Abstract : Atrial fibrillation is an independent risk factor for stroke, and oral anticoagulation therapy with warfarin is effective in the prevention of stroke in atrial fibrillation. It has been reported that the prevalence of atrial fibrillation increases with age, and numbers of elderly patients who take warfarin is also increasing. As a result, increasing rate of bleeding associated with warfarin in elderly patients has been reported in previous studies. This study was designed to evaluate the incidence rate of bleeding in relation to age, and the factor associated with bleeding.
In this retrospective study, baseline characteristics, anticoagulant control (target INR of 2-3) and the incidence of bleeding were assessed in an elderly population (≥75 years) compared with a younger population (between 65 and 74 years). All patients were new warfarin users, attending anticoagulation service (ACS) at Samsung Medical Center from January 1, 2008 to August 31, 2009. Each patient was followed up by 1 year after starting taking warfarin.
A total of 155 patients were studied, and 100 patients in the younger group providing 83.1 per- son-years of follow-up and 55 patients in the elderly group providing 39.5 person-years of fol- low up. Between younger and elderly group, average of duration of INR within target range is
고령의 심방세동 환자의 Warfarin 치료 시, 출혈 발생률과 위험인자 분석
삼성서울병원 약제부, 경성대학교 약학대학
aIncidence Rate and Risk Factors of Bleeding Associated with Warfarin Therapy in Elderly Atrial Fibrillation Patients
Hyunbok Cho, Kyungah Min, Yongwon In, Youngmi Lee, Kiho Son
aDepartment of Pharmacy, Samsung Medical Center, 50 Irwon-dong, Gangnam-gu, Seoul, 135-710, Korea College of Pharmacy, Kyungsung University, 314-79 Daeyeon-dong, Nam-gu, Busan, 608-736, Korea
a회원학술보고
배경 및 목적
심방세동(Atrial fibrillation, AF)은 가장 일반적 으로 발생하는 부정맥의 형태이며
1)뇌졸중의 독립적 인 인자
2)로, 심방세동 환자의 경우 허혈성 뇌졸중의 위험이 6배 증가한다고 보고되었다.
3)심방세동의 발생빈도는 나이에 따라 증가하는 양상 을 보이며, 연령이 10세 증가함에 따라 심방세동의 odds ratio는 2배씩 증가한다고 보고되었다.
4)또한 심방세동 환자의 뇌졸중 발생위험을 평가하는 CHADS2 score 체계에서는 75세 이상의 연령을 위 험인자로 포함하고 있으며
5), 최근 유럽심장학회에서 권고된 CHA2DS2-VACs score 체계에서는 65세 에서부터 74세의 연령보다 75세 이상의 연령에 더 많은 점수를 부여하였다. 이러한 기준들은 심방세동 환자의 뇌졸중 발생 위험이 연령 증가와 연관되어 있
음을 보여준다.
6)몇몇 연구에서도 연령의 증가가 허 혈성 뇌졸중의 위험인자임이 알려졌다.
7-8)따라서 고 령의 심방세동 환자의 경우 뇌졸중 예방을 위한 적절 한 항혈전요법이 시행되어야 하며, warfarin은 비 판막성 심방세동 환자에서의 주요한 일차적 혈전색 전증 예방법으로 평가되었다.
9-13)그러나 warfarin은 그 치료역이 좁고 다양한 인자 에 의해 약효에 영향을 받으며, warfarin 복용 시 가 장 중요한 부작용은 출혈이다. 연령 증가는 출혈 증가 에 영향을 미치는 인자로 알려져 있으며, 이러한 출혈 부작용의 위험으로 인해 고령에서는 warfarin의 사 용이 충분히 이루어지지 못하는 경향이 있다.
14-17)뇌졸중 위험에 취약한 고령의 심방세동 환자의 경 우, 효과적이며 안전한 항응고 약물요법이 필요하나 이전에 시행된 몇몇 연구에서는 고령 환자에서 warfarin으로 인한 출혈 부작용이 유의하게 증가하 57.5% and 61.5% respectively, and there is no significant difference (p=0.269). No difference of incidence of minor bleedings was found between the elderly group and the elderly group(p=0.395).
