751
술 전 예측 인자
The Preoperative Factors Predicting a Positive Frozen Section during Radical Prostatectomy for Prostate Cancer
Myungsun Shim, Changhee Yoo1, In Gab Jeong, Choung-Soo Kim From the Department of Urology, Asan Medical Center, University of Ulsan College of Medicine, 1Hallym Sacred Heart Hospital, University of Hallym College of Medicine, Seoul, Korea
Purpose: The purpose of this study was to identify the preoperative factors that predict a positive frozen section during radical prostatectomy for prostate cancer.
Materials and Methods: We retrospectively analyzed preoperative pro- state-specific antigen (PSA), prostate volume, Gleason score, the number or percent (%) of cancer-positive cores from prostate biopsy, and the clinical stage of 364 patients who underwent radical prostatectomy between 1993 and 2007. We compared these parameters between patients who had positive frozen sections in specimens from the urethra or bladder neck with those who had negative frozen sections.
Results: The PSA and Gleason score were significantly higher and prostate volume was significantly smaller in patients with positive frozen sections in the urethra than in patients with negative frozen sections. The results were the same for the bladder neck. In multivariate analysis, PSA was the only independent predictor for positive frozen sections at the bladder neck, and the cutoff value was 8.71 ng/ml.
Conclusions: Preoperative PSA may be a potent factor for predicting posi- tive frozen sections during radical prostatectomy, especially in the bladder neck. Therefore, it may be beneficial to prepare frozen sections of the bladder neck during the operation to reduce the positive resection margin when PSA is higher than 8.7 ng/ml. (Korean J Urol 2009;50:751-756)
Key Words: Prostatectomy, Frozen sections, Prostatic neoplasms, Prostate- specific antigen
Korean Journal of Urology Vol. 50 No. 8: 751-756, August 2009
DOI: 10.4111/kju.2009.50.8.751
울산대학교 의과대학 서울아산병원
비뇨기과학교실, 1한림대학교
의과대학 비뇨기과학교실
심명선ㆍ유창희1ㆍ정인갑ㆍ김청수
Received:March 19, 2009 Accepted:June 30, 2009
Correspondence to: Choung-Soo Kim Department of Urology, Asan Medical Center, University of Ulsan College of Medicine, 388-1, Pungnap-dong, Songpa-gu, Seoul 138-736, Korea
TEL: 02-3010-3734 FAX: 02-477-8928
E-mail: [email protected] This study was supported by a grant of the Korea Healthcare technology R&D project, Ministry for Health, Welfare & family Affairs, Republic of Korea (A062254).
