저작자표시-비영리-변경금지 2.0 대한민국 이용자는 아래의 조건을 따르는 경우에 한하여 자유롭게 l 이 저작물을 복제, 배포, 전송, 전시, 공연 및 방송할 수 있습니다. 다음과 같은 조건을 따라야 합니다: l 귀하는, 이 저작물의 재이용이나 배포의 경우, 이 저작물에 적용된 이용허락조건 을 명확하게 나타내어야 합니다. l 저작권자로부터 별도의 허가를 받으면 이러한 조건들은 적용되지 않습니다. 저작권법에 따른 이용자의 권리는 위의 내용에 의하여 영향을 받지 않습니다. 이것은 이용허락규약(Legal Code)을 이해하기 쉽게 요약한 것입니다. Disclaimer 저작자표시. 귀하는 원저작자를 표시하여야 합니다. 비영리. 귀하는 이 저작물을 영리 목적으로 이용할 수 없습니다. 변경금지. 귀하는 이 저작물을 개작, 변형 또는 가공할 수 없습니다.
Prognostic significance of preoperative
neutrophil-to-lymphocyte ratio and
platelet-to-lymphocyte ratio in patients with
non-metastatic clear cell renal cell carcinoma
by
Jung Hwan Lee
Major in Medicine
Prognostic significance of preoperative
neutrophil-to-lymphocyte ratio and
platelet-to-lymphocyte ratio in patients with
non-metastatic clear cell renal cell carcinoma
by
Jung Hwan Lee
A Dissertation Submitted to The Graduate School of
Ajou University in Partial Fulfillment of the Requirements
for the Degree of
Master of Medicine
Supervised by
Sun Il Kim, M.D., Ph.D.
Major in Medicine
Department of Medical Sciences
The Graduate School, Ajou University
This certifies that the dissertation
of Jung Hwan Lee is approved.
SUPERVISORY COMMITTEE
Sun Il Kim
Se Joong Kim
Hyun Soo Ahn
The Graduate School, Ajou University
June, 19th, 2015
i
-Abstract-
Prognostic significance of preoperative neutrophil-to-lymphocyte
ratio and platelet-to-lymphocyte ratio in patients with
non-metastatic clear cell renal cell carcinoma
Introduction & Objectives: This study was performed to evaluate the significance of preoperative neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) as a predictive factor for recurrence in patients with non-metastatic clear cell renal cell carcinoma (RCC).
Material & Methods: We retrospectively reviewed the medical records of 341 patients (232 men and 109 women, mean age of 54.9 years) with non-metastatic clear cell RCC who underwent radical or partial nephrectomy between March 1995 and July 2012. Patients longer than 12 months follow-up were included. The prognostic significance of various clinicopathological variables for recurrence-free survival and cancer specific-free survival was analyzed by using univariate and multivariate analysis.
Results: The median follow-up duration was 48 months (mean, 54.1; range, 12-215 months). Of the total 341 patients, 37 patients (10.9%) developed metastases and 14 patients (4.1%) died of renal cell carcinoma among 21 patients who died during the follow-up period. Preoperative NLR was significantly correlated with symptom presentation (p=0.008), tumor size (p=0.022), T stage (p=0.004), neutrophil count (p<0.001), lymphocyte count (p<0.001), recurrence at follow-up (p=0.006). Preoperative PLR was significantly correlated with symptom presentation (p<0.001), lymphocyte count (p<0.001), recurrence at follow-up (p=0.002). In the univariate analysis, clinical presentation, tumor size, T stage, Fuhrman grade, preoperative hemoglobin, neutrophil count, NLR, PLR were significant prognostic factors for recurrence-free survival. The 5-year recurrence-free survival rate of patients with a higher preoperative NLR (≥2.5) was significantly lower than that of patients with a lower preoperative NLR (<2.5) (86.5% vs. 96.7%, p=0.006). The 5-year recurrence-free survival rate of patients with a higher preoperative PLR (≥130) was significantly lower than that of patients with a lower preoperative PLR (<130) (89.4% vs. 96.8%, p=0.022). In the multivariate analysis, tumor size (p<0.001), T stage (p<0.001), Fuhrman grade (p=0.015)
ii
and preoperative hemoglobin (p=0.026) were independent prognostic factors for recurrence-free survival.