Major bleedings were developed 1 event in younger group and 2 events in the elderly group.
Incidence rate of major bleeding in the elderly group was higher than the younger group in 4.21 folds, but it was not statistically significant (95% CI, 0.38-46.4). 42.6% of all bleeding and 33.3%
of major bleeding were developed in first 90 days after starting warfarin therapy. Male (p=0.031) was analyzed as a risk factor for bleeding associated with warfarin in the all 155 patient, and history of cancer was analyzed that had effect on the analyzing sex as a risk factor for bleeding.
However, we couldn't find the risk factors of bleeding for the elderly group.
These findings suggest that older age and early period of warfarin therapy were related to increasing of bleeding caused by warfarin, and needed much care for anticoagulation therapy.
Further studies to analyse risk factors for bleeding and there results may be help provide better anticoagulation therapy to elderly atrial fibrillation patients for prevention of stroke.
[Key words] atrial fibrillation, older age, bleeding associate with warfarin, risk factors
투고일자 2011. 4. 27; 심사완료일자 2011. 5. 22; 게재확정일자 2011. 5. 30였다고 보고하였다.
18-20)국내에서도 고령 인구의 증가로 인해 warfarin 복 용이 필요한 고령의 심방세동 환자가 증가하고 있으 므로, 본 연구에서는 warfarin을 복용하는 75세 이 상의 심방세동 환자에서의 전반적인 출혈 발생률을 파악하고 이에 영향을 미치는 위험인자를 탐색하여, 안전하고 효과적인 항응고 약물요법을 제공하는데 참고하고자 하였다.
연구방법
1. 용어의 정의
이 연구에서 사용한 용어의 정의는 다음과 같다.
1.1. Person-year
21)해당 군에 포함된 환자들의 분석 기간을 모두 합하 여, 연(year) 단위로 표현한 기간이며, 이를 사용하 여 환자들의 분석 기간을 모두 반영하였다.
1.2. 출혈 부작용 발생률
21)1.3. Major bleeding
21),22)두개내출혈(intracranial hemorrhage), 경막하출 혈(subdural hemorrhage), 복막후출혈(retroperi- toneal hemorrhage), warfarin의 복용 중단이나 입원치료를 유발한 주요 장기에서의 출혈, 약물적 중 재(transfusion, vitamin K 또는 fresh frozen plasma)가 필요했던 출혈로 정의하였다.
1.4. Minor bleeding
19)코피(epistaxis), 잇몸 출혈(gingival bleeding), 결막 출혈(conjunctival hemorrhage) 미세혈뇨 (microscopic hematuria) 등 major bleeding을 제외한 모든 출혈로 정의하였다.
2. 연구대상의 선정 및 제외 기준
연구는 2008년 1월 1일부터 2009년 8월 31일까지 삼성서울병원 항응고약물상담실(Anticoagulation Service, ACS)에 심방세동을 적응증으로 항응고약물 상담이 의뢰되었던 65세 이상의 환자 중, 처음 war- farin을 복용하며 target INR 범위가 2-3인 환자를 대상으로 하였다. 고령군의 기준은 75세로 하고, 75 세 미만의 환자군과 75세 이상의 환자군으로 층화하 여 분석을 시행하였다. 대상 환자 중 분석 기간 내에 타병원에 입원하여 용량 조절을 받았던 경우, war- farin 시작 시 간기능 검사수치가 정상 범위(AST, ALT≤40)에 포함되지 못한 경우는 제외하였다.
3. 연구방법
대상 환자들의 전자의무기록(Electronic medical record, EMR)과 항응고약물상담 시행 시 작성하게 되는 항응고약물 상담 환자 전자 차트를 후향적인 방 법으로 분석하고, 효과 및 부작용은 2개의 군으로 나 누어 상호 비교, 평가 하였다. 분석은 warfarin 복 용 시작일 기준으로 1년의 기간을 대상으로 하였으 며, 1년 이내 major bleeding, warfarin 복용 중 단, 타원 전원 등이 발생한 경우에는 해당 시점 이후 의 자료 분석은 중단하였다.