Ⓒ The Korean Urological Association, 2009
서 론
근치적 전립선적출술을 시행하는데 가장 중요한 목표는 암의 완전한 제거이며 이는 종양의 범위와 술기에 많은 영 향을 받게 된다.1,2 영구 조직검사에서 절단면 양성인 경우 에는 암의 완전한 제거가 이루어지지 않았다는 것을 의미 하며 이는 전립선암의 생화학적 재발 위험성을 높이고, 향 후 호르몬 치료나 방사선 치료 등 추가적인 치료를 필요로 할 가능성이 높아지게 된다.3,4 이전의 여러 연구에서 술 전
전립선특이항원 (prostate-specific antigen; PSA), 임상적 병 기, Gleason 점수 그리고 병리학적 병기 등 전립선암의 재발 에 영향을 줄 수 있는 다른 인자들을 고려해서 분석한 결과 절단면 양성은 생화학적 재발과 관련이 있다고 보고되고 있다.4-9
PSA 선별 검사에 따른 전립선암의 조기 진단 및 이에 따 른 국소 전립선암 비율의 증가로 인하여 근치적 전립선적 출술 후 영구 조직검사에서의 절단면 양성률은 크게 낮아 졌으나, 최근의 연구에 의하면 절단면 양성률이 여전히 41%까지 보고되는 것으로 나타났다.10,11 따라서 영구 조직
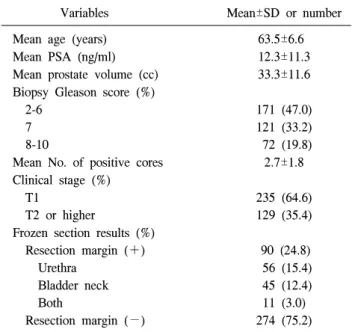
Table 1. Preoperative characteristics and results of frozen sections
Variables Mean±SD or number
Mean age (years) 63.5±6.6
Mean PSA (ng/ml) 12.3±11.3
Mean prostate volume (cc) 33.3±11.6 Biopsy Gleason score (%)
2-6 7 8-10
171 (47.0) 121 (33.2) 72 (19.8) Mean No. of positive cores 2.7±1.8 Clinical stage (%)
T1
T2 or higher
235 (64.6) 129 (35.4) Frozen section results (%)
Resection margin (+) Urethra
Bladder neck Both
Resection margin (−)
90 (24.8) 56 (15.4) 45 (12.4) 11 (3.0) 274 (75.2) SD: standard deviation, PSA: prostate-specific antigen 검사에서의 절단면 양성률을 줄이기 위한 여러 방법이 제
기되고 있으며, 여기에는 전립선 조직검사를 시행하는 PSA 절단치를 낮추는 방법,12 근치적 전립선적출술 시행 시 신경 혈관다발을 보존할 지 여부를 결정하기 위한 알고리즘을 사용하는 방법,13 그리고 수술 중 동결절편검사를 시행하는
방법1,2,14 등이 있을 수 있다. 특히 동결절편검사에서 양성인
경우 해당 부위에서 음성이 될 때까지 추가적인 절제를 시 행하게 되며,15,16 이는 영구 조직검사에서 절단면 양성률을 줄일 수 있다.1,2 그러나 시간, 비용 등을 고려하면 현실적으 로 모든 환자에 대해서 동결절편검사를 시행할 수 없으므 로, 여러 가지 술 전 인자를 고려하여 동결절편검사에서 양 성일 가능성이 높은 경우에 한하여 선택적으로 시행하는 것이 적절할 것으로 생각한다. 본 연구에서는 여러 술 전 인자들 중 동결절편검사에서 양성일 가능성을 예측할 수 있는 인자를 찾아보고자 하였다.
대상 및 방법
1993년 9월부터 2007년 6월까지 본원에서 단일 술자에 의해 근치적 전립선적출술을 시행 받은 364명의 환자를 대 상으로 후향적으로 조사하였다. 수술 전 호르몬 치료 또는 방사선 치료를 받은 환자는 제외하였다.
PSA가 4.0 ng/ml보다 높게 측정되거나 직장수지검사 (di- gital rectal examination; DRE) 또는 경직장초음파 (trans- rectal ultrasound; TRUS)에서 이상 소견을 보이는 경우에 전 립선 조직검사를 시행하였다. 전립선 조직검사는 4-12 부위 에서 시행했고, 2004년 3월 이후부터는 모든 환자에서 TRUS 유도 하에 12 부위에서 조직검사를 시행하였으며, 이 는 전체 환자의 55.2% (201/364)를 차지하였다. 수술 방법은 후치골 근치적 전립선적출술 (retropubic radical prostatec- tomy; RRP)과 제한 림프절절제술을 시행하였고, 모든 환자 에서 술 중 요도 및 방광 경부에서 동결절편검사를 시행하 였다. 동결절편검사에서 양성인 환자는 음성이 나올 때까 지 추가로 절제하였다.
환자들의 평균 나이는 63.5세였고, 평균 PSA는 12.3 ng/ml, TRUS에서 전립선의 평균 크기는 33.3 cc였으며, 진 단 시 임상적 병기가 T2 이상인 경우는 129명 (35.4%)이었 다. 전체 364명의 환자 중에서 수술 중 시행한 동결절편검 사에서 양성을 보인 환자의 수는 90명 (24.8%)이었고, 이들 중 요도절단면에서 양성인 경우가 56명 (15.4%), 방광경부 에서 양성인 경우가 45명 (12.4%)이었으며, 양쪽 모두에서 양성인 경우가 11명 (3.0%)이었다 (Table 1).
