접수일: 2012년 10월 7일, 게재승인일: 2012년 11월 9일 책임저자: 원선재, 서울시 영등포구 63로 10 (여의도동)
150-713, 가톨릭대학교 의과대학 여의도성모병원
재활의학과
Tel: 02-3779-1064, Fax: 02-786-4509 E-mail: [email protected]
척추부위에서의 초음파 가이드 중재술
가톨릭대학교 의과대학 여의도성모병원 재활의학과
원 선 재
Ultrasound-Guided Intervention in Axial Structures
Sun Jae Won, M.D.
Department of Rehabilitation Medicine, Yeouido St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea
Based on the advancement of medical engineering technol- ogy, ultrasonography has been used increasingly for the visualization and intervention of axial structures. Especially in the cervical spine, there is a paradigm shift by an ultra- sound-guided intervention. Several ultrasound-guided inter- ventions have been introduced; medial nerve branch blocks or facet block, selective nerve root block, stellate ganglion block, caudal block and sacro-iliac joint injection. This article reviews these ultrasound-guided interventions and de- scribes the techniques involved. (Clinical Pain 2012;11:72- 77)
Key Words: Ultrasound-guided intervention, Spinal intervention, Nerve block, Sacro-iliac joint injection, Stellate ganglion block
서 론
허리 및 목 등의 척추 부위 통증은 매우 흔하고, 그 유병 율도 높은 것으로 알려져 있다.1 척추부 통증의 원인은 매 우 다양하고, 그에 따른 치료도 물리치료, 약물치료와 같은 보존적인 치료에서부터 수술적인 치료에 이르기 까지 다양 한 방법으로 이루어지고 있다. 이 중 척추부위에 시행되는 대표적인 중재적 시술법으로는 경막 외 스테로이드 주입술 (epidural steroid Injection), 내측 신경차단술 또는 후관절 강 내 주사시술(medial nerve branch blocks and facet joint injection)이 대표적이며, 이외에도 환추후두관절(atlanto-
occipital joint), 환추관절(atlanto-axial joint), 천장관절 (sacro-iliac joint) 등의 주사법이 시행되고 있는데,2-4 이들 중재술은 대부분 X선 투시법(fluoroscopy)을 이용한 방법 들이다. X선 투시법은 혈관을 영상화할 수 없기 때문에, 이 를 이용한 시술은 조영제를 주사하기 전에는 혈관 내 주사 를 감지할 수 없다는 단점이 있다. 이로 인해 신경근 차단 술, 환추관절 주사법의 경우 합병증의 발생이 보고되고 있 으며,5-7 숙련된 시술자에 의해 주의 깊게 시술되도록 권고 하고 있다.8
최근 의공학의 발달로 초음파기기의 해상도가 좋아지면 서 각종 척추부 질환에서 초음파를 이용한 시술법들이 소 개되고 있다.9-13 기존의 X선 투시법을 이용한 중재술은 시 술 중에 발생할 수 있는 혈관 내 주사를 ‘감지’할 수 있는 반면, 초음파가이드 중재술은 혈관 내 주사를 ‘예방’할 수 있다는 장점이 있다.14,15 이외에도 초음파를 이용한 시술은 방사선 노출이 없으며, 상대적으로 적은 공간 및 인력으로 시행이 가능하다는 장점이 있다.16 그러나 척추부위에서 초 음파가이드 주사법은 2000년대 이후부터 본격적으로 소개 되기 시작하여, 기존에 보고된 연구의 수는 X선 투시법을 이용한 중재술에 비해 많지 않으며, 초음파 가이드 하에서 주사바늘의 끝을 목표한 곳에 정확하게 위치시켰는지 여부 에 대한 연구나,9,11-13,17-27 기존의 X선 투시법을 이용한 중 재술과 효과를 비교한 임상연구가 대부분이다.28-30
이 글에서는 이들 연구를 바탕으로 지금까지 소개된 척 추부위 초음파가이드 주사법 들 중에 대표적인 것들을 소 개하고자 한다.