3.1. 조사 내용
환자의 성별, 연령, 기저질환(고혈압, 당뇨, 고지질 혈증, 이전의 뇌졸중 병력, 위궤양, 심부전, 암, 이전 의 출혈 여부), 분석 기간 중 음주 여부, 병용약물의 개수, aspirin 병용, 복용오류 여부, 건강기능식품 복용 여부 등을 조사하였다.
3.2. INR 조절 평가
Warfarin의 항응고 효과는 INR로 나타내며, INR 조절의 평가는 warfarin 복용 시작 후 INR 2 이상 에 도달한 시점부터 이루어졌다. 총 INR 측정 횟수 중 target INR을 유지한 횟수의 비율, 대상 기간 중 target INR을 유지한 기간의 비율을 각각 per-
출혈 부작용 발생률 = 분석기간중 출혈 부작용의 발생횟수
person - year
centage로 표기하여 평가하였고, INR 유지 기간은 Rosendaal 등에 의해 기술된 선형 보간법
23)을 사용 하였다.
3.3. 출혈 부작용 평가
출혈 부작용 발생을 평가하기 위해서 분석 기간 중 총 출혈 부작용(major/minor bleeding) 발생 횟수 와 비율, 출혈과 연관되어 있는 INR 값, 첫 출혈 발 생까지의 기간(time to bleeding), 출혈 부작용에 대한 중재 여부와 그 내용을 분석하였다. 출혈과 연 관된 INR 측정값은 출혈이 발생한 당시의 INR 값 또는 출혈 부작용 발생 이전 8일 이내에 측정된 값으 로 정의하였다.
24)4. 통계방법
SPSS version 18.0을 사용하여, 연속형 변수의 경우 independent t-test 또는 Mann-Whitney analysis를, 범주형 변수의 경우, chi-square test 또는 Fischer's exact test를 시행하였다. Major bleeding 발생률 분석은 Poisson regression model로 시행하였으며, 위험인자 분석은 multi- variable logistic regression model로 시행하였 다. 각 항목은 p-value가 <0.05일 경우 통계학적 유의성이 있는 것으로 평가 하였다.
연구결과
1. 대상 환자군의 특성
2008년 1월 1일부터 2009년 8월 31일까지 총 1년 8개월 동안 삼성서울병원 항응고약물상담실에 심방 세동을 적응증으로 의뢰된 65세 이상의 환자 중 target INR이 2-3이었던 환자는 총 158명이었으 며, 이 중 제외기준에 해당하는 3명(타원에 입원하여 용량 조절(2명), warfarin 시작 시 간수치 이상(1명) 을 제외한 155명이 최종적으로 연구에 포함되었다.
대상 환자군의 특성을 비교한 결과는 Table 1에 나 타내었다. 75세 미만군은 100명이었으며 평균 연령
은 69.3±3.04세, 총 분석 기간은 83.1 person- year 이었다. 75세 이상군은 55명이었으며, 평균 연 령은 78.9±3.37세(나이 범위, 75-86세), 총 분석 기간은 39.5person-year 이었다. 환자 특성 중 암 과 건강식품 복용 여부에서 두 군간의 차이를 보였으 며, 두 항목 모두 75세 미만군에서 더 많이 관찰되었 다. 155명 중 분석 기간이 1년 미만이었던 환자는 43 명이었으며, 이 중 75세 미만군은 22명, 75세 이상 군은 21명이었다. 이에 해당하는 사유는 타원 전원 또는 내원 중단(20명), aspirin 또는 clopidogrel로 변경(16명), 간 질환 발생(2명), 사망(2명), major bleeding(3명) 등이었다. 사망한 2명의 환자는 아밀 로이드증과 심부전을 사인으로 하는 1명, 고령으로 인한 병사를 사인으로 하는 1명이었다.
