Surgery & Related Research
Received August 29, 2018; Revised (1st) October 30, 2018;
(2nd) November 27, 2018; (3rd) January 2, 2019; Accepted January 7, 2019 Correspondence to: Jaime Hinzpeter, MD
Department of Orthopaedic, Clinical Hospital University of Chile, Santos Dumont 999 Independencia, Santiago 8380000, Chile Tel: +56229788000, Fax: +56229788225
Email: [email protected]
143
This is an Open Access article distributed under the terms of the Creative Commons Attribution NonCommercial License (http://creativecommons.org/licenses/bync/4.0/) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright © 2019 KOREAN KNEE SOCIETY www.jksrr.org
144
Hinzpeter et al. OCD Treatment with Autogenous Iliac Bone Graft and Hyaluronic Acid ScaffoldCase Report
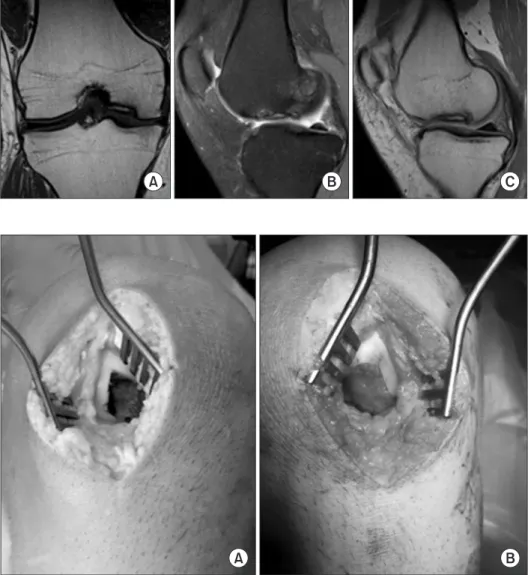
An 18yearold patient with no prior trauma history sought a medical consultation after suffering knee pain for ten months. A physical examination revealed medial knee pain, joint effusion, and a full knee range of motion. An MRI was requested, which revealed a lesion in the medial condyle compatible with grade 4 OCD (Fig. 1). The patientreported outcome before surgery was level 2 on the Tegner scale and 36 points on the Lysholm scale.
The patient underwent surgery under spinal anesthesia and sedation. First, diagnostic arthroscopy was conducted by an an
terolateral portal and an anteromedial portal and no other lesions were found. The defect in the medial condyle was confirmed and measured 2 cm in length and 1 cm in width.
Then, the contralateral anterior iliac crest (AIC) was addressed by an open approach performed parallel to the AIC. The ante
riorsuperior iliac spine was identified, and the harvest was per
formed 2 cm posterior to avoid an injury to the lateral femoral cutaneous nerve. Bone harvesting was performed with the trap
door technique as described by Cooper and Coughlin7).
Finally, a medial parapatellar arthrotomy was performed to expose the medial condyle. The knee was flexed and the patella was gently pulled laterally by a retractor to obtain full exposure.
Curettage of the lesion was performed with removal of all the de
vitalized tissue under the cartilage defect until healthy tissue was visualized, and then the 1cm deep defect was noted (Fig. 2). The defect was filled with the cancellous bone graft obtained from the AIC up to the level of the adjacent subchondral bone; then it was sealed with Hyalofast® (Cimed Healthcare, Kuala Lumpur, Ma
laysia) biodegradable hyaluronic acid scaffold. This scaffold was sutured with four stitches of 20 Ethibond® (Ethicon, Somerville, NJ, USA). Full range of motion and no weight bearing were en
couraged for six weeks after hospital discharge.
At oneyear followup, the patient was asymptomatic without
Fig. 1. Magnetic resonance imaging show
ing a grade 4 osteochondritis in the femoral condyle. (A) Coronal T1 sequence showing the defect in the femoral condyle; the size was 1 cm. (B) Sagittal T2 sequence showing the defect in the medial femoral condyle and mild edema in the surrounding area.
(C) Sagittal T2 sequence showing the defect in the medial femoral condyle; the size was 2 cm.
Fig. 2. Intraoperative photograph. (A) Only healthy tissue was left after curettage. (B) The lesion was filled with the iliac crest au
tograft and sealed with Hyalofast® (Cimed Healthcare) biodegradable hyaluronic acid scaffold.