Conclusions: An increased preoperative NLR and PLR were associated with a higher recurrence rate in patients with non-metastatic clear cell RCC, although it was not an independent prognostic factor for recurrence-free survival.
iii
TABLE OF CONTENTS
ABSTRACT··· i
TABLE OF CONTENTS ··· iii
LIST OF TABLES ··· iv
Ⅰ. INTRODUCTION ··· 1
Ⅱ. MATERIALS AND METHODS ··· 2
Ⅲ. RESULTS ··· 3
Ⅳ. DISCUSSION ··· 11
Ⅴ. CONCLUSION ··· 13
REFERENCES ··· 14
iv
LIST OF TABLES
Table 1. Clinicopathological data of the 341 patients included in the study ··· 5
Table 2.1. Relationship between preoperative neutrophil-to-lymphocyte ratio (NLR) level and clinicopathological variables in the 341 patients included in the study··· 6
Table 2.2. Relationship between preoperative platelet-to-lymphocyte ratio (PLR) level and clinicopathological variables in the 341 patients included in the study ··· 7
Table 3. Univariate and multivariate analysis of potential prognostic factors for recurrence-free survival ··· 8
Figure 1. Recurrence free survival by T stage ··· 9
Figure 2. Recurrence free survival by hemoglobin ··· 9
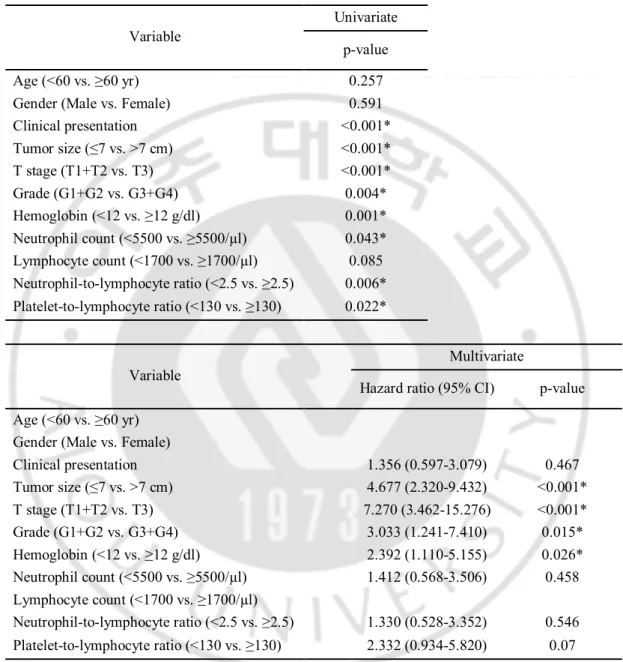
Figure 3. Recurrence free survival by NLR ··· 9
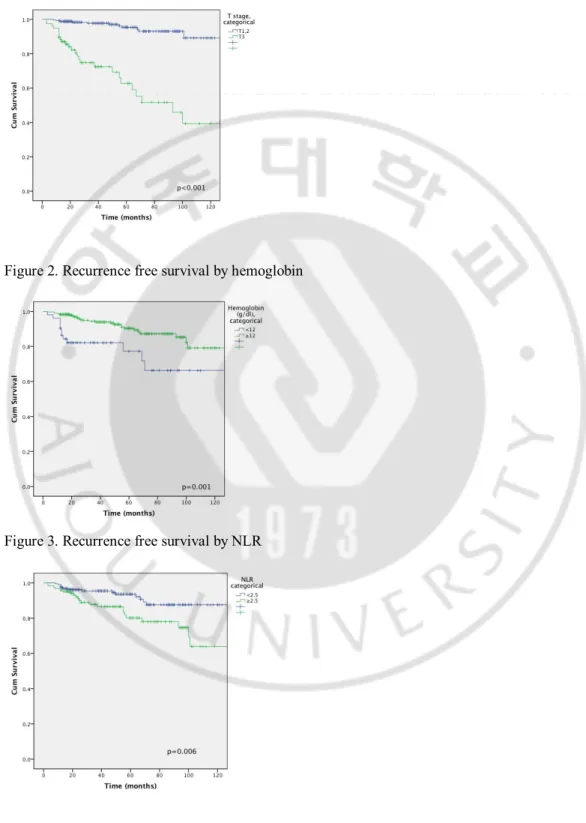
Figure 4. Recurrence free survival by PLR ··· 10
Figure 5. Recurrence free survival by symptom at presentation ··· 10
1
I. INTRODUCTION
Renal cell carcinoma (RCC) is the 14th most common cancer in the world (Ferlay et al., 2010) and the most common cancer arising from adult renal parenchyma. (Lipworth et al., 2006) Widespread use of abdominal ultrasound and computed tomography has increased the number of incidentally detected RCCs (Pichler et al., 2012). These tumors are often smaller and of lower stage. Surgery, either radical nephrectomy or partial nephrectomy including the tumor, remains the only curative treatment. After the treatment of RCC, the local recurrence or metastasis rate from 10% to 20% (Bower and Lamkin, 2013) (Solinas et al., 2009). Local recurrence or metastasis following surgery portends poor prognosis, because RCC is unresponsive to conventional cytotoxic chemotherapy, with 3 year survival rate of 11~88%. (Eggener et al., 2006) Traditional prognostic factors include tumor size, histological subtype, Fuhrman nuclear grade and tumor stage. Although these factors have correlated well with prognosis following surgery, they seem to be inadequate in predicting which patient will have recurrence in a more contemporary cohort of patients who have tendency to get an earlier diagnosis and treatment. Moreover, histological subtype, Fuhrman nuclear grade and tumor stage are obtained post-operatively, which are impossible to use to predict recurrence preoperatively. If one could identify prognostic factors preoperatively more accurate risks stratification can be accessed that could be applied in treatment planning and patient counseling. For these factors to be clinically useful, they should be routinely available, inexpensive, well standardized and validated in different patients.