No. of patients(%) Age, mean±SD(y) (range)
Male Sex Female
Hypertension Diabetes mellitus Hyperlipidemia Previous stroke Peptic ulcer Heart failure Cancer History of bleeding Alcohol use No. of medication Aspirin therapy Herbal medication use Incorrect dose
* NS: Not Significant
Age < 75 (n=100) 69.3±3.04
(65-74)
Age ≥ 75 (n=55) 78.9±3.37
(75-86)
p-value
-
54 (54.0) 46 (46.0) 74 (74.0) 33 (33.0) 17 (17.0) 44 (44.0) 5 (5.0) 30 (30.0) 17 (17.0) 9 (9.0) 13 (13.0)
4.3 22 (22.0) 38 (38.0) 59 (59.0)
23 (41.8) 32 (58.2) 39 (70.9) 14 (25.5) 6 (10.9) 19 (34.5) 2 (3.6) 12 (21.8)
1 (1.8) 5 (9.1) 4 (7.3) 4.3 12 (21.8) 6 (10.9) 32 (58.2)
NS*
NS NS NS NS NS NS NS 0.005
NS NS NS NS
< 0.001 NS
Table 1. Patients Characteristics
2. INR 조절
총 INR 측정 횟수는 3,095회였으며, 75세 미만군 에서는 2,028회, 75세 이상군에서는 1,067회의 INR이 측정되었다. 90일 이내 INR f/u 횟수는 75 세 미만군에서 8.12회, 75세 이상군에서 8.00회 (p=0.72)이었다.
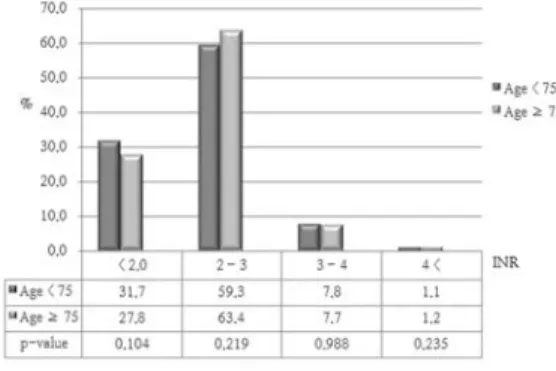
총 측정 횟수 중 target INR 범위를 유지한 횟수 의 비율은 75세 미만군에서 59.3%, 75세 이상 군에 서 63.4%(p=0.219)이었고, target INR 범위 미만 인 비율은 75세 미만군에서 31.7%, 75세 이상군에 서 27.8%(p=0.104)이었다. Target INR 범위를 초 과한 경우, INR 4 이하의 비율은 75세 미만군과 75 세 이상군에서 각각 7.8%, 7.7%(p=0.988)이었으며 INR 4 초과의 비율은 각각 1.1%, 1.2%(p=0.235)이 었다(Fig. 1).
각 환자의 INR을 유지한 평균 기간을 분석한 결 과, 75세 미만군에서 57.5%, 75세 이상군에서 61.5%의 기간 동안 target INR 범위를 유지하였 다(P=0.269). Target INR 범위 미만을 유지한 기간은 75세 미만군에서 34.2%, 75세 이상군에서 30.1%(p=0.091)이었다. Target INR을 초과한 기간의 경우, INR 4 이하의 기간은 75세 미만군 과 75세 이상군에서 각각 7.2%, 7.6%(p=0.683) 이었으며 INR 4 초과의 기간은 각각 1.2%, 0.8%(p=0.151)이었다(Fig. 2).
3. 출혈 부작용
연구기간 중 전체 155명의 환자에서 47건의 출혈 부작용이 발생하였다.
3.1. 출혈 부작용 발생률
전체 47건의 출혈 부작용 중, 75세 미만군에서는 32건의 출혈 부작용이 발생했으며, 75세 이상군에서 는 15건의 출혈 부작용이 발생했다(Table 2.).
Major bleeding은 전체 155명의 환자에서 총 3건 이 발생하였다. 75세 미만군에서 1건이 발생하였고 발생률은 0.012건/person-year이었으며, 75세 이 상군에서 2건이 발생하였고 발생률은 0.051건/per- son-year 이었다. 75세 미만군에 대한 75세 이상군 의 상대위험도는 4.21(95% CI, 0.38-46.4)이었다.
