Outcome of Gamma Knife Radiosurgery for Trigeminal Neuralgia
Sang Ryong Jeon, M.D., Dong Joon Lee, Ph.D.,* Jeong Hoon Kim, M.D., Chang Jin Kim, M.D., Yang Kwon, M.D.,
Jung Kyo Lee, M.D., Byung Duk Kwun, M.D.
Department of Neurological Surgery, Asan Medical Center, College of Medicine, University of Ulsan, Seoul, Korea
Department of Neurological Surgery,* College of Medicine, University of Inje, Seoul, Korea
= Abstract =
삼차신경통에 대한 감마나이프방사선 수술
울산대학교 의과대학 신경외과학교실, 인제대학교 의과대학 신경외과학교실
*전상룡·이동준*·김정훈·김창진·권 양·이정교·권병덕
bjective:This study was undertaken to analysis gamma knife radiosurgery(GKR) effect for trigeminal neuralgia after long term follow-up.
Methods:There were 11 trigeminal neuralgia patients. The authors irradiated 67-85 Gy maximally to the nerve root entry zone(NREZ) using single 4mm collimator, just 1-6mm lateral side from the junction of the trigeminal nerve and pons. For the first 3 cases, we targeted the junction between the nerve and the pons. In theses cases, the pons was irradiated 56 or 60 gray in the surface. In the later 8 cases, the isocenter is positioned more distal side so that the brain stem surface would receive less than the 20% isodose.
Results:The average follow-up duration was 25 months(13-50 months). Pain relief was noticed within a week to 5 months. In 3 patients, pain was relieved completely and in other 3 patients, mark improvement was achieved(80-90%).
Remaining 4 patients showed significant improvement(30-50%). There was recurrence in only one case and she complained with similar intensity of pain at the last follow-up. There was no significant complication related to GKR.
Conclusion:GKR is considered effective for trigeminal neuralgia based on the long term follow-up evaluation, but more clinical experience is needed to evaluate the efficacy of GKR for trigeminal neuralgia as a primary treatment modality.
KEY WORDS:Gamma knife radiosurgery・Trigeminal neuralgia・Root entry zone.
Introduction
The surgical methods for medically intractable trigemi- nal neuralgia are microvascular decompression(MVD) and/or percutaneous RFG or glycerol rhizotomy. But now radiosurgery is used as another method to this condition.
Since the first radiosurgical treatment of trigeminal neural- gia which was performed by Leksell in the early 1950s
13), the target was changed from trigeminal ganglion to the root entry zone of trigeminal nerve
1)20)12). And the dosages of
stereotactic irradiation to target are variable now
7). In our study, we report our long-term experience in typical trige- minal neuralgia who had gamma knife radiosurgery.
Methods and Material
The mean age of patients was 51 years(range, 24-71).
Eight patients had undergone prior surgical treatment.
Among them, one patient had 2 procedures such as mic- rovascular decompression(MVD) after glycerol injection at trigeminal ganglion. There were 4 males and 7 females. No
OOOO
one had underlying neurological disease.
All patients had Gamma Knife radiosurgery(GKR) us- ing the Leksell Unit. By the magnetic resonance image (MRI) we identified the trigeminal nerve in its course from the pons to Meckel’s cave. Stereotactic coordinates were calculated for a single 4mm isocenter, just 1-6mm lateral side from the junction of the trigeminal nerve and pons.
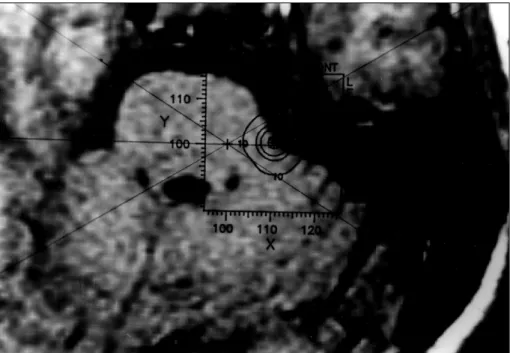
At the first 3 cases, we targeted the junction between the nerve and the pons(Fig. 1). In theses cases, the pons was iradiated above 56 gray. In the later cases, The isocenter is positioned more lateral side so that the brain stem surface usually received less than the 20% isodose(Table 1)(Fig. 2).
A range of maximum radiosurgical doses were selected between 67 and 85 gray(Table 1). All patients were disch- arged within 24 hours. Patients were evaluated by follow- up studies through outpatient department or telephone interview with regard to the severity and frequency of pain compared to preradiosurgical status. The patient him/her- self made the classification of the pain relief using the percentile scale
7)13).
Results
The mean follow-up duration was 25 months(range 13- 50). The effects of GKR for pain have begun early. In 7 cases, the effects developed within 1 month(3 cases within 1 week) and in others at postoperative second, third, fifth month respectively.