It is increasingly being recognized that inflammation can affect tumor growth, invasion and metastasis (Mantovani et al., 2008). Likewise, systemic inflammatory markers, either alone or in combination, have also been shown to be related with cancer progression, such as plasma C-reactive protein (CRP), Glasgow Prognostic Score (GPS), neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR). (Mantovani et al., 2008) (Cho et al., 2011) For these factors to be clinically useful, they should be routinely available, inexpensive, well standardized and validated in different patients. Recent reports indicate that increased pretreatment NLR or PLR is associated with a worse prognosis in several tumors, including
2
lung, bladder, prostate, breast, colorectal cancer and RCC. (Ohno et al., 2010; Kaynar et al., 2014; Kemal et al., 2014; Lorente et al., 2015) It has been hypothesized that the synthesis of inflammatory cytokines triggered by the tumor microenvironment alters acute phase reactants and hematological components including serum neutrophil and lymphocyte counts. (Mantovani et al., 2008; Grivennikov et al., 2010)
We hypothesized that a greater preoperative NLR and PLR is associated with higher recurrence with radical nephrectomy (RN) or partial nephrectomy (PN). Accordingly, the study was performed to evaluate the significance of preoperative NLR and PLR as a predictive factor for recurrence in patients with non-metastatic clear cell RCC.
II. MATERIALS AND METHODS
All patients who underwent radical or partial nephrectomy at Ajou University Hospital, between March 1995 and July 2012 were systematically searched. Exclusion criteria included benign surgical pathology, non-clear cell type RCC, bilateral tumors, history of other cancer and preoperative treatment. Three hundred forty-one patients diagnosed with non-metastatic clear cell RCC (T1-4N0M0) with at least 12 months of follow-up were finally included. Tumor stage was determined according to the 1997 UICC TNM classification of malignant tumors. The clinical and pathological variables recorded included age, sex, symptoms at presentation, size of tumor, T stage, Fuhrman nuclear grade, hemoglobin, neutrophil count, lymphocyte count, NLR and PLR. The baseline marker of systemic inflammation data was obtained within 4 weeks before the operation. Presentation was categorized into symptomatic or incidental. Symptoms at presentation included gross hematuria, flank pain and palpable abdominal mass. After surgery, patients were followed-up every 3 months for the first 2 years, every 6 months for the next 2 years and yearly thereafter. Physical examination, chest X-ray and laboratory test including complete blood count, serum routine chemistry, serum electrolytes, erythrocyte sedimentation rate, CRP and urinalysis were performed at each visit. Abdominal computed tomography was obtained every 6 months during the first 2 years and yearly thereafter. The study end point was recurrence-free
3
survival. The time to recurrence was defined as the time from RN or PN to the time of radiological detection of recurrence.