Major bleeding의 사례로는 70세 남성 환자가 warfarin 복용 후 37일째에 발생한 hematuria로 인해 warfarin의 복용을 중단한 경우였으며 당시 INR은 2.86 이었다. 84세 여성 환자는 warfarin 복용 후 229일 째에 bruise와 hematuria를 주소로 응급실에 내원하였으며 당시 INR은 5.20으로 vitamin K 5mg을 정맥투여 한 후 입원하여 치료를 받았다. 출혈 발생 1주일 전부터 oxolamine과 도라 지즙을 복용했던 이력이 INR 상승의 원인으로 생각 된다. 또한 80세 여성 환자가 warfarin 복용 후 142 일 째에 melena로 인해 입원하여 치료를 받았으며, 이후 warfarin을 중단하였다(Table 4.).
Fig. 1 Comparing the proportion of the number of INR results below, within and over the target INR
Fig. 2 Comparing the proportion of the duration
below, within and over the target INR
Minor bleeding은 총 44건이었으며, 75세 미만군 에서는 31건, 75세 이상군에서는 13건이 발생하였다.
각각 결막하출혈(conjunctival hemorrhage) 16건, 잇몸 출혈(gingival bleeding) 9건, 코피(epistaxis) 6건, 미세 혈뇨(microscopic hematuria) 5건, 치질 로 인한 출혈(hemorrhoid bleeding) 4건, 객혈 (hemoptysis) 4건이 발생하였고, 높은 INR에 대해 warfarin 용량을 조절했던 경우를 제외하고 다른 조 치 없이 해결되었다. 1년 이상의 자료가 있었던 환자 들의 경우, 75세 미만군에서 23건, 75세 이상군에서 10건이 발생(p=0.35)하였다(Table 2.).
전체 발생한 47건의 출혈 부작용 중에서 14건 (29.8%)은 INR 기록이 없거나 출혈 발생과 INR 측정 과의 시간적 차이로 인해 INR 측정값이 누락되었고, 33건에서 출혈과 연관된 INR 값을 확인할 수 있었다.
Target INR 미만인 측정값은 4건(12.1%)이었으며 모 두 75세 미만군에 해당하였다. Target INR 이내의 측정값은 24건(72.7%)이었으며, 이 중 17건이 75세 미만군에, 7건이 75세 이상군에 해당하였다. Target INR 초과 범위의 5건(15.2%)의 측정값 중 3건은 75 세 미만군에, 2건은 75세 이상군에 해당하였다.
전체 출혈 중 INR 4 초과에서 발생한 출혈은 2건 으로, 모두 75세 이상군에서 발생하였고, 이 중 minor bleeding과 major bleeding은 각각 1건씩 이었다.
3.2. 치료 초기(90일 이내) 출혈 부작용 발생률 Warfarin 사용 시작 후 90일 이내에 발생한 출혈 은 전체 47건의 출혈 중 20건(42.6%)이었다(Table 3.). Warfarin 사용 후 90일 이내 발생한 출혈은 75
1 2
3
Table 4. Cases of Major Bleeding during Follow-up Study No.
M F
F
Sex
70 84
80
Age
Hematuria Bruise, hematuria
Melena
Type
37 229
142
Time to bleeding (d)
2.86 5.20
-
INR
Discontinuation of warfarin Administration of vitamin K at ER, and hospitalization Hospitalization(Dx. with multiple gastric ulcer),
Discontinuation of warfarin
Result
Major bleedingMinor bleeding
possible duration of analysis≥1yrs
1 (33.3) 19 (43.2) 12 (36.4)
1 (100.0) 10 (32.3) 7 (30.4)
0 (0.0) 9 (69.2) 5 (50.0)
Table 3. Comparison of incidence of bleedings developed in first 90 days after Starting Warfarin Therapy Overall
No.(%) Age < 75 Age ≥ 75
-
p=0.853
Statistical significance
Major bleedingNo.