본 론
1. 경추부 내측 신경차단술 또는 후관절강 내 주사법 (Cervical medial bundle branch block or facet block)
경추부 후관절은 경추의 위측 관절돌기(superior articu- lar process)와 아래측 관절돌기(inferior articular process)가 만나 이루는 관절로 그 관절면은 꼬리쪽으로 45o 정도 기울 어져 있다. 각각의 관절은 섬유피막(fibrous capsule)과 활 액막(synovial membrane)으로 둘러싸여 있으며, 초음파를 통해 관절의 병변을 확인할 수 있는 경우도 있다. 경추성
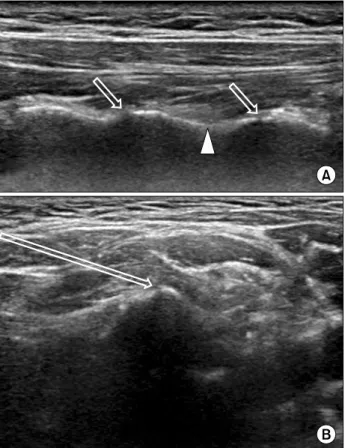
Fig. 1. Ultrasound-guided cervical medial bundle branch block or facet block. (A) Posterior approach using longitudinal scan.
The saw sign is clearly visualized, which means the facet joint (hollow arrow). The target point of medial bundle branch block is the point between saw signs (arrowhead). (B) Lateral approach using axial scan. The facet joint line and the direction of the nee- dle insertion are visualized (hollow arrow).
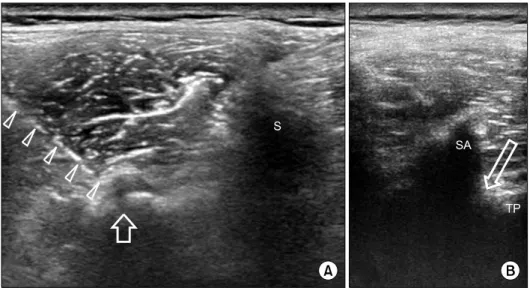
Fig. 2. Cervical selective nerve root block. The target point is the space between nerve root and posterior tubercle (dotted ar- row). The small radicular artery (white arrow) and vertebral ar- tery are visualized with Doppler mode. C7: C7 root, PT: Post- erior tubercle, VA: Vertebral artery.
두통(cervicogenic headache)이나 만성적인 목의 통증, 사고 로 인한 편타성 손상(whiplash injury)으로 인한 통증 등의 원인이 될 수 있다. 이들 통증에서 후관절강 내 스테로이드 주사의 효과는 아직까지 논란이 있으며,31,32 내측 신경차단 술이 표준 치료로 합당하다는 의견도 있다.33,34 후관절 혹은 내측 신경에 대한 초음파가이드 주사는 전산화단층촬영 (computed tomography)이나 X선 투시법을 이용하여 검증 된 연구가 있으며, 정확하게 바늘의 끝을 위치시킬 수 있는 것으로 보고되고 있다.24,35,36
이들에 대한 초음파 가이드 주사는 외측접근법(lateral approach)과 후방접근법(posterior approach)으로 시행할 수 있다(Fig. 1). 후방접근법의 경우 복와위로 환자를 엎드리 게 한 후 고해상도 직선형 탐촉자를 이용하여 위측관절돌 기와 아래측 관절돌기가 만나서 이루는 특징적인 톱니 모 양(saw sign)을 관찰한다. 이를 기준으로 주사하고자 하는
후관절 혹은 내측 신경에 주사를 시행한다. Zhou 등은 경추 성 두통에서 0.25% 부피바케인(bupivacaine)과 스테로이드 (betamethasone 3 mg)를 섞어서 1 ml를 주사하여 90.3%의 환자에서 50% 이상의 통증의 감소를 보였다고 보고하였 다.32
2. 경추부 선택적 신경근 차단술(Cervical selective nerve root block)
경추부 선택적 신경근 차단술은 2005년 Galiano 등에 의 해 처음 그 가능성이 소개되었으며,9 Narouze 등이 2009년 X선 투시법을 이용한 타당성 연구를 통해 구체적인 술기를 보고한 이래,11 이후 경추부 선택적 신경근 차단술은 Naro- uze 등이 제시한 방법을 인용하여 시행되고 있다.30,37 경추 부 신경근병증에 합당한 방사성 통증을 보이는 경우 이 시 술을 시행해 볼 수 있다. 환자는 앙와위 혹은 병변측이 위로 오도록 옆으로 누운 자세에서 목표로 하는 신경근과 경추 의 후결절(posterior tubercle)의 사이 지점을 목표로 주사를 시행한다(Fig. 2). 목표로 하는 신경근을 결정할 때에는 제6 번 경추의 전결절(anterior tubercle)이 매우 뚜렷이 관찰되 나 제7번 경추의 전결절은 관찰할 수 없는 것을 이용하는 방법이 가장 많이 제시되고 있다.30,38 대개 22 G 스파이날 니들(spinal needle)을 이용하여 4 ml 이내에서 주사액을 주 입하는 것을 권장한다. 경추부 중재술의 경우 주변에 중요 한 혈관 및 구조물이 많기 때문에 바늘의 위치와 경로를 정확히 파악할 수 있도록 평면 정렬 접근법(in plane ap- proach)을 이용하는 것이 좋다. 또한 주사액을 주입할 때 바늘 끝의 위치가 흔들리지 않도록 주의하여야 하며, 수액 선(line extension)을 이용하여 보조자가 주사액을 주입하는
Fig. 3. Lumbar facet block and medial bundle branch block. (A) The facet joint line is visualized with synovial capsule bulging (hol- low arrow). The needle is inserted into the facet joint (arrowheads).