Knee Surg Relat Res, Vol. 31, No. 2, Jun. 2019
145
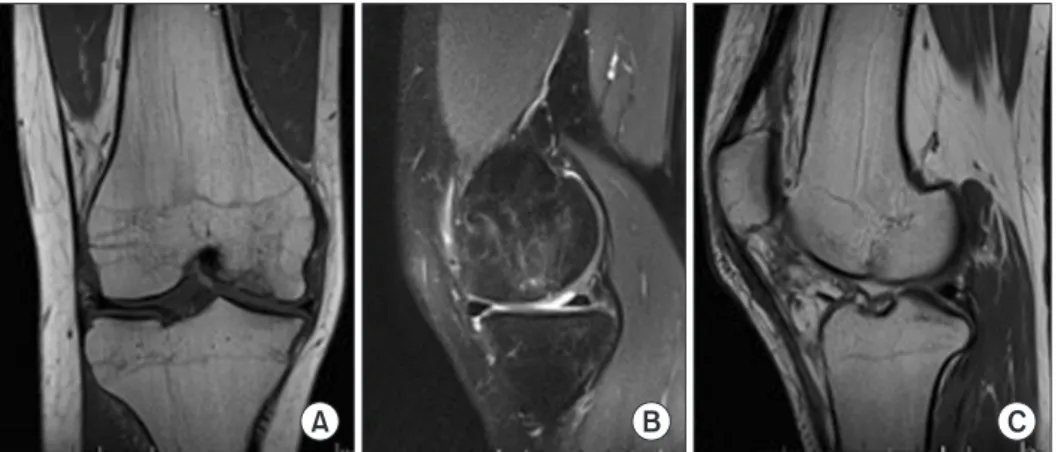
joint pain and had a full range of motion. An MRI was per
formed, which showed complete healing of the subcondral bone and a continuous signal of the cartilage in the medial femoral condyle (Fig. 3). The patient was authorized to resume sports.
Patientreported outcomes at oneyear followup were level 4 on the Tegner scale and 90 points on the Lysholm scale.
Discussion
OCD is a disabling pathology in adolescent athletes, represent
ing an important challenge for the knee surgeon, especially in grade 4 lesions8). Standard treatment for grade 4 OCD is to per
form an osteochondral autologous transfer (OATS), which con
sists of obtaining an osteochondral cylinder from a knee region with low contact pressure, most commonly, the lateral trochlea, and to transfer it to the site of the defect9). This procedure has the disadvantage of leaving a defect in another area of the knee; nev
ertheless, reports show a favorable outcome in 82% of patients10). In our case, the size of the lesion was so large that it was at the upper size limit of the traditional OATS indication; two 10 mm plugs would have to be used for OATS in the patient, which means a large donor area in the trochlea11,12). Taking this into ac
count, it was decided to use an iliac crest autograft to fill the de
fect and seal it with a biodegradable hyaluronic acid membrane.
With this, a structural and biological environment for fibrocar
tilage formation was provided. A disadvantage of this technique is the risk of iliac crest pain and paresthesia of the lateral femoral cutaneous nerve; nevertheless, the patient had no complaints af
ter the first postoperative month.
The size of the lesion is critical in the treatment decision mak
ing of OCD2). For a large lesion, several techniques are described.
Hohmann and Tetsworth13) described in patients with OCD over 2.5 cm2, the use of a freshfrozen irradiated allograft provided good results; nevertheless, this type of graft is expensive and
unavailable worldwide. Zellner et al.14) reported good outcomes were achieved with use of bone autograft from either the iliac crest or the distal femur, combined with autologous chondrocyte transplantation in large and deep osteochondral defects; however, this also raises costs and is not widely available.
Development of cellfree scaffolds (chondrocytes) has arisen with the purpose of inducing tissue regeneration through the proliferation and migration of mesenchyme cells15). Also, scaf
folds would be able to sustain the clot created after microfractures or nanofractures and increase the success rate in medial condyle lesions16). Focusing on patients with OCD, Berruto et al.15) re
ported a multicenter study with 2 years of followup where good functional outcomes were achieved in large OCD lesions treated with scaffolds without chondrocytes.
The result of the treatment we proposed in this report is com
parable to the good results obtained with other types of treat
ment10,13,14,17,18). It also has the advantage of not requiring an intraarticular donor site and allografts in cases with deep and large defects greater than 2 cm2. Besides, the hyaluronic acid scaf
fold, despite the high cost, is more affordable than autologous chondrocyte transplants and freshfrozen allografts. Significant clinical and functional improvements were observed in this case, considering that the treated lesion was large, 2 cm2 in size and 1 cm in depth.
In conclusion, treatment of large (2 cm2) and deep grade 4 OCD lesions with autologous iliac crest bone grafts and hyaluronic acid scaffolds seems to be a good alternative for this challenging condition. Further studies must be conducted with longer follow
ups.
Conflict of Interest
No potential conflict of interest relevant to this article was re
ported.
