Background/Aims: This nationwide, multicenter prospective randomized controlled trial aimed to compare the efficacy and safety of 10-day concomitant therapy (CT) and 10-day sequential therapy (ST) with 7-day clarithromycin-containing triple therapy (TT) as first-line treatment for Helicobacter pylori infection in the Korean population. Methods: Patients with H. pylori infection were assigned randomly to 7d-TT (lansoprazole 30 mg, amoxicillin 1 g, and clarithromycin 500 mg twice daily for 7 days), 10d-ST (lansoprazole 30 mg and amoxicillin 1 g twice daily for the first 5 days, followed by lansoprazole 30 mg, clarithromycin 500 mg, and metronidazole 500 mg twice daily for the remaining 5 days), or 10d-CT (lansoprazole 30 mg, amoxicillin 1 g, clarithromycin 500 mg, and metronidazole 500 mg twice daily for 10 days). The primary endpoint was eradication rate by intention-to-treat (ITT) and per-protocol (PP) analyses.
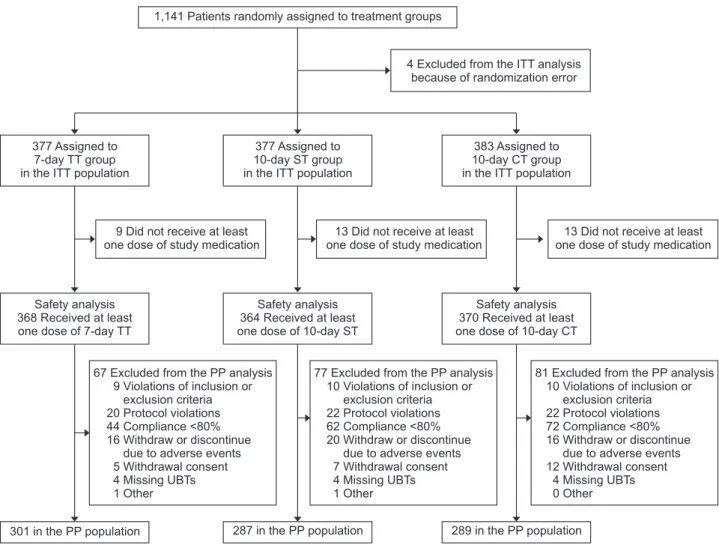
Results: A total of 1,141 patients were included. The 10d-CT
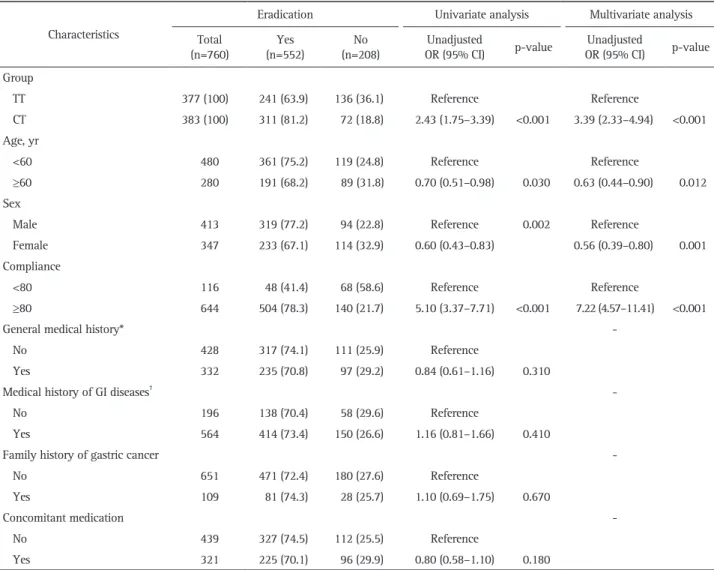
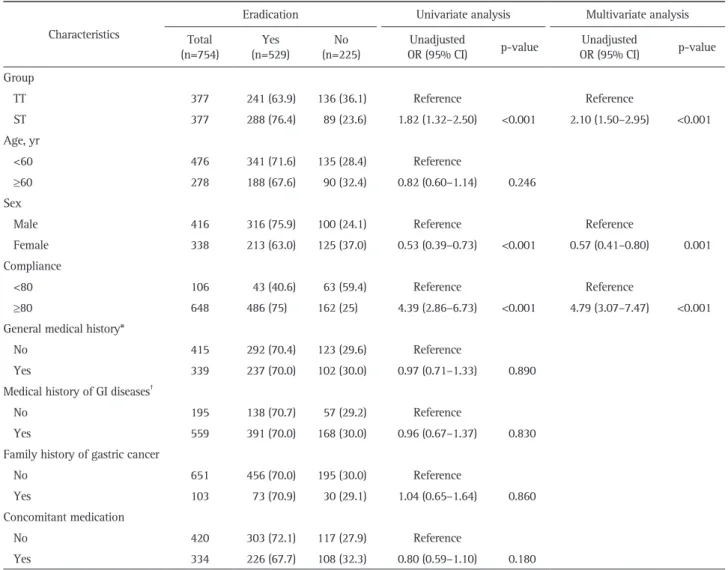
protocol achieved a markedly higher eradication rate than the 7d-TT protocol in both the ITT (81.2% vs 63.9%) and PP analyses (90.6% vs 71.4%). The eradication rate of the 10d- ST protocol was superior to that of the 7d-TT protocol (76.3%
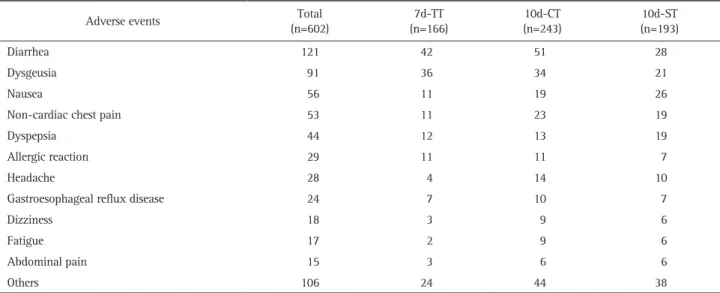
vs 63.9%, ITT analysis; 85.0% vs 71.4%, PP analysis). No significant differences in adherence or serious side effects were found among the three treatment arms. Conclusions:
The 10d-CT and 10d-ST regimens were superior to the 7d- TT regimen as standard first-line treatment in Korea. (Gut Liver 2019;13:531-540 )
Key Words: Concomitant therapy; Disease eradication;
Helicobacter pylori; Triple therapy; Sequential therapy
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Ten-Day Concomitant, 10-Day Sequential, and 7-Day Triple Therapy as First- Line Treatment for Helicobacter pylori Infection: A Nationwide Randomized Trial in Korea
Beom Jin Kim
1, Hyuk Lee
2, Yong Chan Lee
3, Seong Woo Jeon
4, Gwang Ha Kim
5, Hyun-Soo Kim
6, Jae Kyu Sung
7, Dong Ho Lee
8, Heung Up Kim
9, Moo In Park
10, Il Ju Choi
11, Soon Man Yoon
12, Sang Wook Kim
13, Gwang Ho Baik
14, Ju Yup Lee
