pISSN 2288-6575 • eISSN 2288-6796 http://dx.doi.org/10.4174/astr.2016.90.6.328 Annals of Surgical Treatment and Research
Comparison of perioperative and short-term outcomes between robotic and conventional laparoscopic surgery for colonic cancer: a systematic review and meta-analysis
Sungwon Lim*, Jin Hee Kim1,*, Se-Jin Baek2, Seon-Hahn Kim2, Seon Heui Lee3
National Evidence-Based Healthcare Collaborating Agency, Seoul, 1Department of Nursing, College of Medicine, Chosun University, Gwangju, 2Division of Colorectal Surgery, Department of Surgery, Korea University College of Medicine, Seoul,
3Department of Nursing Science, College of Nursing, Gachon University, Incheon, Korea
INTRODUCTION
In the last decade, laparoscopic surgery has become popular in many surgical fields due to its advantages compared to the open approach, such as less pain, faster recovery/resumption of daily activities, and better cosmesis [1,2]. However, because laparoscopic surgery is more technically demanding, for reasons including the limited range of instrument motion, relative
loss of dexterity, and inadequate visualization, laparoscopic surgery continues to be stressful for surgeons, and the learning curve is very steep [3,4]. The da Vinci robotic surgical system (Intuitive Surgical, Sunnyvale, CA, USA) has been applied to overcome the ergonomic discomfort of laparoscopic surgery, with advanced technologies including superior 3dimensional views and an internal articulated EndoWrist® that improves dexterity and allows seven degrees of freedom [5,6]. With these Purpose: Reports from several case series have described the feasibility and safety of robotic surgery (RS) for colonic cancer. Experience is still limited in robotic colonic surgery, and a few metaanalysis has been conducted to integrate the results for colon cancer specifically. We conducted a systematic review of the available evidence comparing the surgical safety and efficacy of RS with that of conventional laparoscopic surgery (CLS) for colonic cancer.
Methods: We searched English databases (MEDLINE, Embase, and Cochrane Library), and Korean databases (KoreaMed, KMbase, KISS, RISS, and KisTi). Dichotomous variables were pooled using the risk ratio, and continuous variables were pooled using the mean difference (MD).
Results: The present study found that the RS group had a shorter time to resumption of a regular diet (MD, –0.62 days;
95% CI, –0.97 to –0.28), first passage of flatus (MD, –0.44 days; 95% CI, –0.66 to –0.23) and defecation (MD, –0.62 days; 95%
CI, –0.77 to –0.47). Also, RS was associated with a shorter hospital stay (MD, –0.69 days; 95% CI, –1.12 to –0.26), a lower estimated blood loss (MD, –19.49 mL; 95% CI, –27.10 to –11.89) and a longer proximal margin (MD, 2.29 cm; 95% CI, 1.11- 3.47). However, RS was associated with a longer surgery time (MD, 51.00 minutes; 95% CI, 39.38–62.62).
Conclusion: We found that the potential benefits of perioperative and shortterm outcomes for RS than for CLS. For a more accurate understanding of RS for colonic cancer patients, robust comparative studies and randomized clinical trials are required.
[Ann Surg Treat Res 2016;90(6):328-339]
Key Words: Robotic surgical procedures, Colonic neoplasms
Reviewed January February March April May June July August September October November December
Received January 15, 2016, Reviewed March 12, 2016, Accepted March 14, 2016
Corresponding Author: Seon Heui Lee
Department of Nursing Science, College of Nursing, Gachon University, 191, Hambangmoe-ro, Yeonsu-gu, Incheon 21936, Korea
Tel: +82-32-820-4235, Fax: +82-32-820-4201 E-mail: [email protected]
*Sungwon Lim and Jin Hee Kim contributed equally to this study as co-first authors.
Copyright ⓒ 2016, the Korean Surgical Society
cc Annals of Surgical Treatment and Research is an Open Access Journal. All articles are distributed under the terms of the Creative Commons Attribution Non- Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
advantages, robotic surgery (RS) has been adopted rapidly for advanced surgical procedures in many fields, such as urologic, gynecologic, and cardiac surgery [79].
The first robotassisted colorectal surgery was reported in 2002 [10]. Recently, much of the reported data has been from robotic surgeries for rectal cancer, because robotic technology is of maximal advantage in narrow spaces such as the medi
astinum and pelvic cavity, and it is very useful for the pelvic dissection known as total mesorectal excision in rectal cancer surgery [11,12]. On the other hand, the role of robotic surgical systems in colonic surgery is still under debate. Thus, there are a few reports of robotassisted colonic surgery, and only one metaanalysis of RS for right colon cancer has been reported [13].
Therefore, we conducted a systematic review of the available evidence comparing the surgical safety and efficacy of RS with that of conventional laparoscopic surgery (CLS) for colonic cancer.
METHODS
Search strategy and study selection
We searched OvidMEDLINE (1946–2014), Embase (incep
tion–2014), and the Cochrane Library on June 25, 2014. Korean databases (KoreaMed, KMbase, KISS, RISS, and KisTi) also were searched. To ensure a highly sensitive search, we designed search strategies that included pertinent MeSH (medical
subject headings), common keywords, and comprehensive com
binations of them. Search terms combined patientrelated terms (colon neoplasms, colon cancer, colon carcinoma, and colon tumor), operation terms (colectomy) and intervention terms (robotic, computerassisted surgery, telerobot, remote operation, remote surgery, and da Vinci).
A total of 775 records were identified through the search.
After duplicates were removed, 635 studies were imported for the first title and abstract screening. We excluded 584 after examining the titles and abstracts, based on exclusion criteria.
A total of 51 articles were obtained to conduct the fulltext review. Next, we excluded 46 publications because 9 included nonrelevant patients, 4 included nonrelevant interventions, 2 included nonrelated comparators, 7 were not original papers, 23 were gray literature, and 1 was not in English or Korean. Also, one additional article was found during our hand searches of relevant bibliographies. We considered sample size, publication year, study design, and the number of outcomes of interest, in order to choose highquality data with a low risk of bias for publications with possible overlap. Ultimately, six publications were selected for the metaanalysis (Fig. 1).