대상 환자들을 동결절편검사에서 절제면 양성인 군과 음 성인 군으로 나누어서 각 군의 술 전 PSA, TRUS에서 전립
선의 크기, 전립선 조직검사에서 Gleason score, 조직검사에 서 양성 core 개수 및 전체 core 중 양성 core의 비율 (%), 그리고 임상적 병기를 비교하였다. 또한 술자의 수술 술기 에 대한 숙련도에 따라 절단면의 양성률이 다를 수 있으므 로 일반적으로 근치적 전립선적출술의 종양학적 성적이 안 정화된다고 알려진 250례를 기준으로 그 이전과 이후로 나 누어 변수로 추가하였다.17 이들 환자를 요도절단면 또는 방 광 경부에서 동결절편검사가 양성인 환자군, 요도절단면에 서만 양성인 환자군, 그리고 방광 경부에서만 양성인 환자 군으로 나누어 이들 부위에서 동결절편검사가 음성인 환자 군과 비교하여 분석하였다.
동결절편검사에서 양성인 환자군과 음성인 환자군에서 의 술 전 PSA, TRUS에서 전립선 크기와 양성검체의 개수 또는 비율 (%)은 Student’s t-test를, 전립선 생검에서의 Gleason 점수와 임상적 병기는 chi-square test를 사용하여 비교하였 다. 또한 동결절편검사에서 양성으로 나온 경우를 예측할 수 있는 술 전 인자를 알아보기 위해 다중 로지스틱 회귀분 석 (multiple logistic regression analysis)을 시행하였다. 통계 분석은 Windows용 SPSS version 12.0를 이용하였고, p값이 0.05 미만일 때 통계적으로 유의한 것으로 판정하였다.
결 과
동결절편검사에서 양성인 환자군과 음성인 환자군을 비 교하여 보았을 때, 술 전 PSA와 조직 검사의 Gleason 점수
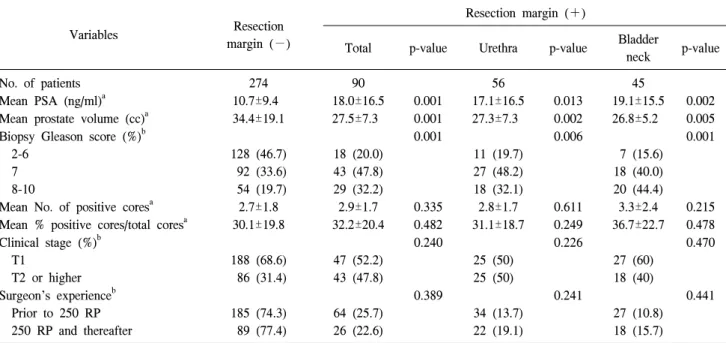
Table 2. Comparative analysis of preoperative variables between subjects according to the results of frozen sections
Variables Resection
margin (−)
Resection margin (+)
Total p-value Urethra p-value Bladder
neck p-value
No. of patients 274 90 56 45
Mean PSA (ng/ml)a 10.7±9.4 18.0±16.5 0.001 17.1±16.5 0.013 19.1±15.5 0.002
Mean prostate volume (cc)a 34.4±19.1 27.5±7.3 0.001 27.3±7.3 0.002 26.8±5.2 0.005
Biopsy Gleason score (%)b 2-6
7 8-10
128 (46.7) 92 (33.6) 54 (19.7)
18 (20.0) 43 (47.8) 29 (32.2)
0.001
11 (19.7) 27 (48.2) 18 (32.1)
0.006
7 (15.6) 18 (40.0) 20 (44.4)
0.001
Mean No. of positive coresa 2.7±1.8 2.9±1.7 0.335 2.8±1.7 0.611 3.3±2.4 0.215
Mean % positive cores/total coresa 30.1±19.8 32.2±20.4 0.482 31.1±18.7 0.249 36.7±22.7 0.478 Clinical stage (%)b
T1
T2 or higher
188 (68.6) 86 (31.4)
47 (52.2) 43 (47.8)
0.240
25 (50) 25 (50)
0.226
27 (60) 18 (40)
0.470
Surgeon’s experienceb Prior to 250 RP 250 RP and thereafter
185 (74.3) 89 (77.4)
64 (25.7) 26 (22.6)
0.389
34 (13.7) 22 (19.1)
0.241
27 (10.8) 18 (15.7)
0.441
