관련 문서
Units of the average power are watts, while units of complex power are volt-amps(VA), and the units of reactive power are volt-amp reactive (VAR)... Complex Power in
In order to analyze thermal stability and capacity loss according to the temperature of the battery cell by applying different C-rate discharge and
Effect of Soru Lower-leg Massage Therapy on Heart Rate Variability and Reactive Oxygen Species Concentration in
Factors affecting post-traumatic stress of general hospital nurses after the epidemic of Middle East respiratory syndrome infection: Journal of Korean Clinical
Full genome cloning and nucleotide sequence analysis of hepatitis C virus from sera of chronic hepatitis patients in Korea. Detection of hepatitis C virus RNA
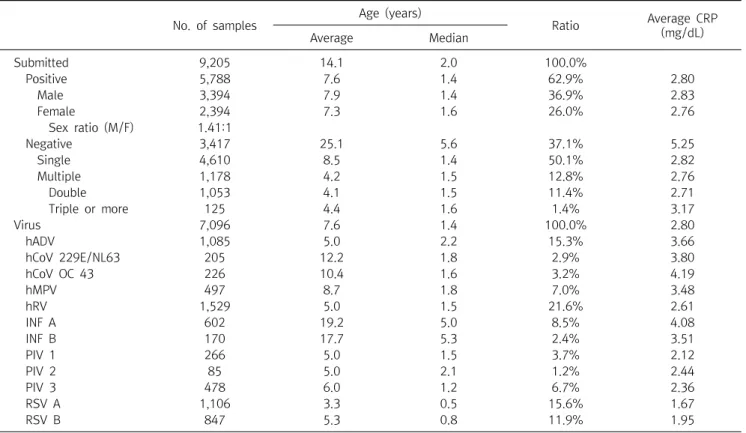
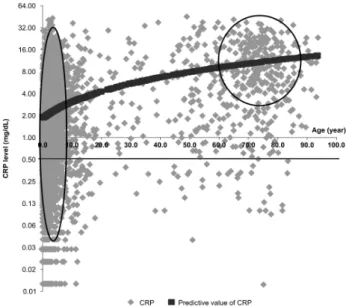
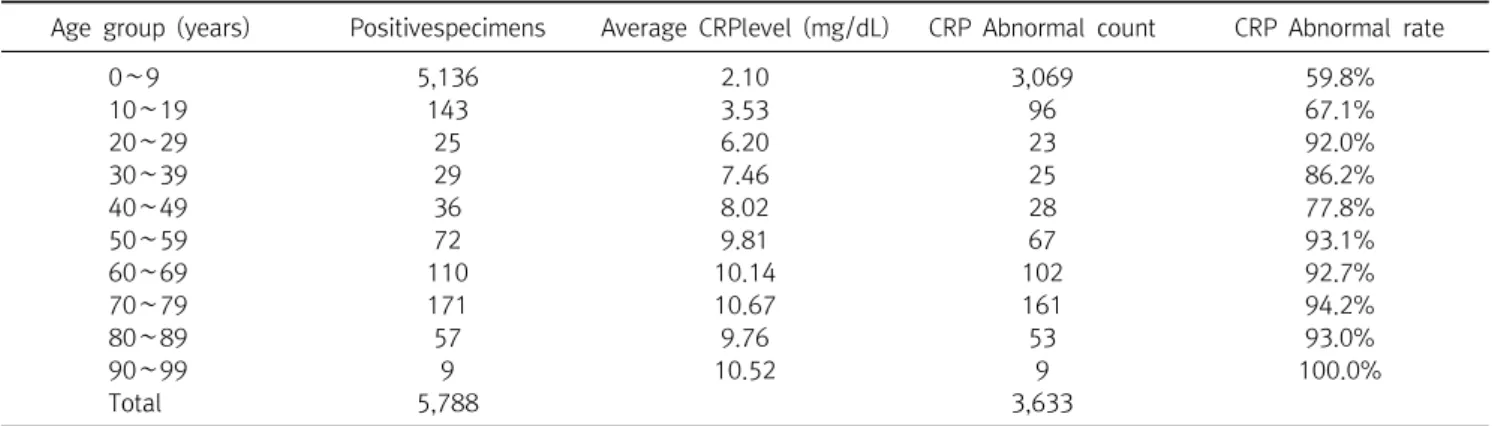
Whether to be or not the effect of tacrolimus has been examined in two ways : one is comparing erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) before
A study on the relationship between body mass index and the food habits of college students. Keilins respiratory chain concept and its
그러한 손상과 관련하여 적혈구 침강속도(erythrocyte sedimentation rate, ESR)는 비특이적이기는 하지만 염증성 반응을 나타내는 좋은