Study eligibility
In accordance with the preferred reporting items for ran
domized controlled trials (RCTs), systematic reviews and meta
analysis statement, 2 authors (Lim and Kim) independently
Records identified through electronic DB -164Ovid-MEDLINE
-569Ovid-Embase -14Cochrane library
-28Domestic DB (KoreaMed et al.) 775 Total
635 Articles after duplicates removed
51 Potentially appropriate articles to be included in this study
5 All articles included in this study
6 All articles included in this study
584 Excluded by title and abstract review
46 9 4 2 7 23 1
Full-text articles excluded Reasons
- Not focused on patients with colon cancer - Not related with robotic surgery
- No comparison between RS and CLS - Not original articles
- Gray literature - Not English or Korean
1 Hand search
Fig. 1. Flow diagram of the study selec tion process. RS, robotic sur gery; CLS, conventional lapar- oscopic surgery.
evaluated the titles and abstracts of the references to exclude irrelevant studies, and fulltext review was subsequently performed for potentially relevant articles. The inclusion criteria allowed studies of patients with colonic cancer and compared surgical and patient outcomes between RS and CLS.
The inclusion criteria were as follows: (1) studies that focused on patients only with colonic cancer; (2) comparative studies of RS and CLS; and (3) studies that reported at least one outcome of interest. Studies were excluded if they were (1) not original articles and (2) preclinical studies and protocols.
Data extraction and quality assessment
Two independent authors (Lim and Kim) performed the data extraction and quality assessment using a data extraction form.
Quality assessment also was performed independently by the reviewers using the Cochrane Risk of Bias (RoB) for randomized con trolled trials [14] and the Risk of Bias Assessment tool for Nonrandomized Studies (RoBANS 2.0) for nonrandomized com parative studies [15]. RoB is composed of 7 domains and RoBANS 2.0 is composed of 8 domains to assess the metho
dological quality of studies. Each criterion was evaluated as
‘low risk of bias’, ‘high risk of bias’, or ‘unclear’. If the study did not mention a certain criterion, we evaluated it as ‘unclear’. In each instance of disagreement, the case was discussed with all authors.
Baseline characteristics of the study participants
Age, sex ratio, body mass index, American Society of Anesthe
siologists class, clinical stage and pathology, and tumor size were recorded as demographic and clinical characteristics.
Information about interventions
The collected information about RS and CLS included the extent of surgical colonic resection, the anastomosis technique (e.g., extracorporeal or intracorporeal) and the name of the equipment used.
Outcomes for safety
Adverse event and postoperative complication variables included 30day mortality, conversion to open surgery, ileus, anastomotic leakage, wound rupture, postoperative bleeding, pneumonia, chyloperitoneum, intraabdominal abscess, acute myocardiac infarction, stroke, wound infection, and urinary tract infection.
Outcomes for efficacy
Readmission rate, time to regular diet, time to first flatus, time to first defecation, proximal margin, distal margin, opera
tive time, length of stay, and estimated blood loss (EBL) were assessed.
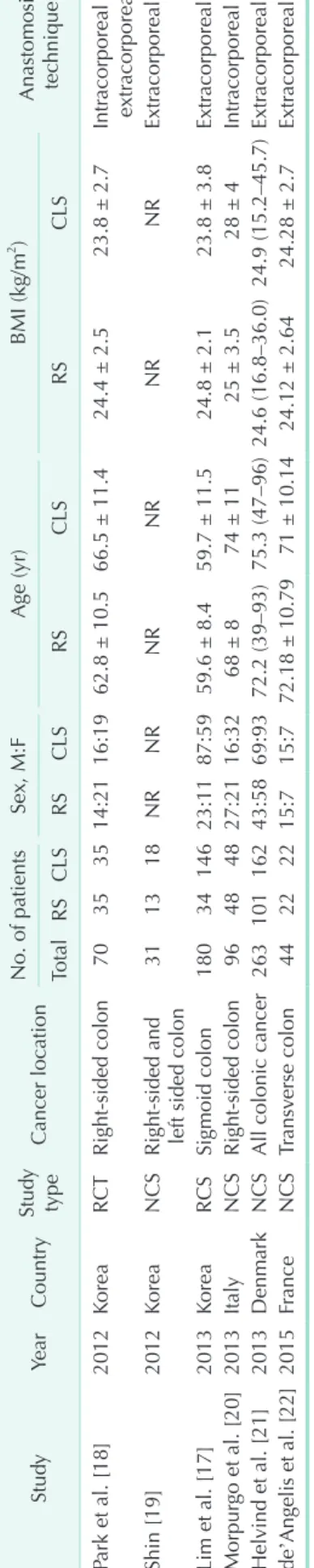
Table 1. Characteristics of the eligible studies StudyYearCountryStudy typeCancer locationNo. of patientsSex, M:FAge (yr)BMI (kg/m2 ) Anastomosis tec
hniqueTotalRSCLSRSCLSRSCLSRSCLS Park et al. [18]2012KoreaRCTRight-sided colon70353514:2116:1962.8 ± 10.566.5 ± 11.424.4 ± 2.523.8 ± 2.7Intracorporeal and extracorporeal Shin [19]2012KoreaNCS
Right-sided and left sided colon
311318NRNRNRNRNRNRExtracorporeal Lim et al. [17]2013KoreaRCSSigmoid colon1803414623:1187:5959.6 ± 8.459.7 ± 11.524.8 ± 2.123.8 ± 3.8Extracorporeal Morpurgo et al. [20]2013ItalyNCSRight-sided colon96484827:2116:3268 ± 874 ± 1125 ± 3.528 ± 4Intracorporeal Helvind et al. [21]2013DenmarkNCSAll colonic cancer26310116243:5869:9372.2 (39–93)75.3 (47–96)24.6 (16.8–36.0)24.9 (15.2–45.7)Extracorporeal de’Angelis et al. [22]2015FranceNCSTransverse colon44222215:715:772.18 ± 10.7971 ± 10.1424.12 ± 2.6424.28 ± 2.7Extracorporeal Values are presented as mean ± standard deviation or median (range) unless otherwise indicated. RS, robotic surgery; CLS, conventional laparoscopic surgery; BMI, body mass index; RCT, randomized controlled trials; NCS, nonconcurrent cohort study; RCS, retrospective cohort study; NR, no record.
Statistical analysis
We performed all metaanalyses with Review Manager, V. 5.3 (RevMan, Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014) and used the twotailed test of significance (P < 0.05). Dichotomous variables were pooled using the risk ratio (RR), and continuous variables were pooled using the mean difference (MD). RR and MD were cal
culated and reported with 95% confidence intervals (CI). The Cochrane Q statistic and I2 statistic were used to evaluate statistical heterogeneity [16]. A fixed effects model was used for studies with low or moderate statistical heterogeneity (I2 <
25, 25%–50%), and a random effects model was used for studies with high statistical heterogeneity (I2 > 50%). Metaanalyses of dichotomous variables were conducted using the Mantel
Haenszel method, and those of continuous variables were performed using the inverse variance method.
Ethical consideration
This study was reviewed and approved by the Institutional Review Board at the National EvidenceBased Healthcare Collaborating Agency (NECA); approval number: NECA IRB 14
019.