Incidence rate Minor bleeding
possible duration of analysis≥1yrs
3
44 33
1 0.012/person-year
31 23
2 0.051/person-year
13 10
Table 2. Comparison of incidence of bleedings
Overall Age < 75 Age ≥ 75
RR, 4.21 95% CI, 0.38-46.4
p=0.395
Statistical significance
세 미만군에서 11건(34.4%), 75세 이상군에서 9건 (60.0%)이었다. 1년 이상의 자료가 있었던 환자들의 경우, 75세 미만군에서 7건(30.4%), 75세 이상군에 서 5건(50.0%)이 발생하였다(p=0.853). 90일 이내 에 발생한 major bleeding은 1건이었으며, 75세 미 만군에서 발생하였다.
4. 출혈 부작용의 위험인자 분석
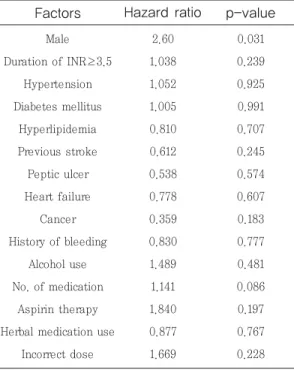
전체 155명 중에서 출혈이 발생한 환자는 총 33명 (47건)이었다. 환자의 성별, 기저질환, 연구기간 중 음주 여부, 이전의 출혈 발생력, 병용약물의 개수, aspirin 병용여부, 건강식품 복용여부, 복용 오류 여부 등을 위험인자로 고려하여 분석한 결과, 남성 이 출혈의 위험인자로 분석(p=0.031)되었으며, hazard ratio는 2.60(95% CI, 0.161-0.916)이었 다(Table 5.).
75세 이상군에서 출혈이 발생한 환자는 총 9명(15 건)이었다. 성별, INR 3.5 이상의 기간, 당뇨, 이전 의 뇌졸중 병력, 병용약물 개수, 복용 오류 여부를 대 상으로 분석한 결과, 분석에 포함된 모든 인자에서 통계학적인 유의성은 나타나지 않았다(Table 6.).
고찰
심방세동은 가장 일반적으로 나타나는 부정맥의 한 형태이며
1), 뇌졸중 발생의 독립적인 인자로 알려져 있다
2). 심방세동은 연령이 증가함에 따라 발생빈도 가 증가
4)할 뿐 만 아니라 심방세동으로 인한 뇌졸중 의 발생 위험도 연령에 따라 증가하게 된다.
5)-8)따라 서 고령의 심방세동 환자일수록 warfarin을 사용한 뇌졸중 예방요법이 필요하다. 그러나 고령은 war- farin의 중요한 부작용인 출혈의 위험인자로 알려져 있으며, 이와 관련하여 warfarin을 복용하는 고령 환자에서의 major bleeding의 증가
18-20), 고령에서 의 warfarin 사용 감소
14-17)등이 보고되기도 하였다.
INR 조절 정도는 출혈에 영향을 미친다고 알려져 있으며, 심방세동 환자의 출혈 위험을 평가하는 Pisters 등의 연구에서는 불안정한 INR 또는 tar- get INR 유지 기간이 짧은 경우를 출혈의 위험인자 로 고려 25) 하였고, Fang 등은 3.5이상의 INR이 출 혈 위험의 증가와 연관되어 있다고 보고
26)하였다.
Factors
Male Duration of INR≥3.5Hypertension Diabetes mellitus
Hyperlipidemia Previous stroke Peptic ulcer Heart failure Cancer History of bleeding
Alcohol use No. of medication
Aspirin therapy Herbal medication use
Incorrect dose
Hazard ratio
2.60 1.038 1.052 1.005 0.810 0.612 0.538 0.778 0.359 0.830 1.489 1.141 1.840 0.877 1.669p-value
0.031 0.239 0.925 0.991 0.707 0.245 0.574 0.607 0.183 0.777 0.481 0.086 0.197 0.767 0.228Table 5. Analysis of Risk Factors for Bleeding
Associated with Warfarin in All Patients Group (n=155)
Factors
Male Duration of INR≥3.5Diabetes mellitus Previous stroke No. of medication
Incorrect dose
p-value
0.792 0.208 0.698 0.803 0.074 0.961Hazard ratio
1.224 1.104 0.621 0.820 0.685 1.037