PSA: prostate-specific antigen, RP: radical prostatectomy, a: PSA, prostate volume, No. of positive cores and % positive cores/total cores were analyzed as continuous variables, b: biopsy Gleason score, clinical stage and surgeon’s experience was analyzed as categorical variables
Table 3. Predictors of a positive frozen section among preoperative variables in binary logistic analysis
Total Urethra Bladder neck
Odds ratio (95% CI) p-value Odds ratio (95% CI) p-value Oddsratio (95% CI) p-value
PSAa 1.040 (1.005-1.077) 0.027 1.033 (0.996-1.071) 0.079 1.059 (1.002-1.118) 0.041
Biopsy Gleason scoreb 2-6
7 1.566 (0.639-3.837) 0.308 2.055 (0.709-5.958) 0.347 0.910 (0.245-3.373) 0.552
8-10 0.844 (0.319-2.232) 0.372 1.313 (0.420-4.102) 0.459 0.449 (0.095-2.132) 0.256
Prostate volumea 0.976 (0.952-1.001) 0.064 0.983 (0.959-1.008) 0.186 0.950 (0.892-1.012) 0.110 CI: confidence interval, PSA: prostate-specific antigen, a: PSA and prostate volume were analyzed as continuous variables, b: biopsy Gleason score was analyzed as categorical variables
는 양성인 환자군에서 유의하게 높았고, TRUS에서의 전립 선 크기는 양성인 환자군에서 유의하게 작았다 (Table 2).
그러나 조직 검사 중 양성 검체의 개수 또는 비율, 진단 시 의 임상적 병기 및 술자의 수술 술기에 대한 숙련도는 유의 한 차이를 보이지 않았다 (Table 2). 이를 양성 부위별로 요 도 절단면과 방광 경부로 나누어서 분석해 보았을 때도 위 와 동일한 결과를 보였다 (Table 2).
술 전 인자들 중 동결절편검사에서 양성 여부를 예측하기 위해서 다변량 분석을 시행한 결과, 술 전 PSA만이 유의한 인자로 나타났다 (p=0.027). 이를 요도절단면과, 방광경부로 분리해서 분석하였을 때, 방광경부에서만 절단면 양성 여 부를 예측할 수 있는 유의한 인자였다 (p=0.041) (Table 3).
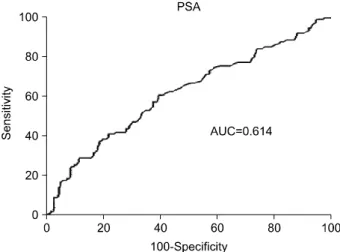
또한 수신자판단특성곡선 (receiver operation characteristic curve; ROC curve)을 이용하여 동결절편검사에서 방광경부 양성 여부를 예측하기 위한 PSA의 절단치 (cut off value)를 구하고자 하였다. 그 결과 민감도와 특이도가 각각 60.9%, 60.5%로 가장 적절한 값은 8.71 ng/ml였고, 이 값에서 동결 절편검사 결과 양성인 환자와 음성인 환자를 가장 잘 분류 해 주는 것으로 나타났다 (AUC=0.614, 95% CI; 0.560-0.666) (Fig. 1).
고 찰
근치적 전립선적출술을 시행 받은 후 발생할 수 있는 전
Fig. 1. ROC curve and AUC of serum PSA predicting a positive frozen section at the bladder neck. ROC: receiver operation characteristic, AUC: area under the curve, PSA: prostate-specific antigen.