NLR was defined as elevated if it were higher than or equal to 2.5 as proposed by Ohno et al. (Ohno et al., 2010) Also, PLR was defined as elevated if it were higher than or equal to 130 at which the survival difference between the two groups was maximized. According to the level of preoperative NLR and PLR, patients were divided into high NLR and normal NLR groups and high PLR and normal PLR groups. Continuous variables including age and tumor size were analyzed as dichotomous variables according to approximate optimal cutoff points. The prognostic significance of various clinical and pathologic variables for
recurrence-free survival was analyzed by using univariate and multivariate analysis. Survival curves were constructed by the Kaplan-Meier method. Comparison of survival in the
univariate survival analysis was done with the log rank test. Multivariate analysis was performed by Cox regression analysis with forward stepwise variable selection. SPSS ver. 16.0 (SPSS Inc., Chicago, IL, USA) was used for all statistics. Values of p<0.05 were considered to be statistically significant in all of the analyses.
III. RESULTS
Total 390 patients underwent surgery for RCC. 6 patients with pathologic stage T4, 41 patients with less than 12 months follow-up, 1 bilateral RCC and 1 concomitant lymphoma patient were excluded. Table 1 summarizes the characteristics of the study patients. Of the 361 patients, 232 (68%) were men and 109 (32.0%) were women. 210 (61.6%) patients were aged over 60. 294 (86.2%) patients had incidentally detected tumors. 263 (77.1%) patients had T1 or T2 tumor and 284 (83.3) patients had smaller than 7cm sized tumors. 125 (36.6%) patients had high NLR (≥2.5) and 168 (49.3%) patients had high PLR (≥130). The median follow-up duration was 48 months (mean 54.1 months; range, 12-215 months). Of the total 341 patients, 37 (10.9%) developed metastases and 14 (4.1%) died of RCC. Table 2 shows relationship of preoperative NLR level and PLR level with clinicopathological variables. High preoperative NLR was significantly associated with symptom at presentation (p=0.008),
4
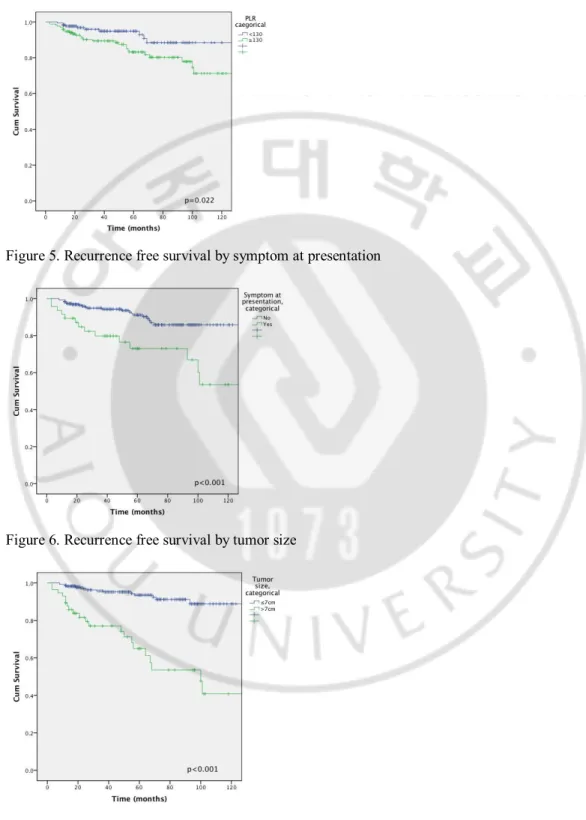
bigger tumor size (p=0.022), higher T stage (p=0.004), higher neutrophil count (p<0.001), lower lymphocyte count (p<0.001), and higher recurrence at follow-up (p=0.006). High preoperative PLR was significantly associated with symptom at presentation (p<0.001), lower lymphocyte count (p<0.001), and higher recurrence at follow-up (p=0.002). In the univariate analysis, symptom at presentation, tumor size, T stage, Fuhrman grade, preoperative hemoglobin, neutrophil count, NLR and PLR were significant prognostic factors for recurrence-free survival. The 5-year recurrence-free survival rate of patients with a high preoperative NLR (≥2.5) was significantly lower than that of patients with a lower preoperative NLR (<2.5) (86.5% vs. 96.7%, p=0.006). And the 5-year recurrence-free survival rate of patients with a higher preoperative PLR (≥130) was significantly lower than that of patients with a lower preoperative PLR (<130) (89.4% vs. 96.8%, p=0.022). In the multivariate analysis, tumor size (p<0.001), T stage (p<0.001), Fuhrman grade (p=0.015) and preoperative hemoglobin (p=0.026) were independent prognostic factors for recurrence-free survival. NLR and PLR were not independent prognostic factors. Figure 1 to 6 show Kaplan-Meier survival curves by symptom at presentation, tumor size, T stage, Fuhrman grade, preoperative hemoglobin, NLR and PLR, which were significant independent factor in univariate analysis.