RESULTS
Study characteristics
Table 1 shows the characteristics of the included studies [1722]. The six studies included 684 patients: 253 in the RS group and 431 in the CLS group. One study was an RCT, one was a prospective cohort study, and four were historical cohort studies. Of the 6 studies, 3 were conducted in Korea, 1 was conducted in Italy, 1 was conducted in Denmark, and 1 was conducted in France. All studies had been published during the previous 4 years (2012–2015) (Table 1). Importantly, Shin [19] reported perioperative outcomes divided into leftsided and rightsided colon cancer. So, this outcomes were included respectively. The risk of bias in the RCT was high, and the quality of the cohort studies was poor. The detailed information is summarized in Fig. 2.
Safety outcomes
In terms of safety, there were no significant differences in operative outcome between the RS and CLS groups, including complications. The metaanalysis revealed no differences between the two groups in terms of 30day mortality (RR, 0.26;
95% CI, 0.03–2.13) and conversion to open surgery (RR, 1.06;
95% CI, 0.39–2.87). Also, no significant differences between
Unclear risk of bias Low risk of bias
0 25 50 75 100
% Random sequence generation (selection bias)
Allocation concealment (selection bias)
Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)
Selective reporting (reporting bias)
Other bias
0 25 50 75
% Comparability of participants
Selection of participants Confounding variables Measurement of exposure Blinding of outcome assessment Outcome evaluation Incomplete outcome data Selective reporting
100 Blinding of participants and personnel (performance bias)
Park 2012
Randomsequencegeneration(selectionbias) Allocationconcealment(selectionbias) Blindingofparticipantsandpersonnel(performancebias) Blindingofoutcomeassessment(detectionbias) Incompleteoutcomedata(attritionbias) Selectivereporting(reportingbias) Otherbias
de'Angelis 2015 Helvind 2013 Lim 2013 Morpurgo 2013 Shin 2012
Comparabilityofparticipants Selectionofparticipants Confoundingvariables Measurementofexposure Blindingofoutcomeassessment Outcomeevaluation Incompleteoutcomedata Selectiveoutcomereporting
High risk of bias
Unclear risk of bias Low risk of bias
High risk of bias
Fig. 2. Quality assessment of included studies. Quality assessment was performed using cochrane risk of bias (RoB) for ran- domized controlled trials and nonrandomized studies (RoBANS 2.0) for nonrandomized comparative studies. Green, low risk of bias; yellow, unclear; red, high risk of bias.
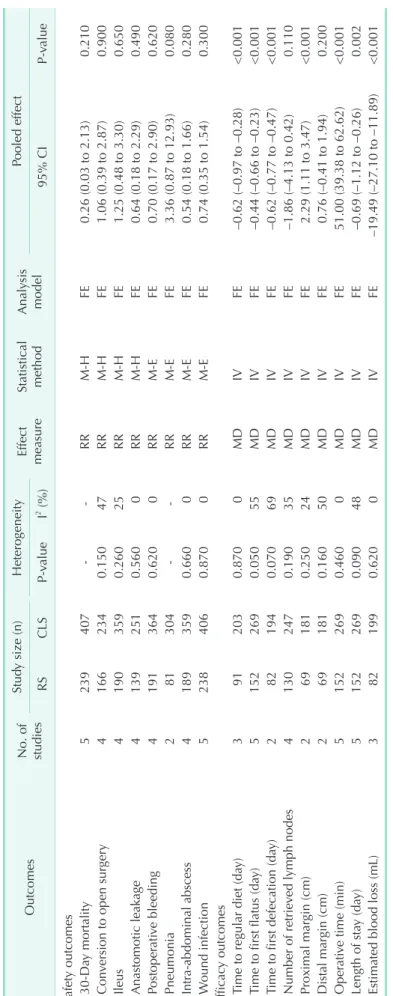
Table 2. Efficacy and safety outcomes Outcomes No. of studies
Study size (n)HeterogeneityEffect measureStatistical methodAnalysis modelPooled effect RSCLSP-valueI2 (%)95% CIP-value Safety outcomes 30-Day mortality5239407--RRM-HFE0.26 (0.03 to 2.13)0.210 Conversion to open surgery41662340.15047RRM-HFE1.06 (0.39 to 2.87)0.900 Ileus41903590.26025RRM-HFE1.25 (0.48 to 3.30)0.650 Anastomotic leakage41392510.5600RRM-HFE0.64 (0.18 to 2.29)0.490 Postoperative bleeding41913640.6200RRM-EFE0.70 (0.17 to 2.90)0.620 Pneumonia281304--RRM-EFE3.36 (0.87 to 12.93)0.080 Intra-abdominal abscess41893590.6600RRM-EFE0.54 (0.18 to 1.66)0.280 Wound infection52384060.8700RRM-EFE0.74 (0.35 to 1.54)0.300 Efficacy outcomes Time to regular diet (day)3912030.8700MDIVFE–0.62 (–0.97 to –0.28)<0.001 Time to first flatus (day)51522690.05055MDIVFE–0.44 (–0.66 to –0.23)<0.001 Time to first defecation (day)2821940.07069MDIVFE–0.62 (–0.77 to –0.47)<0.001 Number of retrieved lymph nodes41302470.19035MDIVFE–1.86 (–4.13 to 0.42)0.110 Proximal margin (cm)2691810.25024MDIVFE2.29 (1.11 to 3.47)<0.001 Distal margin (cm)2691810.16050MDIVFE0.76 (–0.41 to 1.94)0.200 Operative time (min)51522690.4600MDIVFE51.00 (39.38 to 62.62)<0.001 Length of stay (day)51522690.09048MDIVFE–0.69 (–1.12 to –0.26)0.002 Estimated blood loss (mL)3821990.6200MDIVFE–19.49 (–27.10 to –11.89)<0.001 RS, robotic surgery; CLS, conventional laparoscopic surgery; CI, confidence interval; RR, risk ratio; MD, mean difference; M-H, Mantel-Haenszel; IV, inverse variance; FE, fixed effects.
the 2 groups were found in complications such as ileus (RR, 1.25; 95% CI, 0.48–3.30), anastomotic leakage (RR, 0.64; 95% CI, 0.18–2.29), postoperative bleeding (RR, 0.70; 95% CI, 0.17–2.90), pneumonia (RR, 3.36; 95% CI, 0.87–12.93), intraabdominal abscess (RR, 0.54; 95% CI, 0.18–1.66), and wound infection (RR, 0.74; 95% CI, 0.35–1.54), with a low heterogeneity (Table 2).