Fig. 3. Magnetic resonance imaging at 12month followup. (A) Coronal T1 sequence showing adequate filling of the defect, with the healing of the subchondral bone. (B) Sagittal T2 showing continuous signal in the cartilage of the medial femoral condyle. (C) Sagittal T2 sequence showing adequate filling of the defect, with the heal
ing of the subchondral bone.
146
Hinzpeter et al. OCD Treatment with Autogenous Iliac Bone Graft and Hyaluronic Acid ScaffoldReferences
1. Jacobs JC Jr, ArchibaldSeiffer N, Grimm NL, Carey JL, Shea KG. A review of arthroscopic classification systems for os
teochondritis dissecans of the knee. Clin Sports Med. 2014;
33:18997.
2. Abouassaly M, Peterson D, Salci L, Farrokhyar F, D’Souza J, Bhandari M, Ayeni OR. Surgical management of osteochon
dritis dissecans of the knee in the paediatric population: a systematic review addressing surgical techniques. Knee Surg Sports Traumatol Arthrosc. 2014;22:121624.
3. Bates JT, Jacobs JC Jr, Shea KG, Oxford JT. Emerging genetic basis of osteochondritis dissecans. Clin Sports Med. 2014;
33:199220.
4. Grimm NL, Weiss JM, Kessler JI, Aoki SK. Osteochondritis dissecans of the knee: pathoanatomy, epidemiology, and di
agnosis. Clin Sports Med. 2014;33:1818.
5. Brittberg M, Winalski CS. Evaluation of cartilage injuries and repair. J Bone Joint Surg Am. 2003;85A Suppl 2:5869.
6. Carey JL, Grimm NL. Treatment algorithm for osteochon
dritis dissecans of the knee. Clin Sports Med. 2014;33:375
82.
7. Cooper MT, Coughlin MJ. Surgical technique: iliac crest corticocancellous bone graft harvest using a trapdoor tech
nique. Med Chir Pied. 2009;25:12732.
8. Heyworth BE, Kocher MS. Osteochondritis dissecans of the knee. JBJS Rev. 2015;3. pii: 0187447420150307000003.
9. Dhollander AA, Liekens K, Almqvist KF, Verdonk R, Lam
brecht S, Elewaut D, Verbruggen G, Verdonk PC. A pilot study of the use of an osteochondral scaffold plug for car
tilage repair in the knee and how to deal with early clinical failures. Arthroscopy. 2012;28:22533.
10. Lim HC, Bae JH, Song SH, Park YE, Kim SJ. Current treat
ments of isolated articular cartilage lesions of the knee achieve similar outcomes. Clin Orthop Relat Res. 2012;470:
22617.
11. Mithoefer K, Williams RJ 3rd, Warren RF, Wickiewicz TL, Marx RG. Highimpact athletics after knee articular carti
lage repair: a prospective evaluation of the microfracture technique. Am J Sports Med. 2006;34:14138.
12. Redondo ML, Beer AJ, Yanke AB. Cartilage restoration: mi
crofracture and osteochondral autograft transplantation. J Knee Surg. 2018;31:2318.
13. Hohmann E, Tetsworth K. Large osteochondral lesions of the femoral condyles: treatment with fresh frozen and irradi
ated allograft using the Mega OATS technique. Knee. 2016;
23:43641.
14. Zellner J, Grechenig S, Pfeifer CG, Krutsch W, Koch M, Welsch G, Scherl M, Seitz J, Zeman F, Nerlich M, Angele P. Clinical and radiological regeneration of large and deep osteochondral defects of the knee by bone augmentation combined with matrixguided autologous chondrocyte transplantation. Am J Sports Med. 2017;45:306980.
15. Berruto M, Delcogliano M, de Caro F, Carimati G, Uboldi F, Ferrua P, Ziveri G, De Biase CF. Treatment of large knee osteochondral lesions with a biomimetic scaffold: results of a multicenter study of 49 patients at 2year followup. Am J Sports Med. 2014;42:160717.
16. Patrascu JM, Freymann U, Kaps C, Poenaru DV. Repair of a posttraumatic cartilage defect with a cellfree polymer
based cartilage implant: a followup at two years by MRI and histological review. J Bone Joint Surg Br. 2010;92:11603.
17. Gudas R, Kalesinskas RJ, Kimtys V, Stankevicius E, Toliusis V, Bernotavicius G, Smailys A. A prospective randomized clinical study of mosaic osteochondral autologous transplan
tation versus microfracture for the treatment of osteochon
dral defects in the knee joint in young athletes. Arthroscopy.
2005;21:106675.
18. Trinh TQ, Harris JD, Flanigan DC. Surgical management of juvenile osteochondritis dissecans of the knee. Knee Surg Sports Traumatol Arthrosc. 2012;20:241929.