5
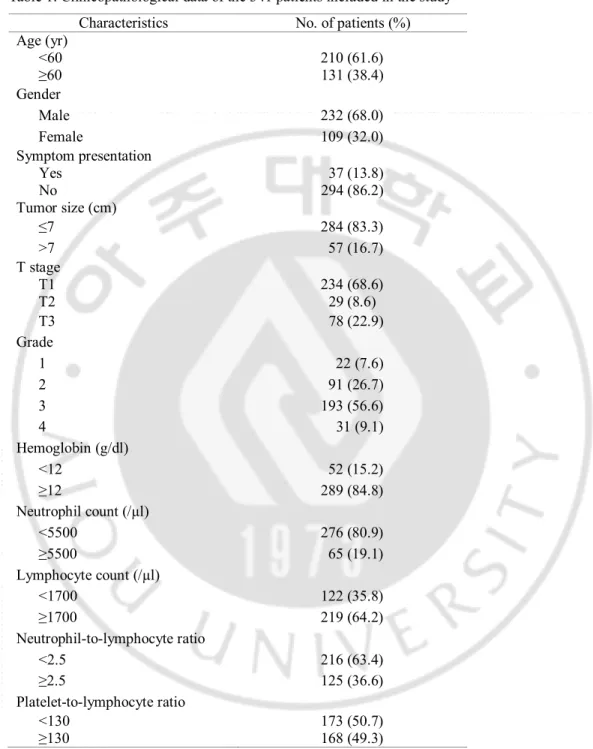
Table 1. Clinicopathological data of the 341 patients included in the study Characteristics No. of patients (%) Age (yr) <60 210 (61.6) ≥60 131 (38.4) Gender Male 232 (68.0) Female 109 (32.0) Symptom presentation Yes No Tumor size (cm) 37 (13.8) 294 (86.2) ≤7 284 (83.3) >7 57 (16.7) T stage T1 234 (68.6) T2 29 (8.6) T3 78 (22.9) Grade 1 22 (7.6) 2 91 (26.7) 3 193 (56.6) 4 31 (9.1) Hemoglobin (g/dl) <12 52 (15.2) ≥12 289 (84.8) Neutrophil count (/µl) <5500 276 (80.9) ≥5500 65 (19.1) Lymphocyte count (/µl) <1700 122 (35.8) ≥1700 219 (64.2) Neutrophil-to-lymphocyte ratio <2.5 216 (63.4) ≥2.5 125 (36.6) Platelet-to-lymphocyte ratio <130 173 (50.7) ≥130 168 (49.3)
6
Table 2.1. Relationship between preoperative neutrophil-to-lymphocyte ratio (NLR) level and clinicopathological variables in the 341 patients included in the study
Variable NLR <2.5 NLR ≥2.5 p-value Age (yr) 0.493 <60 136 74 ≥60 80 51 Gender 0.152 Male 141 91 Female 75 34 Symptom presentation 0.008 Yes 195 96 No 21 29 Tumor size (cm) 0.022 ≤7 188 96 >7 28 29 T stage 0.004 T1+T2 178 85 T3 38 40 Grade 0.707 G1+G2 73 40 G3+G4 140 84 Hemoglobin (g/dl) 0.078 <12 27 25 ≥12 189 100 Neutrophil count (/µl) <0.001 <5500 201 75 ≥5500 15 50 Lymphocyte count (/µl) <0.001 <1700 44 78 ≥1700 172 47 Recurrence 0.006 No 201 103 Yes 15 22
7
Table 2.2. Relationship between preoperative platelet-to-lymphocyte ratio (PLR) level and clinicopathological variables in the 341 patients included in the study
Variable PLR <130 PLR ≥130 p-value Age (yr) 0.585 <60 109 101 ≥60 64 67 Gender 0.054 Male 126 106 Female 47 62 Symptom presentation 0.001 Yes 13 34 No 160 134 Tumor size (cm) 0.087 ≤7 150 134 >7 23 34 T stage 0.883 T1+T2 134 129 T3 39 39 Grade 0.593 G1+G2 60 53 G3+G4 112 112 Hemoglobin (g/dl) 0.056 <12 20 32 ≥12 153 136 Neutrophil count (/µl) 0.995 <5500 140 136 ≥5500 33 32 Lymphocyte count (/µl) <0.001 <1700 22 100 ≥1700 151 68 Recurrence 0.002 No 163 141 Yes 10 27
8
Table 3. Univariate and multivariate analysis of potential prognostic factors for recurrence-free survival
Variable