Efficacy outcomes
Time to regular diet (days)
Three studies [17,18,22] analyzed the time to regular diet. The pooled estimates using a fixed effects model revealed that the time was significantly shorter for RS than for CLS (MD, −0.62 days; 95% CI, −0.97 to −0.28), with no heterogeneity between
Study or subgroup Mean SD Weight IV, Fixed, 95% CI
Robot Laparoscopy Mean difference
RCT
Park 2012 [18]
Subtotal (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 1.06 (P = 0.29)
Total (95% CI)
Heterogeneity: Chi = 0.27, df = 2 (P = 0.87); I = 0%
Test for overall effect: Z = 3.54 (P = 0.0004)
Test for subgroup dufferences: Chi = 0.00, df = 1 (P = 0.96); I = 0%
2 2
2 2
5.1 1.7 9.6%
9.6%
0.60 [ 1.71, 0.51]
0.60 [ 1.71, 0.51]
1
2 0 1 2
Favors robot Favors laparoscopy Total
35 35
Mean SD
5.7 2.9
Total IV,Fixed,95% CI
Mean difference
91 203 100.0% 0.62 [ 0.97, 0.28]
35 35
Cohort study de'Angelis 2015 Lim 2013 Subtotal (95% CI)
Heterogeneity: Chi = 0.27, df = 1 (P = 0.60); I = 0%
Test for overall effect: Z = 3.38 (P = 0.0007)
2 2
[22]
[17]
4.04 4.5
1.17 1.2
32.7%
57.7%
90.4%
0.50 [ 1.10, 0.10]
0.70 [ 1.16, 0.24]
0.63 [ 0.99, 0.26]
22 34 56
4.54 5.2
0.85 1.3
22 146 168
A
B
Study or subgroup Mean SD Weight IV, Fixed, 95% CI
Robot Laparoscopy Mean difference
RCT Park 2012 Subtotal (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 0.68 (P = 0.50) [18]
Total (95% CI)
Heterogeneity: Chi = 11.14, df = 5 (P = 0.05); I = 55%
Test for overall effect: Z = 4.05 (P < 0.0001)
Test for subgroup dufferences: Chi = 0.11, df = 1 (P = 0.74); I = 0%
2 2
2 2
2.6 1.4 6.2%
6.2%
0.30 [ 1.16, 0.56]
0.30 [ 1.16, 0.56]
1
2 0 1 2
Favors robot Favors laparoscopy Total
35 35
Mean SD
2.9 2.2
Total IV,Fixed,95% CI
Mean difference
152 269 100.0% 0.44 [ 0.66, 0.23]
35 35
Cohort study de'Angelis 2015 Lim 2013 Morpurgo 2013 Shin_1 2012 Shin_2 2012 Subtotal (95% CI)
Heterogeneity: Chi = 11.02, df = 4 (P = 0.03); I = 64%
Test for overall effect: Z = 4.00 (P < 0.0001)
2 2
[22]
[17]
[20]
[19]
[19]
2.45 2.21 2.4 3.3 3.5
1.05 0.9 0.8 0.7 0.5
15.2%
42.4%
90.4%
27.6%
7.0%
1.5%
93.8%
0.04 [ 0.51, 0.59]
0.31 [ 0.64, 0.02]
1.00 [ 1.41, 0.59]
0.30 [ 1.11, 0.51]
0.10 [ 1.83, 1.63]
0.45 [ 0.67, 0.23]
22 34 48 7 6 117
2.41 2.52 3.4 3.6 3.6
0.79 0.8 1.2 1.1 2.1
22 146 48 12 6 234
C
Study or subgroup Mean SD Weight IV, Fixed, 95% CI
Robot Laparoscopy Mean difference
Lim 2013 Morpurgo 2013 Total (95% CI)
Heterogeneity: Chi = 3.21, df = 1 (P = 0.07); I = 69%
Test for overall effect: Z = 8.05 (P < 0.00001)
2 2
[17]
[20]
3.85 3
0.2 1
88.3%
11.7%
100.0%
0.57 [ 0.73, 0.41]
1.00 [ 1.44, 0.56]
0.62 [ 0.77, 0.47]
0.5
1 0 0.5 1
Favors robot Favors laparoscopy Total
34 48 82
Mean SD 4.42
4 0.9 1.2
Total IV,Fixed,95% CI
Mean difference
146 48 194
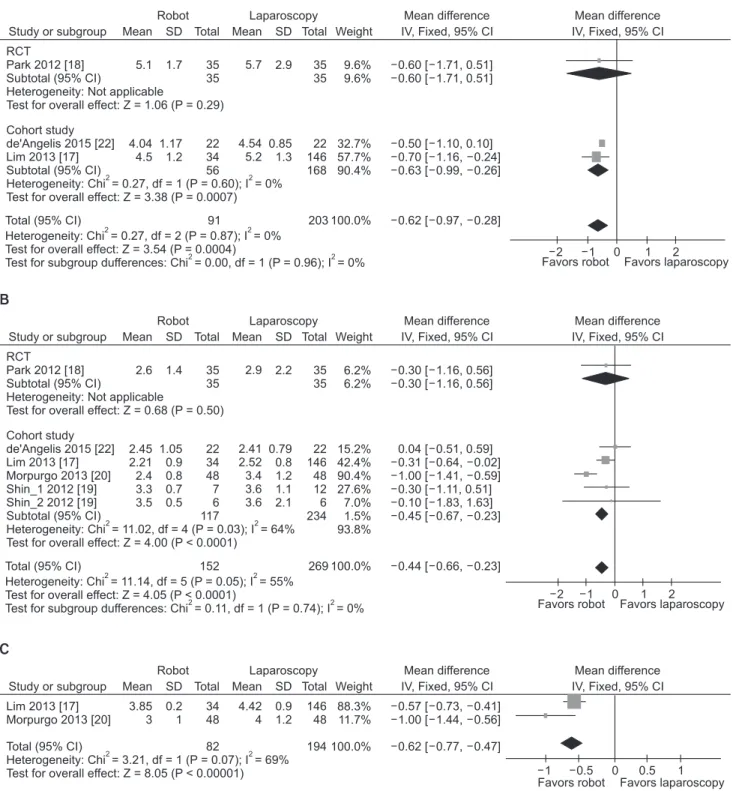
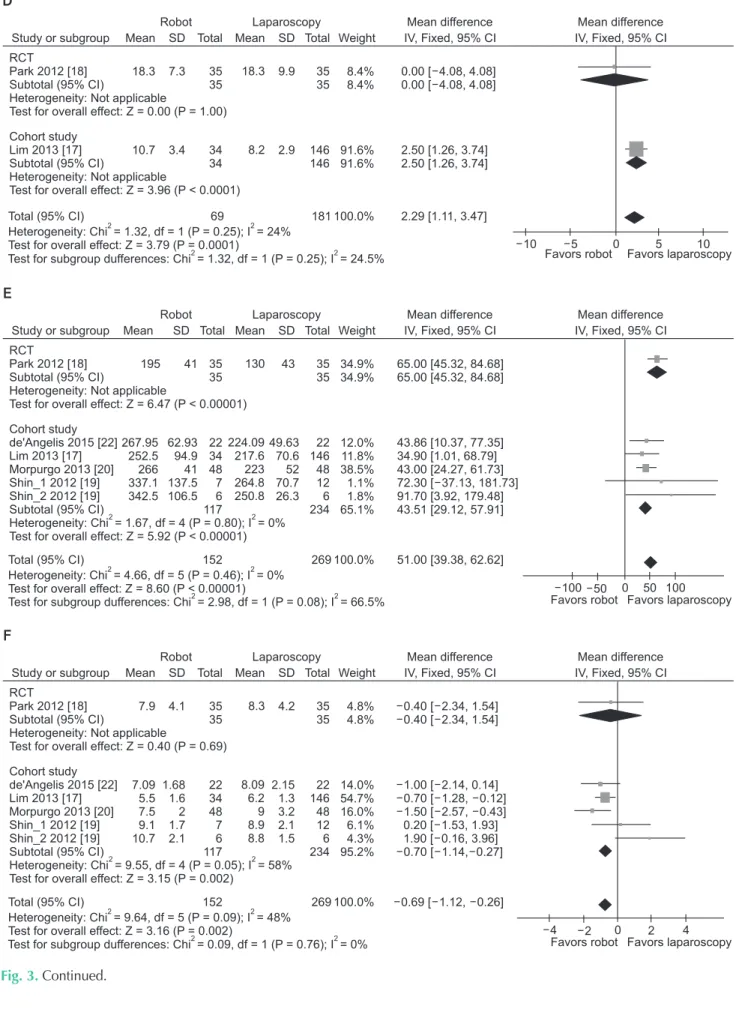
Fig. 3. Forest plot and meta-analysis of time to regular diet (A); time to first flatus (B); time to first defecation (C); number of proximal margin (D); operative time (E); length of stay (F); and estimated blood loss (G). SD, standard deviation; CI, confidence interval; RCT, randomized controlled trial.