(B) The target point of the medial bundle branch block is the angle between the superior articular pro- cess and transverse process. S: Spi- nous process, SA: Superior articu- lar process, TP: Transverse process.
것도 도움이 된다. Jee 등은 120명의 환자에서 무작위배정, 맹검연구를 통해 초음파가이드 주사법을 이용해 3 ml의 주 사액(2 ml dexamethasone+1 ml 0.5% lidocaine)을 주사한 것과 X선 투시법을 이용한 주사법의 효과를 비교하였는데, 12주까지 추적관찰한 결과 기존의 X선 투시법을 이용한 주 사법과 그 효과에서 차이가 없었다고 보고하였다.30 또한 기존에 Narouze 등은 초음파 가이드 중재술로 선택적 신경 근차단술을 시행할 경우 약물이 경막 외까지는 올라가지 않으며 척수후근신경(dorsal root ganglion)까지만 퍼지기 때문에 경추간공 경막외차단술(transforaminal epidural block)이라기보다는 선택적 신경근차단술(selective nerve root block)이라는 용어가 합당하다고 하였으나,11 이 연구 에서는 시술 후 경추부 경막 외까지 조영제가 퍼지는 것을 확인하여 이전의 연구들과는 상반된 결과를 보고하였다.
3. 성상신경절차단술(Stellate ganglion block)
초음파가이드 성상신경절 차단술은 아무런 가이드 없이 해부학적인 표지만을 이용하여 시행하는 경우와 비교해, 바늘이 식도를 뚫거나, 경동맥, 척수동맥 및 전척수동맥에 주사하는 경우를 피할 수 있어 안전하다.39-41 제6경추의 전 결절(anterior tubercle)과 경동맥 사이로 척추전근막(pre- vertebral fascia)을 목표로 하여 외측에서 평면 정렬 접근법 으로 바늘을 삽입한다. 탐촉자를 세게 압박할 경우 경정맥 이 압박되어 보이지 않게 되므로 시술 중에 탐촉자의 압력 을 주지 않고 목의 구조물을 관찰하여, 경정맥의 위치를 확 인하는 것이 필요하다. 대개 5 ml의 국소마취제를 주사하 나,41 일부 연구에서는 2 ml로도 충분하다고 보고하기도 하 였다.40
4. 요추부 내측 신경차단술 또는 후관절강내 주사법 (Lumbar medial bundle branch block or facet block)
경추부와 마찬가지로 요추부 내측 신경차단술 또는 후관 절강 내 주사법도 주로 전산화단층촬영이 나 X선 투시법을 이용하여 그 유효성 연구가 이뤄져 왔으며, 89∼95% 전후 의 정확도를 보이는 것으로 보고된 바 있다.13,19,22,27 요추부 는 경추부에 비하여 목표로 하는 구조물이 더 깊이 있기 때문에 대개 곡선형 탐촉자를 이용하며, 특히 체질량지수 (body mass index)가 30 이상인 비만군에서는 그 정확도가 62%까지 떨어지는 것으로 보고된 바 있다.42 체형이 날씬 한 환자에서는 요추 4-5번, 요추 5번-천추 1번간 후관절의 경우 대개 직선형 탐촉자로도 시술이 가능하다(Fig. 3). 시 술할 척추의 위치를 확인하기 위해서는 천골에서부터 탐촉 자를 머리쪽으로 이동시키면서 나타나는 후관절의 개수를 세거나, Jung 등이 제시한 대로 초음파의 종단면 영상 (longitudinal scan)을 이용하여 시술할 척추의 위치를 확인 하는 것이 유용하다.23 국소마취제(1∼2% lidocaine)만 사 용하거나, 혹은 스테로이드(triamcinolone 10∼40 mg)를 섞어서 1∼2 ml의 주사액을 주입한다.13,23,28
5. 미추 경막외 신경차단술(Caudal epidural block) 초음파 가이드 미추 경막외 신경차단술은 Chen 등에 의 해 소개된 방법이 주로 인용되어 사용되고 있다.20 초음파 를 횡단면 영상(axial scan)으로 양 천골각(sacral cornua)이 U자 형태로 보이는 지점에서 종단면(longitudinal scan)으 로 탐촉자를 회전시켜 천추-미추인대(sacro-coccygeal liga- ment)를 확인한다. 이 상태에서 평면 정렬 접근법으로 바늘
을 삽입한다.20 주사액은 X선 투시법을 이용한 경우와 동일 하게 국소마취제와 스테로이드를 섞어서 10∼20 ml를 주 입한다. 주사액을 주입하기 전에 항상 혈관 내 주사를 피하 기 위해 도플러 모드를 이용하여 재확인하는 것이 필요하 다.43
