증 례
ISSN 2093-9272 일산병원학술지 2017;16(2):221-223Volume 16 Number 2 December 2017
221
악성 기저 멜라닌 세포 암종: 증례 보고
국민건강보험 일산병원 성형외과1, 병리과2
김채민
1, 전여름
1, 기정혜
2, 정 섬
1Malignant Basomelanocytic Tumor: A Case Report
Chae Min Kim
1, Yeo Reum Jeen
1, Jeong Hae Kie
2, Seum Chung
1Department of 1Plastic Surgery and 2Pathology, National Health Insurance Service Ilsan Hospital, Goyang, Korea
Cutaneous combined tumors have been described as having various types of adnexal and/or neuroendocrine differentiation, however, combined tumors composed of keratinocytes and melanocytes are extremely rare. We describe a malignant cutaneous neoplasm with combined phenotypical features of basal cell carcinoma and malignant melanoma, also known as a malignant basomelanocytic tumor. This is the first report of a combined-type malignant basomelanocytic tumor in an Asian patient.
Key Words: Malignant basomelanocytic tumor, Malignant melanoma, Basal cell carcinoma
책임저자: 정 섬
10444 경기도 고양시 일산동구 일산로 100 국민건강보험 일산병원 성형외과
전화 : (031)900-3507-0560, 팩스 : (031)900-3507-0343 E-mail :[email protected]
Fig. 1. Gross appearance. The tumor was 3.5×2.5 cm sized, pig- mented and protruded from the patient's left thigh.
INTRODUCTION
Cutaneous combined tumors exhibit various types of adne- xal and/or neuroendocrine differentiation. According to Boyd et al.,1 basal cell carcinoma/melanocytic nevi or basal cell carci- noma/seborrheic keratosis combinations are the most com- mon patterns. This result is not surprising because basal cell car- cinoma and melanocytic nevi are the most common tumors found on histopathological evaluation.2 However, combined tumors composed of keratinocytes and melanocytes are extre- mely rare.3 We describe a malignant cutaneous neoplasm with combined phenotypical features of basal cell carcinoma and malignant melanoma, also known as a malignant basomelano- cytic tumor.4
CASE REPORT
A 76-year-old female presented with a 3.5×2.5 cm, pigmen- ted, protruding mass on her left thigh one year in duration
(Fig. 1). The mass was painless and there were no additional palpable masses on the rest of her body, nor were relevant trauma or family history reported. Initial biopsy revealed a malignant tumor showing an intermingled pattern of melano- cytic and basaloid differentiation with positive immunoreac- tivity for Human Melanoma Black-45 (HMB-45)/S-100 and cytokeratin 5/6 (CK5/6). PET-CT was negative for lymph node and/or distant metastasis. Wide excision with surgical margins
CM Kim, et al. Malignant Basomelanocytic Tumor
222 Korean Journal of National Health Insurance Service Ilsan Hospital
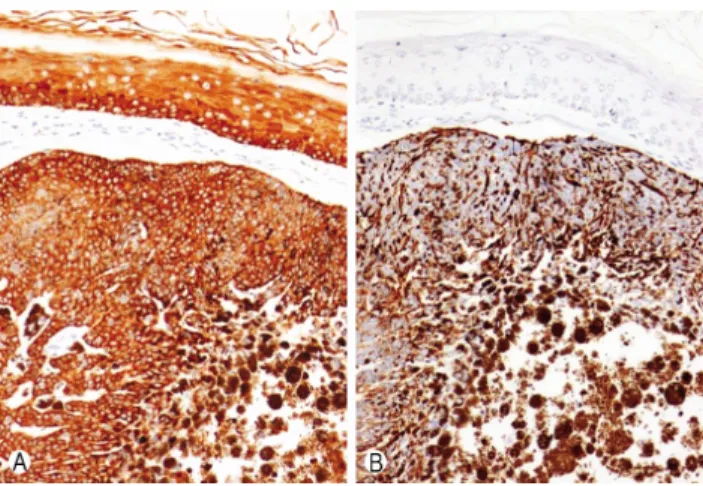
Fig. 3. Tumor cells are diffusely and strongly positive for cytoke-r atin 5/6 (CK5/6) similar to the normal epidermis (A), and are also diffusely and strongly positive for Human Melanoma Black-45 (HMB-45), a marker for melanoma (×200) (B).
Fig. 2. Histologically, tumor cells show basal cell carcinoma-like features such as cleft artifact and surrounding palisaded baso- philic cells with rather prominent nucleoli (H&E, ×200).
of at least 3 cm and a split thickness skin graft were perfor- med. Post-excision recovery was unremarkable. The pathology of the specimen was as follows. Tumor cells showed basal cell car- cinoma-like features such as cleft artifact and surrounding pali- saded basophilic cells, while also having rather prominent nuc- leoli (×200, hematoxylin and eosin (H&E); Fig. 2). Tumor cells were diffusely and strongly positive for CK5/6, similar to nor- mal epidermis, and were also diffusely and strongly positive for HMB-45, the marker for melanoma (×200; Fig. 3) In summary, the features indicated a combined tumor with features of both malignant melanoma; (tumor thickness, 3 mm, Clark level, IV;
tumor stage, T4a, N0, M0), and basal cell carcinoma.