E
Study or subgroup Mean SD Weight IV, Fixed, 95% CI
Robot Laparoscopy Mean difference
RCT Park 2012 Subtotal (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 6.47 (P < 0.00001) [18]
Total (95% CI)
Heterogeneity: Chi = 4.66, df = 5 (P = 0.46); I = 0%
Test for overall effect: Z = 8.60 (P < 0.00001)
Test for subgroup dufferences: Chi = 2.98, df = 1 (P = 0.08); I = 66.5%
2 2
2 2
195 41 34.9%
34.9%
65.00 [45.32, 84.68]
65.00 [45.32, 84.68]
100 50 0 50 100 Favors robot Favors laparoscopy Total
35 35
Mean SD
130 43
Total IV,Fixed,95% CI
Mean difference
152 269 100.0% 51.00 [39.38, 62.62]
35 35
Cohort study de'Angelis 2015 Lim 2013
Morpurgo 2013 [20]
Shin_1 2012 Shin_2 2012 Subtotal (95% CI)
Heterogeneity: Chi = 1.67, df = 4 (P = 0.80); I = 0%
Test for overall effect: Z = 5.92 (P < 0.00001)
2 2
[22]
[17]
[19]
[19]
267.95 252.5 266 337.1 342.5
62.93 94.9 41 137.5 106.5
12.0%
11.8%
38.5%
1.1%
1.8%
65.1%
43.86 [10.37, 77.35]
34.90 [1.01, 68.79]
43.00 [24.27, 61.73]
72.30 [ 37.13, 181.73]
91.70 [3.92, 179.48]
43.51 [29.12, 57.91]
22 34 48 7 6 117
224.09 217.6 223 264.8 250.8
49.63 70.6 52 70.7 26.3
22 146 48 12 6 234
F
Study or subgroup Mean SD Weight IV, Fixed, 95% CI
Robot Laparoscopy Mean difference
RCT Park 2012 Subtotal (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 0.40 (P = 0.69) [18]
Total (95% CI)
Heterogeneity: Chi = 9.64, df = 5 (P = 0.09); I = 48%
Test for overall effect: Z = 3.16 (P = 0.002)
2 2
7.9 4.1 4.8%
4.8%
0.40 [ 2.34, 1.54]
0.40 [ 2.34, 1.54]
4 2 0 2 4
Favors robot Favors laparoscopy Total
35 35
Mean SD
8.3 4.2
Total IV,Fixed,95% CI
Mean difference
152 269 100.0% 0.69 [ 1.12, 0.26]
35 35
Cohort study de'Angelis 2015 Lim 2013 Morpurgo 2013 Shin_1 2012 Shin_2 2012 Subtotal (95% CI)
Heterogeneity: Chi = 9.55, df = 4 (P = 0.05); I = 58%
Test for overall effect: Z = 3.15 (P = 0.002)
2 2
[22]
[17]
[20]
[19]
[19]
7.09 5.5 7.5 9.1 10.7
1.68 1.6 2 1.7 2.1
14.0%
54.7%
16.0%
6.1%
4.3%
95.2%
1.00 [ 2.14, 0.14]
[ 1.28, 0.12]
0.70
1.50 [ 2.57, 0.43]
0.20 [ 1.53, 1.93]
1.90 [ 0.16, 3.96]
0.70 [ 1.14, 0.27]
22 34 48 7 6 117
8.09 6.2 9 8.9 8.8
2.15 1.3 3.2 2.1 1.5
22 146 48 12 6 234
Study or subgroup Mean SD Weight IV, Fixed, 95% CI
Robot Laparoscopy Mean difference
RCT Park 2012 Subtotal (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 0.00 (P = 1.00) [18]
Total (95% CI)
Heterogeneity: Chi = 1.32, df = 1 (P = 0.25); I = 24%
Test for overall effect: Z = 3.79 (P = 0.0001)
2 2
18.3 7.3 8.4%
8.4%
0.00 [ 4.08, 4.08]
0.00 [ 4.08, 4.08]
5
10 0 5 10
Favors robot Favors laparoscopy Total
35 35
Mean SD
18.3 9.9
Total IV,Fixed,95% CI
Mean difference
69 181 100.0% 2.29 [1.11, 3.47]
35 35
Cohort study Lim 2013 Subtotal (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 3.96 (P < 0.0001)
[17] 10.7 3.4 91.6%
91.6%
2.50 [1.26, 3.74]
2.50 [1.26, 3.74]
34 34
8.2 2.9 146 146
D
Test for subgroup dufferences: Chi = 1.32, df = 1 (P = 0.25); I = 24.5%2 2
Test for subgroup dufferences: Chi = 0.09, df = 1 (P = 0.76); I = 0%2 2
Fig. 3. Continued.
the studies (P = 0.870, I2 = 0%) (Table 2, Fig. 3A).