6. 천장관절 주사법(Sacro-iliac joint injection) 천장관절주사법은 천장관절의 하부 1/3지점에서 대개 시행하며, 이 지점에서 관절면은 중앙의 극돌기(spinal pro- cess)에서 약 5 cm 정도 외측에 존재하게 된다. 초음파 가이 드 주사를 시행했을 때 성공률은 76.7∼80%로 보고된 바
있다.12,29 Klauser 등은 10명의 환자에서 1.5 ml의 주사액
(40 mg triamcinolone+2% mepivacaine 0.5 ml)을 주입하 여 시술이 성공한 모든 환자에서 통증의 호전이 있었으며, 특히 제2 엉치뼈구멍(sacral foramen) 주위에서 시행하는 것이 더 위쪽에서 시행하는 것보다 성공률이 높다고 보고 하였다.29
결 론
초음파 가이드 주사법은 시술자가 주사하고자 하는 부위 의 초음파 영상을 정확히 구현할 수 있고, 시술 중 바늘을 정확히 관찰할 수 있어야 한다. 시술 중 주사액을 주입하면 서 초음파를 이용하여 바늘 끝에서 주사액이 조직 내로 퍼 지는 것을 관찰해야 한다. 주사액이 조직 내로 퍼지는 것이 제대로 관찰되지 않는 경우 정맥 내 주사의 가능성이 있으 므로 바늘의 끝을 적절히 재위치시킬 필요가 있다. 경추부 중재술의 경우 초음파를 이용하여 신경근, 혈관을 포함한 대부분의 구조물의 관찰이 가능하여,38 X선 투시법을 이용 한 중재술에서 초음파가이드를 이용한 중재술로의 패러다 임의 변화가 일어나고 있다.15 그러나, 아직까지 개별적인 시술에서 충분한 임상연구가 부족하고 시술법의 장단점이 존재하여 X선 투시법을 완전히 대체하기는 어렵다. 향후 지속적인 연구과 관심이 필요하다.
참 고 문 헌
1. Deyo RA, Mirza SK, Martin BI. Back pain prevalence and visit rates: estimates from U.S. national surveys, 2002.
Spine (Phila Pa 1976) 2006; 31: 2724-2727
2. Jasper JF. Lumbar retrodiscal transforaminal injection. Pain Physician 2007; 10: 501-510
3. Kang SS, Hwang BM, Son HJ, Cheong IY, Lee SJ, Lee SH, et al. The dosages of corticosteroid in transforaminal epidural steroid injections for lumbar radicular pain due to a herniated disc. Pain Physician 2011; 14: 361-370
4. Windsor RE, Storm S, Sugar R, Nagula D. Cervical trans- foraminal injection: review of the literature, complications, and a suggested technique. Pain Physician 2003; 6: 457-465 5. Edlow BL, Wainger BJ, Frosch MP, Copen WA, Rathmell
JP, Rost NS. Posterior circulation stroke after C1-C2 intra- articular facet steroid injection: evidence for diffuse micro- vascular injury. Anesthesiology 2010; 112: 1532-1535 6. Goodman BS, Bayazitoglu M, Mallempati S, Noble BR,
Geffen JF. Dural puncture and subdural injection: a compli- cation of lumbar transforaminal epidural injections. Pain Physician 2007; 10: 697-705
7. Karaman H, Kavak GO, Tufek A, Yldrm ZB. The compli- cations of transforaminal lumbar epidural steroid injections.
Spine (Phila Pa 1976) 2011; 36: E819-E824
8. De Cordoba JL, Bernal J. Cervical transforaminal blocks should not be attempted by anyone without extensive docu- mented experience in fluoroscopically guided injections.