In 3 patients, pain were relieved completely at the last follow up and in 3 patients, markedly improved(80-90%).
Another 4 patients showed significant improvement(30- 50%)(Table 1). There was recurrence in only one case and she complained same amount of pain at the last follow-up.
There was no side effect related to GKR in all cases. Only 3 patients(case 3, 9, 11) showed gradual decrease of sym- ptom. Most patients(case 1, 2, 4, 5, 6, 7, 8, 10) showed fluctuation of symptom during follow-up.
One patient(case 1) complained hypesthesia in tongue 8 months after GKR but it was tolerable. Before GKR, all patients had been taking medication(carbamazepine or carbamazepine with diphenyl hydantoin), but at the last follow-up, 6 patients(55%) were taking medication and especially only one among the patients who were pain- free.
Discussions
In 1971, Lars Leksell discussed results from two patients who underwent radiosurgery for trigeminal neuralgia in 1953
5)8). Both patients had irradiation of the trigeminal ganglion using stereotactic guidance. The first patient who had been treated with 16.5Gy complained no trigeminal neuralgia during 18 years. And the second, 22Gy-treated patient also experienced no trigeminal neuralgia. In 1991, Lindquist, et al., reported 22 cases of patients who had gasserian ganglion radiosurgery by target localization aided by stereotactic cisternograghy. But the results were not good. Thirteen of the 22 patients were pain free after 6 months but only 4 remained so after 2.5 years
9). Kond- ziolka, et al. reported that they concluded that gasserian ganglion was probably not appropriate as the primary ra- diosurgery target and radiosurgery to root entry zone had
Table 1. Patient characteristics who irradiated to the REZ and follow-up results No. Age/
Sex Location Previous treatment
Maximum dose(Gy)
Dose to pons (isodose % line)
Medication before GKR
Medication after GKR
Residual pain
Onset of effect
F/U duration (months) 1 53/F Rt V2, 3 MVD* GI† 67 60(90%) carbamazepine carbamazepine 20% 3m‡ 50 2 60/F Lt V2, 3 GI 67 60(90%) carbamazepine none 50% 7d§ 16 3 71/F Rt V2 AI¶ 80 56(70%) carbamazepine
+DPH
none free 1m 48
4 42/F Rt V2, 3 MVD 70 35(50%) carbamazepine carbamazepine 100% 9d 26 5 45/M Rt V3 RFL# 80 16(20%) carbamazepine none free 15d 27 6 50/M Rt V2 MVD 80 16(20%) carbamazepine carbamazepine 50% 3d 22 7 65/M Rt V2 none 80 16(20%) carbamazepine none 10% 2m 20 8 24/F Rt V2 none 70 14(20%) carbamazepine none 70% 5m 24 9 39/F Lt V3 none 85 17(20%) carbamazepine carbamazepine 50% 2m 18 10 55/F Rt V2 RFL×2 80 16(20%) carbamazepine carbamazepine 10% 9d 16 11 62/M Lt V2 MVD 80 16(20%) carbamazepine carbamazepine free 3d 13
*:microvascular decompression #:radiofrequency lesion making
†:glycerol injection at trigeminal ganglion ¶:alcohol injection at trigeminal ganglion
‡:months §:days
better outcome(58% pain free)
5)6)12).
The advantage of proximal nerve or root entry zone as the irradiation target came from two aspects. the first one is that in this area, the central myelin(oligodendrocyte) be- came peripheral(schwann cell) myelin. So a stronger ra- diobiological effect could occur at this portion
3)5)10)11). The second one is that the root entry zone can be identified clearly with MR images as it traverses the cerebrospinal
fluid of the posterior fossa
5).
The authors identified easily the junction between pons and trigeminal nerve as well as root entry zone even in the patients after MVD. In the first 3 cases of this series, the centers of targets are located lateral margin of root at the junction to pons(Fig. 1). In the later 8 cases, we moved the target into central part and more distal side of root so that the brain stem surface usually received less than the 20%
Fig. 1. The centers of targets are located at lateral margin of root at the junction to pons. Maximum dose was 60-67 Gray and the 70-90% isodose curve is seen on the pons margin(case 1,2,3).
Fig. 2. In the fourth case, we moved the target into root center and more distal side so that the brain stem received less than the 20% isodose(case 4-11).
isodose(Fig. 2). But in the case 4, the nerve root was devi- ated to brain stem due to previous operation(MVD), so the 50% isodose curve was put on the surface of pons. The ne- rve root entry zone was demarcated easily by MRI in all cases including MVD patients. The two target groups showed no differences of results at the last follow-up in effects or complications of brain stem. Only in the first case, she com- plained tongue hypesthesia after 8 months but it was tolerable.