Time to first flatus (days)
Five studies [1720,22] analyzed the time to first flatus. The pooled estimates using a fixed effects model revealed that the time was significantly shorter for RS than for CLS (MD, −0.44 days; 95% CI, −0.66 to −0.23), with no heterogeneity among the studies (P = 0.050, I2 = 55%) (Table 2, Fig. 3B).
Time to first defecation (days)
Two studies [17,20] analyzed the time to first defecation. The pooled estimates using a fixed effects model revealed that the time was significantly shorter for RS than for CLS (MD, −0.62 days; 95% CI, −0.77 to −0.47), with heterogeneity between the studies (P = 0.070, I2 = 69%) (Table 2, Fig. 3C).
Proximal margin (cm)
Two studies [17,18] reported the proximal margin. Signifi
cantly longer proximal margins were observed in patients undergoing RS than in those undergoing CLS (MD, 2.29 cm; 95%
CI, 1.11–3.47), with no heterogeneity (P = 0.250, I2 = 24%) (Table 2, Fig. 3D).
Operative time (min)
The operating time was reported in five studies [1720,22]
comparing RS and CLS. The pooled estimates using a fixed effects model revealed a significantly longer operating time for RS than for CLS (MD, 51.00 minutes; 95% CI, 39.38–62.62), with no heterogeneity (P = 0.460, I2 = 0%) (Table 2, Fig. 3E).
Length of stay (days)
The length of stay was reported in five studies [1720,22]
comparing RS and CLS. The pooled estimates using a fixed effects model revealed a significantly shorter length of stay RS than for CLS (MD, −0.69 days; 95% CI, −1.12 to −0.26), with a low heterogeneity (P = 0.090, I2 = 48%) (Table 2, Fig. 3F).
Estimated blood loss (mL)
The EBL was reported in 3 studies [1719] comparing RS and CLS. The pooled estimates using a fixed effects model revealed a significantly lower blood loss for RS than for CLS (MD, −19.49 mL; 95% CI, −27.10 to −11.89), with no heterogeneity (P = 0.620, I2 = 0%) (Table 2, Fig. 3G).
Finally, no significant differences were found between the 2 groups in the number of retrieved lymph nodes (MD, –1.86;
95% CI, –4.13 to 0.42) or the distal margins (MD, 0.76 cm; 95%
CI, –0.41 to 1.94) (Table 2).
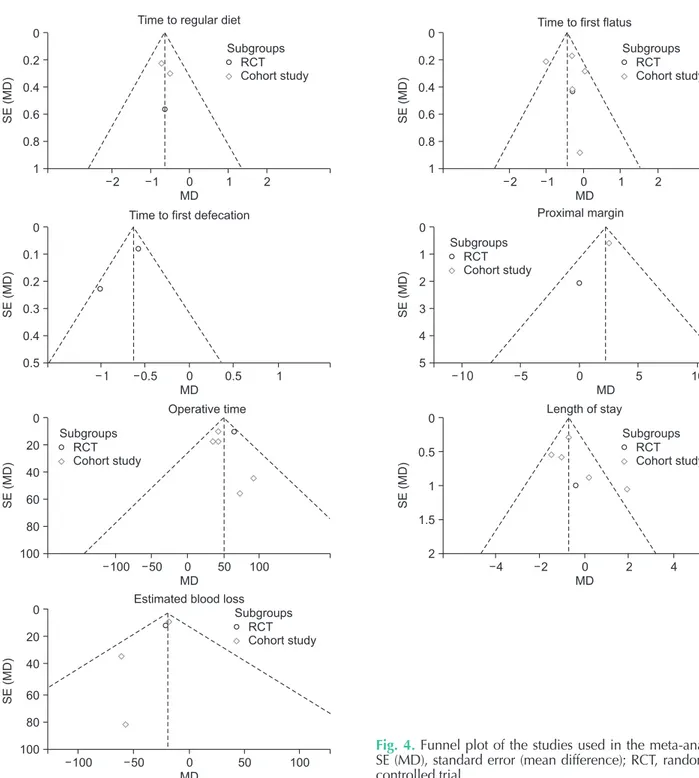
Publication bias
Publication bias was tested using the funnel plot analysis of the studies on the overall postoperative outcomes after RS compared to those after CLS. The funnel plot representing potential publication bias among the studies was fairly symmetric (Fig. 4)
DISCUSSION
Our study showed that robotassisted colectomy was feasible and safe compared with CLS in terms of intraoperative and postoperative complications and the rate of open conversion.
G
Study or subgroup Mean SD Weight IV, Fixed, 95% CI
Robot Laparoscopy Mean difference
RCT Park 2012 Subtotal (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 3.04 (P = 0.002) [18]
Total (95% CI)
Heterogeneity: Chi = 1.77, df = 3 (P = 0.62); I = 0%
Test for overall effect: Z = 5.02 (P < 0.00001)
Test for subgroup dufferences: Chi = 0.07, df = 1 (P = 0.79); I = 0%
2 2
2 2
35.8 26.3 31.5%
31.5%
21.00 [ 34.54, 7.46]
21.00 [ 34.54, 7.46]
50
100 0 50 100
Favors robot Favors laparoscopy Total
35 35
Mean SD
56.8 31.3
Total IV,Fixed,95% CI
Mean difference
82 199 100.0% 19.49 [ 27.10, 11.89]
35 35
Cohort study Lim 2013 Shin_1 2012 Shin_2 2012 Subtotal (95% CI)
Heterogeneity: Chi = 1.70, df = 2 (P = 0.43); I = 0%
Test for overall effect: Z = 4.01 (P < 0.0001)
2 2
[17]
[19]
[19]
60.3 105.7 185
27 80 70.4
67.0%
1.2%
0.2%
68.5%
17.90 [ 27.19, 8.61]
[ 129.72, 7.72]
61.00
56.70 [ 217.48,104.08]
18.80 [ 27.99, 9.60]
34 7 6 47
78.2 166.7 241.7
12.3 61.5 188.2
146 12 6 164
Fig. 3. Continued.
In addition, the times to diet resumption, recovery of bowel function, and postoperative hospital release were shorter in the RS group than in the CLS group. In the RS group, the EBL was lower and the proximal margin of the specimen was longer, but the operative time was significantly longer than in the CLS group. These results are similar to those of other published studies and the previous metaanalysis for rectal cancer [12,23
25].