Anesthesiology 2004; 100: 1323-1324; author reply 4 9. Galiano K, Obwegeser AA, Bodner G, Freund MC, Gruber
H, Maurer H, et al. Ultrasound-guided periradicular in- jections in the middle to lower cervical spine: an imaging study of a new approach. Reg Anesth Pain Med 2005; 30:
391-396
10. Gofeld M. Ultrasound-guided lumbar transforaminal in- jections: feasibility and validation study. Spine (Phila Pa 1976) 2012; 37: 808-812
11. Narouze SN, Vydyanathan A, Kapural L, Sessler DI, Mekhail N. Ultrasound-guided cervical selective nerve root block: a fluoroscopy-controlled feasibility study. Reg Ane- sth Pain Med 2009; 34: 343-348
12. Pekkafahli MZ, Kiralp MZ, Basekim CC, Silit E, Mutlu H, Ozturk E, et al. Sacroiliac joint injections performed with sonographic guidance. J Ultrasound Medicine 2003; 22:
553-559
13. Shim JK, Moon JC, Yoon KB, Kim WO, Yoon DM. Ultra- sound-guided lumbar medial-branch block: a clinical study with fluoroscopy control. Reg Anesth Pain Med 2006; 31:
451-454
14. Narouze SN. Ultrasound-guided cervical periradicular in- jection: cautious optimism. Reg Anesth Pain Med 2006; 31:
87; author reply 87-88
15. Narouze SN. Ultrasound-guided cervical spine injections:
ultrasound “prevents” whereas contrast fluoroscopy “detects”
intravascular injections. Reg Anesth Pain Med 2012; 37:
127-130
16. Galiano K, Obwegeser AA, Walch C, Schatzer R, Ploner F, Gruber H. Ultrasound-guided versus computed tomog- raphy-controlled facet joint injections in the lumbar spine:
a prospective randomized clinical trial. Reg Anesth Pain Med 2007; 32: 317-322
17. Loizides A, Gruber H, Peer S, Brenner E, Galiano K, Obernauer J. A new simplified sonographic approach for pararadicular injections in the lumbar spine: a CT-con- trolled cadaver study. AJNR Am J Neuroradiol 2011; 32:
828-831
18. Loizides A, Gruber H, Peer S, Galiano K, Bale R, Oberna- uer J. Ultrasound guided versus CT-controlled pararadicular injections in the lumbar spine: a prospective randomized clinical trial. AJNR Am J Neuroradiol 2013 [in press]
19. Galiano K, Obwegeser AA, Bodner G, Freund M, Maurer H, Kamelger FS, et al. Ultrasound guidance for facet joint injections in the lumbar spine: a computed tomography- controlled feasibility study. Anesth Analg 2005; 101: 579- 583
20. Chen CP, Tang SF, Hsu TC, Tsai WC, Liu HP, Chen MJ, et al. Ultrasound guidance in caudal epidural needle place- ment. Anesthesiology 2004; 101: 181-184
21. Chin KJ, Karmakar MK, Peng P. Ultrasonography of the adult thoracic and lumbar spine for central neuraxial blockade. Anesthesiology 2011; 114: 1459-1485
22. Greher M, Scharbert G, Kamolz LP, Beck H, Gustorff B, Kirchmair L, et al. Ultrasound-guided lumbar facet nerve block: a sonoanatomic study of a new methodologic approach. Anesthesiology. 2004; 100: 1242-1248
23. Jung H, Jeon S, Ahn S, Kim M, Choi Y. The validation of ultrasound-guided lumbar facet nerve blocks as con- firmed by fluoroscopy. Asian Spine J 2012; 6: 163-167 24. Galiano K, Obwegeser AA, Bodner G, Freund MC, Gruber
H, Maurer H, et al. Ultrasound-guided facet joint injections in the middle to lower cervical spine: a CT-controlled so- noanatomic study. Clin J Pain 2006; 22: 538-543 25. Loizides A, Obernauer J, Peer S, Bale R, Galiano K,
Gruber H. Ultrasound-guided injections in the middle and lower cervical spine. Med ultrason 2012; 14: 235-238 26. Galiano K, Obwegeser AA, Bale R, Harlander C, Schatzer
R, Schocke M, et al. Ultrasound-guided and CT-navi- gation-assisted periradicular and facet joint injections in the lumbar and cervical spine: a new teaching tool to recognize the sonoanatomic pattern. Reg Anesth Pain Med 2007; 32:
254-257
27. Gofeld M, Bristow SJ, Chiu S. Ultrasound-guided injection of lumbar zygapophyseal joints: an anatomic study with fluoroscopy validation. Reg Anesth Pain Med 2012; 37:
228-231
28. Yun DH, Kim HS, Yoo SD, Kim DH, Chon JM, Choi SH, et al. Efficacy of ultrasonography-guided injections in pa- tients with facet syndrome of the low lumbar spine. Ann Rehabil Med 2012; 36: 66-71
29. Klauser A, De Zordo T, Feuchtner G, Sogner P, Schirmer M, Gruber J, et al. Feasibility of ultrasound-guided sacroil-
iac joint injection considering sonoanatomic landmarks at two different levels in cadavers and patients. Arthritis Rhum 2008; 59: 1618-1624