립선암의 재발에는 술 전 PSA, 전립선 조직검사에서의 Gleason 점수, 임상적 병기, 병리학적 병기, 그리고 절단면 이 양성인지 여부 등, 여러 가지 인자가 영향을 줄 수 있다 고 알려져 있다.18,19 이들 인자들 중 수술 방법에 영향을 받 는 유일한 인자는 절단면의 양성 여부일 것이다. 실제로 Eastham 등20은 26명의 술자가 1983년부터 2002년까지 시행 한 총 2,639건의 근치적 전립선적출술의 결과를 비교해 보 았을 때, 술자마다 다른 술기가 절단면 양성률에 영향을 줄 수 있는 인자가 될 수 있다고 보고하였다. 따라서 본 연구에 서는 수술 방법 즉, 동결절편검사를 통해 전립선 절단면 양 성률을 줄일 수 있다는 점에 주목하고자 하였다.
지금까지의 연구에 의하면 영구 조직검사에서 전립선 절 단면의 양성률은 6-48%인 것으로 보고되어 있고,10,11,20 본 연구에서는 부위에 관계없이 절단면 양성률은 24.7%였고, 그 중 요도 절단면과 방광경부에서는 각각 15.4%, 12.4%였 다. 이처럼 절단면 양성의 경우는 추가적인 절제가 가능한 요도 절단면과 방광 경부에서 나타나는 경우가 많으며, Pettus 등21은 전립선 첨부에서 절단면 양성인 경우와 그 외 의 부위에서 양성인 경우에서 생화학적 재발률이 각각 21.4%, 26.3%라고 보고하였고, Blute 등22은 병리학적 병기 가 T2 이하인 환자들 중 요도 절단면에서 양성인 경우와 방광 경부에서 양성인 경우에서 전립선암의 5년 무재발 생 존율이 각각 93.1%, 89.4%라고 보고하였다. 그리고 여러 연 구에서 이러한 전립선 절단면 양성인 경우가 수술 후 전립 선암의 예후에 부정적인 영향을 줄 수 있다고 보고하였
다.4,23,24 Swindle 등4의 연구에 의하면 절단면 양성과 생화학
적 재발은 연관 관계가 없다는 보고도 있지만, 이는 여러 가지 다양한 술 후 보조 치료의 사용과 각 연구마다 서로
상이한 통계학적 방법을 적용한 결과이며, 전립선 절단면 양성 여부가 독립적으로 생화학적 재발에 영향을 줄 수 있 다고 하였다. 그러므로 근치적 전립선적출술의 치료 성적 을 향상시키기 위하여 전립선 절단면 양성률을 줄이는 방 법을 연구하는 것이 중요하다고 하겠다. 그리고 병리학적 병기 T2가 T3a보다 생화학적 재발이 적은 편이며 특히 T2 에서 생화학적 재발을 줄이기 위해서는 절단면을 음성으로 유지하는 것이 중요하다.
수술 중 시행하는 동결절편검사는 영구 조직검사에서 절 단면 양성일 확률을 줄이고 종양을 완벽하게 제거하는데 도움이 될 수 있다. 동결절편검사와 영구조직검사의 결과 를 비교한 과거의 연구에 의하면 전립선 첨부에서 동결절 편검사의 민감도와 특이도는 각각 57%, 86%로 그리고 방 광경부 절단면에서는 각각 67%, 90%로 보고되고 있다.2,14 따라서 동결절편검사는 비록 민감도는 높지 않지만 높은 특이도로 인해 영구조직검사의 결과를 예측하는데 많은 도 움을 줄 수 있을 것이다. 또한, Lepor와 Kaci1는 근치적 전립 선적출술을 시행 받는 환자들을 대상으로 임의로 전립선 첨부에 대해 동결절편검사를 시행한 결과 시행하지 않은 군에 비하여 영구 조직검사에서 절단면 양성률을 3.8% 정 도 감소시킬 수 있다고 하였다. 그러므로 수술 중 동결절편 검사를 시행하는 것이 향후 영구 조직검사에서의 절단면 양성률을 낮추는데 유용하다고 할 수 있겠다. 그러나 Tsuboi 등25의 연구에 의하면 수술 중에 전립선 및 주위 조직에서 의심이 가는 부위에 대해 동결절편검사를 시행했을 때, 그 민감도 42%로 낮았으며 의심이 가지 않았던 부위의 영구 조직검사에서 절단면 양성일 수 있으므로 모든 환자에 대 해서 동결절편검사를 시행하는 것은 유용하지 않다고 결론 지었다. 따라서 술자가 의심이 가는 부위에 대해 동결절편 검사를 시행하는 방법은 그 실효성에 의문의 여지가 있고 또한 모든 환자에 대해서 동결절편검사를 시행하는 것은 현실적으로 비용과 시간적인 측면에서 비효율적이므로 수 술 전 여러 가지 인자를 바탕으로 한 동결절편검사를 시행 하는데 필요한 객관적인 지침이 있다면 매우 유용하다고 할 수 있을 것이다.