To date, most of the published data for robotic colorectal surgery have described rectal cancer surgery, because the
advantages of robotic technology are maximized in narrow spaces such as the pelvic cavity, and robotic systems have been adopted more rapidly for rectal surgery than for colonic surgery [11,26]. Most of the studies comparing robotic rectal surgery with conventional laparoscopic rectal surgery have reported good results for RS in terms of safety outcomes, and comparable or better results in terms of efficacy outcomes, except for operation time. The current study demonstrated that the advantages of robotic systems shown in rectal surgery also hold true in colonic surgery. To date, there has been only one
0.2 0.4 0.6 0.8
2 1 0 1 2
SE(MD)
1 0
MD
RCT Cohort study Subgroups
0.2 0.4 0.6 0.8
2 1 0 1 2
SE(MD)
1 0
MD
RCT Cohort study Subgroups
0.1 0.2 0.3 0.4
0.5 0 0.5 1
SE(MD)
0.5 0
MD
1 2 3 4
5 0 5 10
SE(MD)
5 0
MD RCT
Cohort study Subgroups
20 40 60 80
100 50 0 50 100
SE(MD)
100 0
MD RCT
Cohort study Subgroups
0.5
1
1.5
4 2 0 2 4
SE(MD)
2 0
MD
RCT Cohort study Subgroups
20 40
60 80
100 50 0 50 100
SE(MD)
100 0
MD
RCT Cohort study Subgroups
Time to regular diet Time to first flatus
Time to first defecation Proximal margin
Operative time Length of stay
Estimated blood loss
Fig. 4. Funnel plot of the studies used in the meta-analysis.
SE (MD), standard error (mean difference); RCT, randomized controlled trial.
systematic review comparing robotic and laparoscopic surgeries for right colectomy, which was reported by Xu et al. [13].
Otherwise, our study is the first systematic review including whole colonic surgery from the right colon to the sigmoid colon.
In fact, colonic surgery can be divided largely into rightsided colectomy and leftsided colectomy, and the 2 types of surgery are very different. There are differences between the 2 groups in most fields of anatomy, tumor characteristics, methods of dissection and anastomosis, and these can affect the incidence of complications and the prognosis. Therefore, the advantages of robotic systems may differ in rightsided colectomy and leftsided colectomy generally. In conventional laparoscopic rightsided colectomy, extracorporeal stapled anastomosis is commonly performed through minilaparotomy. Robotic technology in rightsided colectomy facilitates intra corporeal handsewn anastomosis, and can reduce the incision size for specimen extraction, shift the incision site to a Pfannenstiel incision, cause less pain, less incisional hernia and allow better cosmesis [20,27,28]. On the other hand, the advantages of robotic leftside colectomy can be expected to be similar to those of robotic rectal surgery, such as nerve preservation during inferior mesenteric artery dissection, and easy mobilization of the splenic flexure [29].
Because the expected advantages of robotic technology differ among surgery types, the fact that this study included whole colectomy may be a limitation. Nevertheless, it may be an important and significant finding of this study that the advantage of robotic rectal surgery can be applied equally for colonic surgery. In our study, robotic colectomy was not only feasible, but also safe compared with CLS. However, the operative time was significantly longer in the RS group, as reported in other studies, because additional time may be necessary for robot setup, docking, and the learning curve [30].
A very interesting observation in our study was that there was no difference in the conversion rates of robotic and laparoscopic colectomy. Xu et al. [13] reported similar results.
In previous reports of rectal surgery, however, the conversion rate usually was lower in the RS group than in the CLS group [2325], because the robotic system may help to overcome the anatomical difficulty of the narrow pelvis; this point has been important in justifying the use of robotic rectal surgery. On the contrary, the level of difficulty of colectomy is easy compared with proctectomy, so this advantage of RS may not appear significant for colectomy, although there are some merits of RS for intracorporeal suture or splenic flexure mobilization. Thus, there might not be a significant difference in the conversion rates of the two procedures. This has been the weak point in the justification of the very high cost of RS compared with laparoscopic surgery for colectomy, unlike for rectal surgery, and remains a controversial topic. As our study also demonstrated, however, there are many advantages of RS, such as lower
blood loss, earlier recovery of bowel function, shorter hospital stays, and longer proximal margins of the specimens, and future studies should be performed to evaluate more potential advantages of robotics.
Despite our findings, this study has several limitations.
First, there were limitations in the metaanalysis because of the lack of primary studies comparing RS and CLS for patients with colonic cancer. There is a need for additional highquality primary studies, and when a sufficient number of primary studies become available for analysis, another systematic review and metaanalysis should be conducted and compared with this study. Second, in the present study, three out of 6 studies were conducted among Koreans living in South Korea. The regional concentration of a study population commonly influences the generalizability and makes it difficult to interpret the results in the context of other countries. Finally, the comparability of the studies included in the metaanalysis was weak due to differences in baseline attributes between patients who underwent RS and CLS in the cohorts. In 2 of the 6 studies, patients who received RS were younger than those who received CLS, and the tumor sizes differed between patients who had received RS and CLS.
Prospective, protocoled longterm followup studies that report the oncologic results of both CLS and RS are needed to evaluate the safety and efficacy of RS. Moreover, this technique for patients with colonic cancer is still in its infancy, and thus, the technique must be reassessed once the learning curve has been overcome.
In conclusion, the present study found the times to resump
tion of a regular diet, first passage of flatus and defecation were shorter for RS than for CLS. Also, RS was associated with a shorter hospital stay, lower EBL and longer proximal margin than CLS. However, RS was associated with a longer surgery time. For a more accurate understanding of RS for colonic cancer patients, robust comparative studies and randomized clinical trials including a sizeable number of subjects that take into account future actions are required.
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
ACKNOWLEDGEMENTS
This study was funded by the National Evidencebased Healthcare Collaborating Agency in the Republic of Korea (NH14002).
1. Jayne DG, Guillou PJ, Thorpe H, Quirke P, Copeland J, Smith AM, et al. Randomized trial of laparoscopicassisted resection of colorectal carcinoma: 3year results of the UK MRC CLASICC Trial Group. J Clin Oncol 2007;25:30618.
2. Colon Cancer Laparoscopic or Open Resec
tion Study Group, Buunen M, Veldkamp R, Hop WC, Kuhry E, Jeekel J, et al.
Survival after laparoscopic surgery versus open surgery for colon cancer: longterm outcome of a randomised clinical trial.
Lancet Oncol 2009;10:4452.