30. Jee H, Lee JH, Kim J, Park KD, Lee WY, Park Y.
Ultrasound-guided selective nerve root block versus fluoro- scopy-guided transforaminal block for the treatment of rad- icular pain in the lower cervical spine: A randomized, blinded, controlled study. Skeletal Radiol 2013 [in press]
31. Carragee EJ, Hurwitz EL, Cheng I, Carroll LJ, Nordin M, Guzman J, et al. Treatment of neck pain: injections and sur- gical interventions: results of the Bone and Joint Decade 2000-2010 task force on neck pain and its associated disorders. Spine (Phila Pa 1976). 2008; 33: S153-169 32. Zhou L, Hud-Shakoor Z, Hennessey C, Ashkenazi A.
Upper cervical facet joint and spinal rami blocks for the treatment of cervicogenic headache. Headache 2010; 50:
657-663
33. Barnsley L, Bogduk N. Medial branch blocks are specific for the diagnosis of cervical zygapophyseal joint pain. Reg Anesth 1993; 18: 343-350
34. Narouze SN. Atlas of Ultrasound-guided procedures in in- terventional pain management. New York: Springer Sci- ence Business Media; 2010
35. Siegenthaler A, Mlekusch S, Trelle S, Schliessbach J, Curatolo M, Eichenberger U. Accuracy of ultrasound-guid- ed nerve blocks of the cervical zygapophysial joints. Ane- sthesiology 2012; 117: 347-352
36. Finlayson RJ, Gupta G, Alhujairi M, Dugani S, Tran de QH. Cervical medial branch block: a novel technique using ultrasound guidance. Reg Anesth Pain Med 2012; 37:
219-223
37. Yamauchi M, Suzuki D, Niiya T, Honma H, Tachibana N, Watanabe A, et al. Ultrasound-guided cervical nerve root block: spread of solution and clinical effect. Pain Med 2011; 12: 1190-1195
38. Won SJ, Kim BJ, Park KS, Kim SH, Yoon JS. Measure- ment of cross-sectional area of cervical roots and brachial plexus trunks. Muscle Nerve 2012; 46: 711-716
39. Siegenthaler A, Mlekusch S, Schliessbach J, Curatolo M, Eichenberger U. Ultrasound imaging to estimate risk of esophageal and vascular puncture after conventional stellate ganglion block. Reg Anesth Pain Med 2012; 37: 224-227 40. Lee MH, Kim KY, Song JH, Jung HJ, Lim HK, Lee DI,
et al. Minimal volume of local anesthetic required for an ultrasound-guided SGB. Pain Med 2013 [in press]
41. Narouze S, Vydyanathan A, Patel N. Ultrasound-guided stellate ganglion block successfully prevented esophageal puncture. Pain Physician 2007; 10: 747-752
42. Rauch S, Kasuya Y, Turan A, Neamtu A, Vinayakan A, Sessler DI. Ultrasound-guided lumbar medial branch block
in obese patients: a fluoroscopically confirmed clinical fea- sibility study. Reg Anesth Pain Med 2009; 34: 340-342 43. Yoon JS, Sim KH, Kim SJ, Kim WS, Koh SB, Kim BJ.
The feasibility of color Doppler ultrasonography for caudal epidural steroid injection. Pain 2005; 118: 210-214