그러므로 본 연구에서는 동결절편검사에서 양성일 가능 성을 예측할 수 있는 술 전 인자에 대해서 알아보고자 하였 다. 이를 위하여 근치적 전립선적출술을 시행한 환자들을 동결절편검사 양성인 환자군과 음성인 환자군으로 나누어 각 군의 술 전 PSA, TRUS에서의 전립선 크기, 전립선 조직 검사에서의 Gleason 점수, 양성검체의 개수 또는 조직검사 를 시행한 검체에 대한 양성검체의 비율 (%), 그리고 임상 적 병기를 비교해 보았다. 이들 인자는 수술 전 혈액 검사, 신체 검사, 초음파 검사 그리고 조직검사로 비교적 쉽게 알
수 있으므로 위의 결과를 바탕으로 근치적 전립선적출술을 시행할 때, 동결절편검사에서 양성일 가능성이 높은 환자 를 예측하여 이들 환자들에 대해서만 동결절편검사를 시행 한다면 훨씬 경제적이고 효과적일 수 있을 것이다. 또한 보 다 합리적인 결과를 도출하기 위해서는 술자에 따라 수술 중 시행하는 동결절편검사 결과가 다르게 나타날 수 있으 므로 본 연구에서는 단일 술자에 의한 환자만을 대상으로 하였다. 그리고 단일 술자에서도 술기의 숙련도에 따라 그 결과가 달라질 수 있으므로 근치적 전립선적출술에서 종양 학적 성적의 안정화를 위해 필요하다고 알려진 250례를 기 준으로 비교하였으나,17 본 연구에서는 동결절편검사 양성 률에는 영향을 미치지 않았다. 또한 전립선 절제를 시행할 때, 요도 절단면과 방광경부에서 동결절편검사 결과 양성 인 경우 추가적인 절제가 용이하기 때문에 실제 수술에서 활용할 수 있으므로 분석을 이들 부위만으로 제한하였다.
본 연구에서는 술 전 PSA, TRUS에서의 전립선 크기, 그 리고 전립선 조직검사에서의 Gleason 점수가 동결절편검사 양성인 환자와 음성인 환자에서 유의한 차이가 있었다. 특 히 동결절편검사에서 양성인 환자에서 전립선 크기가 작은 것으로 나타났다. Freeland 등26에 의하면 전립선적출술을 받은 환자에서 보다 작은 크기의 전립선은 높은 Gleason 점 수를 가진 경우가 많고 이는 높은 전립선 절단면 양성률, 전립선 피막 침범률, 그리고 향후 전립선암의 생화학적 재 발과 관계가 있다고 보고하였다. 또한 Hong 등27은 전립선 적출술 후 검체의 무게와 전립선암의 전립선 외부 확장, 그 리고 절단면 양성일 확률은 유의하게 반비례 한다고 보고 하였다. 따라서 앞에서 언급한 이들 연구 결과는 동결절편 검사에서 양성인 환자에서 전립선 크기가 작게 나타나는 본 연구의 결과를 뒷받침 한다고 할 수 있다.