15, Jin Il Kim
16, Sang Gyun Kim
17, Jayoun Kim
18, Joongyup Lee
19, Jae Gyu Kim
1, and Jae J. Kim
2, Korean College of Helicobacter and Upper Gastrointestinal Research
1
Department of Internal Medicine, Chung-Ang University College of Medicine,
2Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine,
3Department of Internal Medicine, Severance Hospital, Yonsei University College of Medicine, Seoul,
4Department of Internal Medicine, School of Medicine, Kyungpook National University, Daegu,
5Department of Internal Medicine, Pusan National University School of Medicine, Busan,
6Department of Internal Medicine, Chonnam National University Medical School, Gwangju,
7Department of Internal Medicine, Chungnam National University College of Medicine, Daejeon,
8Department of Internal Medicine, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seoul,
9Department of Internal Medicine, Jeju National University School of Medicine, Jeju,
10Department of Internal Medicine, Kosin University Gospel Hospital, Kosin University College of Medicine, Busan,
11Center for Gastric Cancer, National Cancer Center, Goyang,
12Department of Internal Medicine, Chungbuk National University Hospital, Chungbuk National University College of Medicine, Cheongju,
13Department of Internal Medicine, Chonbuk National University Hospital, Chonbuk National University Medical School, Jeonju,
14Department of Internal Medicine, Hallym University College of Medicine, Chuncheon,
15Department of Internal Medicine, Dongsan Medical Center, Keimyung University School of Medicine, Daegu,
16
Department of Internal Medicine, Yeouido St. Mary Hospital, College of Medicine, The Catholic University of Korea,
17Department of Internal Medicine and Liver Research Institute, Seoul National University College of Medicine,
18Medical Research Collaborating Center, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, and
19Department of Prevention and Management, Inha University Hospital, Inha University School of Medicine, Incheon, Korea
Correspondence to: Jae Gyu Kim
aand Jae J. Kim
ba
Department of Internal Medicine, Chung-Ang University College of Medicine, 102 Heukseok-ro, Dongjak-gu, Seoul 06973, Korea Tel: +82-2-6299-3147, Fax: +82-2-749-9150, E-mail: [email protected]
b