DISCUSSION
Although the etiology of composite tumors remains unclear, several hypotheses have been proposed. First, one neoplasm can induce the development of a second tumor. Neoplasms secrete a growth mediator, and its paracrine effects can cause a second tumor to grow. Keratinocytes secrete a growth medi- ator that promotes the growth of melanocytes, and neoplastic keratinocytes cause tumors of melanocyte origin.5,6 Second, two tumors can coincidentally grow together. The case of colli- sion tumors supports this hypothesis. Boyd et al.,1 performed a retrospective evaluation of 40,000 cutaneous biopsies, yiel- ding 69 examples of collision tumors. A combination of mela- nocytic nevus and basal cell carcinoma was the most common.
Because basal cell carcinoma and melanocytic nevus are the most common tumors, they are most likely to form collision tumors.7 Third, each composite tumor may be differentiated
from one stem cell. Pluripotent stem cells have the capacity of self-renewal and can give rise to phenotypically diverse cells.8 Fourth, the field cancerization theory suggests that there is a high risk of developing two neoplasms within potential skin lesions associated with ultraviolet light, or burn scars. A num- ber of reports of composite tumors in the head and neck region after high exposure to ultraviolet light support this claim.6
The terminology used to define composite tumors was re- cently clarified to include collision, colonized, combined and biphenotypic tumors, which are defined as follows;6,9
1) Collision tumors - Two separate and distinct neoplasms are distinguishable and the two components are usually shar- ply demarcated (no mixed cells) within the tumor.
2) Colonization tumors - These tumors consist of one tumor cell population infiltrating and colonizing an underlying se- cond tumor cell population. The colonizing tumor cells do not extend beyond the dermal component of the second tumor cell population. More specifically, these tumors often repre- sent melanoma in situ colonizing a basal cell carcinoma. The underlying neoplasm may act a conduit for spread of another neoplastic cell throughout the initial neoplasm
3) Combined tumors - A tumor composed of two distinct populations of cells that are intermingled, which may require immunohistochemistry analysis for identification. Each cell population contains a different immunophenotypic pattern.
Basomelanocytic tumors and squamomelanocytic tumors are also classified as combined tumors.10
4) Biphenotypic tumors - A tumor arising from a common stem cell precursor that has evolved into two phenotypically- distinct tumors. These tumors co-express phenotypically diffe- rent immunohistochemical markers and features of two diver- gent cell populations on electron microscopy. Rosen et al repor-
김채민 외. 악성 기저 멜라닌 세포 암종
Volume 16 Number 2 December 2017
223 ted the only documented case of a true biphenotypic tumor.11
In our case, the tumor was composed of both malignant melanoma cells (HMB-45 positive) and palisaded basophilic cells, indicating basal cell carcinoma, and thus classified as a combined tumor. Combined malignant melanoma-basal cell carcinoma tumors are also called malignant basomelanocytic tumors. Malignant basomelanocytic tumors have been repor- ted in only about 100 cases worldwide, and this is the first report in an Asian population. Clinical features and treatment of malignant basomelanocytic tumors generally follows gui- delines for malignant melanoma; prognosis is influenced by the tumor depth of malignant melanoma.6,9
REFERENCES
1. Boyd AS, Rapini RP. Cutaneous collision tumors. An analysis of 69 cases and review of the literature. Am J Dermatopathol 1994;
16(3):253-7.
2. Braun-Falco M. Combined malignant melanoma and basal cell carcinoma tumor of the intermingled type. J Cutan Pathol 2007;
34(9):731-5.
3. Rodriguez J, Nonaka D, Kuhn E, Reichel M, Rosai J. Combi- ned high-grade basal cell carcinoma and malignant melanoma of the skin ("malignant basomelanocytic tumor"): report of two cases and review of the literature. Am J Dermatopathol 2005;
27(4):314-8.
4. Erickson LA, Myers JL, Mihm MC, Markovic SN, Pittelkow MR. Malignant basomelanocytic tumor manifesting as metas- tatic melanoma. Am J Surg Pathol 2004;28(10):1393-6.
5. Brownstein MH, Starink TM. Desmoplastic trichoepithelioma and intradermal nevus: a combined malformation. J Am Acad Dermatol 1987;17(3):489-92.
6. Cornejo KM, Deng AC. Malignant melanoma within squa- mous cell carcinoma and basal cell carcinoma: is it a combined or collision tumor?--a case report and review of the literature.
Am J Dermatopathol 2013; 35(2):226-34.
7. Hirakawa E, Miki H, Kobayashi S, Nomura Y, Ohmori M.
Collision tumor of cutaneous malignant melanoma and basal cell carcinoma. Pathol Res Pract 1998;194(9):649-53.
8. Pouryazdanparast P, Yu L, Johnson T, Fullen D. An unusual squamo-melanocytic tumor of uncertain biologic behavior: a variant of melanoma? Am J Dermatopathol 2009; 31(5):457-61.
9. Satter EK, Metcalf J, Lountzis N, Elston DM. Tumors compo- sed of malignant epithelial and melanocytic populations: a case series and review of the literature. J Cutan Pathol 2009;36(2):
211-9.
10. Goeser M, DiMaio DJ. A colonization of basal cell carcinoma by malignant melanoma in situ resembling a malignant baso- melanocytic tumor. Am J Dermatopathol 2014;36(11):e179-82.
11. Rosen LB, Benson J, Williams WD, Rywlin AM. A malignant neoplasm with features of both squamous cell carcinoma and malignant melanoma. Am J Dermatopathol 1984;6(Suppl 1):
213-9.