다변량 분석에서는 실제로 동결절편검사가 양성일 가능 성을 예측할 수 있는 유의한 인자는 술 전 PSA인 것으로 나타났다. 그러나 이를 부위 별로 나누어 보았을 때, 술 전 PSA는 요도 절단면에서는 의미가 없었으나 방광 경부에서 는 수술 중 동결절편검사를 시행하였을 때 그 결과가 양성 일 가능성이 높았다. 요도 부위에서는 동결절편검사에 결 과가 양성이더라도 요도 괄약근 손상에 의한 요실금 등의 부작용에 대한 우려로 인해 추가적인 절제를 시행하기에 어려운 점이 있다. 그리고 요도 동결절편이 양성인 경우와 음성인 경우를 비교해 보았을 때 생화학적 재발에 큰 차이 가 없다는 보고도 있으므로2 실제 임상적으로는 방광경부 에서의 동결절편검사 시행에 대한 지침을 결정하는 것이 더욱 실용적일 수 있다. 이에 저자들은 방광경부에서의 동 결절편 시행 여부에 대한 지침을 본 연구에서 산출한 PSA 8.71 ng/ml를 바탕으로 하여 8.7 ng/ml로 제시하고자 한다.
따라서 술 전 PSA가 8.7 ng/ml 이상인 경우에 방광경부에서 동결절편검사를 시행하고 양성인 경우에 다시 그 부위를 절제해서 음성으로 전환할 경우, 이는 영구 조직검사에서 의 절단면 양성률을 낮출 수 있을 것으로 기대된다. 그러나 추가적인 절제가 실제로 전립선암의 생화학적 재발을 줄일 수 있는지 확인하기 위해서는 향후 대단위의 전향적 연구 가 필요하다고 하겠다.
결 론
술 전 PSA, TRUS에서의 전립선 크기 그리고 전립선 조 직검사의 Gleason 점수는 동결절편검사 결과에 영향을 줄 수 있다. 이들 중 술 전 PSA는 방광경부에서의 동결절편검 사 양성을 예측할 수 있는 독립적인 인자였다. 따라서 술 전 PSA가 높은 환자, 특히 8.7 ng/ml 이상인 경우에서는 방 광경부에서 동결절편검사를 시행하여 절제 범위를 결정하 는 것이 수술 후 영구 조직검사에서 절단면 양성의 가능성 을 줄이는데 도움이 될 수 있다고 생각한다.
REFERENCES
1. Lepor H, Kaci L. Role of intraoperative biopsies during radical retropubic prostatectomy. Urology 2004;63:499-502
2. Shah O, Melamed J, Lepor H. Analysis of apical soft tissue margins during radical retropubic prostatectomy. J Urol 2001;
165:1943-8
3. Pfitzenmaier J, Pahernik S, Tremmel T, Haferkamp A, Buse S, Hohenfellner M. Positive surgical margins after radical prostatectomy: Do they have an impact on biochemical or clinical progression? BJU Int 2008;102:1413-8
4. Swindle P, Eastham JA, Ohori M, Kattan MW, Wheeler T, Maru N, et al. Do margins matter? The prognostic significance of positive surgical margins in radical prostatectomy speci- mens. J Urol 2005;174:903-7
5. Blute ML, Bergstralh EJ, Iocca A, Scherer B, Zincke H. Use of Gleason score, prostate specific antigen, seminal vesicle and margin status to predict biochemical failure after radical prostatectomy. J Urol 2001;165:119-25
6. Grossfeld GD, Chang JJ, Broering JM, Miller DP, Yu J, Flanders SC, et al. Impact of positive surgical margins on prostate cancer recurrence and the use of secondary cancer treatment: data from the CaPSURE database. J Urol 2000;163:
1171-7
7. Hong JH, Lee HM, Choi HY. The predictors of biochemical recurrence and metastasis following radical perineal pro- statectomy in clinically localized prostate cancer. Korean J Urol 2005;46:1161-7
8. Cho KS, Hong SJ, Chung BH. The impact of positive surgical
margins on biochemical recurrence after radical retropubic prostatectomy. Korean J Urol 2004;45:416-22
9. Kim JB, Kim CS, Park JY. The impact of positive surgical margins and their preoperative predicting factors on bio- chemical failure after radical retropubic prostatectomy. Korean J Urol 2003;44:1262-8