The onset of effects started early. In seven cases, the effects has begun within 1 month and especially 3 cases showed the effects within 1 week. The latest onset was fifth month after GKR.
Interestingly, many cases showed symptom fluctuation during follow-up. In only 3 cases(case 3, 9, 11), pain dec- reased gradually without fluctuation. There were differences in fluctuation ranges but the outcome at the last follow-up was not related with ranges of symptom fluctuation.
There was no difference of effects between the group which had other treatment before GKR and the group which had been treated only by GKR(p=0.65, chi-square).
The first case was treated by microvascular decompression and glycerol injection 18 months and 8 months before GKR respectively, but there was no effect from MVD.
After she treated by GKR, the pain was decreased 80%.
The tenth case had no effect from ganglion lesion making by radiofrequency generator. But GKR reduced 80% of trigeminal neuralgia in this case.
Conclusion
Pain relief of trigeminal neuralgia after GKR is effective during long term follow-up periods(improvement≥50%;
82%), and no significant complication. Although more clinical experiences are needed to evaluate the efficacy of GKR as a primary treatment modality for trigeminal neu- ralgia but we believe that GKR will become one of the im- portant primary management strategies.
•
논문접수일:2000년 3월 29일•
심사완료일:2000년 8월 16일•
책임저자:전 상 룡138-736 서울 송파구 풍납동 388-1
울산대학교 의과대학 서울중앙병원 신경외과학교실 전화:02) 2224-3554, 전송:02) 476-6738 E-mail:srjeon @www.amc.seoul.kr
References
1)
Jessell TM, Kelly DD:Pain and analgesia, in Kandel ER,Schwartz JH, Jessell TM ( eds ): Principals of neural science.
New York/Amsterdam : Elsevier, 1991, pp385-399
2)
Kimura J, Rodnitzky RL, Okawara SH:Electrophysiologicanalysis of aberrant regeneration after facial nerve paralysis.
Neurology 25 : 989-993, 1975
3)
van der Kogel AJ:Central nervous system radiation injuryin small animal models, in Gutin PH, Leibel SA, Sheline GE, et al ( eds ): Radiation Injury to the Nervous System. New York : Raven Press, 1991, pp91-111
4)
Kondziolka D, Flickinger JC, Lunsford LD, Habeck M:Trigeminal neuralgia radiosurgery : The university of Pitts- burgh experience. Stereotact Funct Neurosurg 66 ( suppl 1 ):
343-348, 1996
5)
Kondziolka D, Lunsford LD, Flickinger JC, Young RF, Ver- meulen S, Duma CM, et al:Stereotactic radiosurgery for tri-geminal neuralgia : a multiinstitutional study using the gamma unit. J Neurosurg 84 : 940-945, 1996
6)
Kondziolka D, Lunsford LD, Habek M, Flickinger JC:Gam-ma knife radiosurgery for trigeminal neuralgia. Neurosurg Clin Nor Am 8 : 1 : 79-85, 1997
7)
Kondziolka D, Perez B, Flickinger JC, Habeck M, Lunsford LD:Gamma knife radiosurgery for trigeminal neuralgia.Arch Neurol 55 : 1524-1529, 1998
8)
Leksell L:Stereotactic radiosurgery in trigeminal neuralgia.Acta Chir Scand 137 : 311-314, 1971
9)
Lindquist C, Kihlström L, Hellstrand E:Functional neuro-surgery-a future for the gamma knife? Stereotact Funct Neu- rosurg 57 : 72-81, 1991
10)
Mastaglia FL, McDonald WI, Watson JV, Yogendran K:Effects of X-radiation on the spinal cord : an experimental study of the morphological changes in central nerve fibers.
Brain 99 : 101-122, 1976
11)
Mehta MP, Kinsella TJ:Cavernous sinus cranial neuropa-thies : is there a doseresponse relationship following radio- surgery? Int J Radiat Oncol Biol Phys 27 : 477-480, 1993 12)
Rand RW, Jacques DB, Melbye RW, Copcutt BG, Fisher MR,Levenick MN:Leksell Gamma Knife treatment of tic doulo-
ureux. Stereotact Funct Neurosurg 61 : 93-102, 1993 13)
Urgosik D, Vymazal J, Vladyka V, Liscak R:Gamma knifetreatment of trigeminal neuralgia : clinical and electrophy- siologic study. Stereotact Funct Neurosurg 70 ( suppl 1 ):
200-209, 1998
삼차신경통에 대한 감마나이프방사선 수술
울산대학교 의과대학 신경외과학교실, 인제대학교 의과대학 신경외과학교실
*전상룡·이동준*·김정훈·김창진·권 양·이정교·권병덕