3. Wexner SD, Bergamaschi R, Lacy A, Udo J, Brolmann H, Kennedy RH, et al. The current status of robotic pelvic sur gery:
results of a multinational interdiscipli
nary consensus conference. Surg Endosc 2009;23:43843.
4. Schwab KE, Dowson HM, Van Dellen J, Marks CG, Rockall TA. The uptake of laparoscopic colorectal surgery in Great Britain and Ireland: a questionnaire sur
vey of consultant members of the ACPGBI.
Colorectal Dis 2009;11:31822.
5. Gutt CN, Oniu T, Mehrabi A, Kashfi A, Schemmer P, Buchler MW. Robotassisted abdominal surgery. Br J Surg 2004;91:1390
7.
6. Lanfranco AR, Castellanos AE, Desai JP, Meyers WC. Robotic surgery: a current perspective. Ann Surg 2004;239:1421.
7. Patel VR, Thaly R, Shah K. Robotic radical prostatectomy: outcomes of 500 cases.
BJU Int 2007;99:110912.
8. Veljovich DS, Paley PJ, Drescher CW, Everett EN, Shah C, Peters WA 3rd. Robotic surgery in gynecologic oncology: program initiation and outcomes after the first year with comparison with laparotomy for endometrial cancer staging. Am J Obstet Gynecol 2008;198:679.e19.
9. Leff JD, Enriquez LJ. Roboticassisted car
diac surgery. Int Anesthesiol Clin 2012;
50:7889.
10. Weber PA, Merola S, Wasielewski A, Ballantyne GH. Teleroboticassisted lapar
oscopic right and sigmoid colectomies for
benign disease. Dis Colon Rectum 2002;
45:168994.
11. Spinoglio G, Summa M, Priora F, Quarati R, Testa S. Robotic colorectal surgery: first 50 cases experience. Dis Colon Rectum 2008;51:162732.
12. Lee SH, Lim S, Kim JH, Lee KY. Robotic versus conventional laparoscopic surgery for rectal cancer: systematic review and metaanalysis. Ann Surg Treat Res 2015;
89:190201.
13. Xu H, Li J, Sun Y, Li Z, Zhen Y, Wang B, et al. Robotic versus laparoscopic right colec
tomy: a metaanalysis. World J Surg Oncol 2014;12:274.
14. Higgins JP, Green S, editors. Cochrane handbook for systematic reviews of inter
ventions. version 5.1.0 [Internet]. The Cochrane Collaboration, 2011 [uptated 2011 Mar; cited 2015 Dec 26]. Available from: http://handbook.cochrane.org.
15. Kim SY, Park JE, Lee YJ, Seo HJ, Sheen SS, Hahn S, et al. Testing a tool for assessing the risk of bias for nonrandomized stu
dies showed moderate reliability and pro
mising validity. J Clin Epidemiol 2013;66:
40814.
16. Higgins JP, Thompson SG. Quantifying heterogeneity in a metaanalysis. Stat Med 2002;21:153958.
17. Lim DR, Min BS, Kim MS, Alasari S, Kim G, Hur H, et al. Robotic versus laparoscopic anterior resection of sigmoid colon cancer:
comparative study of longterm oncologic outcomes. Surg Endosc 2013;27:137985.
18. Park JS, Choi GS, Park SY, Kim HJ, Ryuk JP. Randomized clinical trial of robotassi
sted versus standard laparoscopic right colectomy. Br J Surg 2012;99:121926.
19. Shin JY. Comparison of shortterm sur
gical outcomes between a robotic colec
tomy and a laparoscopic colectomy during early experience. J Korean Soc Coloproctol 2012;28:1926.
20. Morpurgo E, Contardo T, Molaro R, Zerbinati A, Orsini C, D’Annibale A.
Roboticassisted intracorporeal anas to
mosis versus extracorporeal anastomosis
in laparoscopic right hemi colec tomy for cancer: a case control study. J Lapar
oendosc Adv Surg Tech A 2013;23:4147.
21. Helvind NM, Eriksen JR, Mogensen A, Tas B, Olsen J, Bundgaard M, et al. No dif ferences in shortterm morbidity and mor tality after robotassisted laparoscopic versus laparoscopic resection for colonic cancer: a casecontrol study of 263 pa
tients. Surg Endosc 2013;27:257580.
22. de’Angelis N, Alghamdi S, Renda A, Azoulay D, Brunetti F. Initial experience of robotic versus laparoscopic colectomy for transverse colon cancer: a matched casecontrol study. World J Surg Oncol 2015;13:295.
23. Trastulli S, Farinella E, Cirocchi R, Cavaliere D, Avenia N, Sciannameo F, et al. Robotic resection compared with lapar oscopic rectal resection for cancer:
sys tematic review and metaanalysis of shortterm outcome. Colorectal Dis 2012;
14:e13456.
24. Memon S, Heriot AG, Murphy DG, Bressel M, Lynch AC. Robotic versus laparoscopic proctectomy for rectal cancer: a metaan
alysis. Ann Surg Oncol 2012;19:2095101.
25. Xiong B, Ma L, Zhang C, Cheng Y. Robotic versus laparoscopic total mesorectal exci
sion for rectal cancer: a metaanalysis. J Surg Res 2014;188:40414.
26. D’Annibale A, Morpurgo E, Fiscon V, Trevisan P, Sovernigo G, Orsini C, et al.
Robotic and laparoscopic surgery for treat
ment of colorectal diseases. Dis Colon Rectum 2004;47:21628.
27. deSouza AL, Prasad LM, Park JJ, Marecik SJ, Blumetti J, Abcarian H. Robotic assis
tance in right hemicolectomy: is there a role? Dis Colon Rectum 2010;53:10006.
28. D’Annibale A, Pernazza G, Morpurgo E, Monsellato I, Pende V, Lucandri G, et al.
Robotic right colon resection: evaluation of first 50 consecutive cases for malignant disease. Ann Surg Oncol 2010;17:285662.
29. Bae SU, Baek SJ, Hur H, Baik SH, Kim NK, Min BS. Robotic left colon cancer resection: a dual docking technique that
REFERENCES
maximizes splenic flexure mobilization.
Surg Endosc 2015;29:13039.
30. Choi DJ, Kim SH, Lee PJ, Kim J, Woo SU.
Singlestage totally robotic dissection for rectal cancer surgery: technique and shortterm outcome in 50 consecutive
patients. Dis Colon Rectum 2009;52:1824
30.
![Table 1 shows the characteristics of the included studies [1722]. The six studies included 684 patients: 253 in the RS group and 431 in the CLS group](https://thumb-ap.123doks.com/thumbv2/123dokinfo/5199285.116984/4.918.101.828.613.1065/table-shows-characteristics-included-studies-studies-included-patients.webp)