10. Epstein JI. Pathologic assessment of the surgical specimen.
Urol Clin North Am 2001;28:567-94
11. Han M, Partin AW, Pound CR, Epstein JI, Walsh PC.
Long-term biochemical disease-free and cancer-specific sur- vival following anatomic radical retropubic prostatectomy. The 15-year Johns Hopkins experience. Urol Clin North Am 2001;28:555-65
12. Catalona WJ, Smith DS, Ornstein DK. Prostate cancer detec- tion in men with serum PSA concentrations of 2.6 to 4.0 ng/ml and benign prostate examination. Enhancement of specificity with free PSA measurements. JAMA 1997;277:1452-5 13. Shah O, Robbins DA, Melamed J, Lepor H. The New York
University nerve sparing algorithm decreases the rate of posi- tive surgical margins following radical retropubic prostatec- tomy. J Urol 2003;169:2147-52
14. Lepor H, Chan S, Melamed J. The role of bladder neck biopsy in men undergoing radical retropubic prostatectomy with preservation of the bladder neck. J Urol 1998;160:2435-9 15. Cangiano TG, Litwin MS, Naitoh J, Dorey F, deKernion JB.
Intraoperative frozen section monitoring of nerve sparing radical retropubic prostatectomy. J Urol 1999;162:655-8 16. Goharderakhshan RZ, Sudilovsky D, Carroll LA, Grossfeld
GD, Marn R, Carroll PR. Utility of intraoperative frozen sec- tion analysis of surgical margins in region of neurovascular bundles at radical prostatectomy. Urology 2002;59:709-14 17. Vickers AJ, Bianco FJ, Serio AM, Eastham JA, Schrag D,
Klein EA, et al. The surgical learning curve for prostate cancer control after radical prostatectomy. J Natl Cancer Inst 2007;
99:1171-7
18. Hull GW, Rabbani F, Abbas F, Wheeler TM, Kattan MW, Scardino PT. Cancer control with radical prostatectomy alone
in 1,000 consecutive patients. J Urol 2002;167:528-34 19. Kattan MW, Wheeler TM, Scardino PT. Postoperative nomo-
gram for disease recurrence after radical prostatectomy for prostate cancer. J Clin Oncol 1999;17:1499-507
20. Eastham JA, Kattan MW, Riedel E, Begg CB, Wheeler TM, Gerigk C, et al. Variations among individual surgeons in the rate of positive surgical margins in radical prostatectomy specimens. J Urol 2003;170:2292-5
21. Pettus JA, Weight CJ, Thompson CJ, Middleton RG, Stephenson RA. Biochemical failure in men following radical retropubic prostatectomy: impact of surgical margin status and location. J Urol 2004;172:129-32
22. Blute ML, Bostwick DG, Bergstralh EJ, Slezak JM, Martin SK, Amling CL, et al. Anatomic site-specific positive margins in organ-confined prostate cancer and its impact on outcome after radical prostatectomy. Urology 1997;50:733-9
23. Ohori M, Wheeler TM, Kattan MW, Goto Y, Scardino PT.
Prognostic significance of positive surgical margins in radical prostatectomy specimens. J Urol 1995;154:1818-24
24. Wieder JA, Soloway MS. Incidence, etiology, location, prevention and treatment of positive surgical margins after radical prostatectomy for prostate cancer. J Urol 1998;160:
299-315
25. Tsuboi T, Ohori M, Kuroiwa K, Reuter VE, Kattan MW, Eastham JA, et al. Is intraoperative frozen section analysis an efficient way to reduce positive surgical margins? Urology 2005;66:1287-91
26. Freeland SJ, Isaacs WB, Platz EA, Terris MK, Aronson WJ, Amling CL, et al. Prostate size and risk of high-grade, advanced prostate cancer and biochemical progression after radical prostatectomy: a search database study. J Clin Oncol 2005;23:7546-54
27. Hong SK, Yu JH, Han BK, Chang IH, Jeong SJ, Byun SS, et al. Association of prostate size and tumor grade in Korean men with clinically localized prostate cancer. Urology 2007;
70:91-5