Univariate p-value Age (<60 vs. ≥60 yr) 0.257 Gender (Male vs. Female) 0.591 Clinical presentation <0.001* Tumor size (≤7 vs. >7 cm) <0.001* T stage (T1+T2 vs. T3) <0.001* Grade (G1+G2 vs. G3+G4) 0.004* Hemoglobin (<12 vs. ≥12 g/dl) 0.001* Neutrophil count (<5500 vs. ≥5500/µl) 0.043* Lymphocyte count (<1700 vs. ≥1700/µl) 0.085 Neutrophil-to-lymphocyte ratio (<2.5 vs. ≥2.5) 0.006* Platelet-to-lymphocyte ratio (<130 vs. ≥130) 0.022* Variable Multivariate
Hazard ratio (95% CI) p-value Age (<60 vs. ≥60 yr)
Gender (Male vs. Female)
Clinical presentation 1.356 (0.597-3.079) 0.467 Tumor size (≤7 vs. >7 cm) 4.677 (2.320-9.432) <0.001* T stage (T1+T2 vs. T3) 7.270 (3.462-15.276) <0.001* Grade (G1+G2 vs. G3+G4) 3.033 (1.241-7.410) 0.015* Hemoglobin (<12 vs. ≥12 g/dl) 2.392 (1.110-5.155) 0.026* Neutrophil count (<5500 vs. ≥5500/µl) 1.412 (0.568-3.506) 0.458 Lymphocyte count (<1700 vs. ≥1700/µl) Neutrophil-to-lymphocyte ratio (<2.5 vs. ≥2.5) 1.330 (0.528-3.352) 0.546 Platelet-to-lymphocyte ratio (<130 vs. ≥130) 2.332 (0.934-5.820) 0.07 CI: Confidence interval
9 Figure 1. Recurrence free survival by T stage
Figure 2. Recurrence free survival by hemoglobin
10 Figure 4. Recurrence free survival by PLR
Figure 5. Recurrence free survival by symptom at presentation
11
IV. DISCUSSION
The evidences of relationship of systemic inflammation and cancer development and progression are increasing but not fully understood. (Mantovani et al., 2008) A systemic inflammatory response can be assessed by the concentration of acute inflammatory phase proteins, such as CRP, fibrinogen, ferritin, albumin and transferring, platelet or peripheral blood leukocyte components, including neutrophil counts and lymphocyte counts. (Wu et al., 2014) NLR calculated by dividing neutrophil counts by lymphocyte counts, is suggested as a marker for general immune responses to various stress stimuli. (Schetter et al., 2009) Elevated neutrophil counts can secrete reactive oxygen species (ROS), which induce cell DNA damage and genetic instability, causing both carcinogenesis and promotion in tumor microenvironment. (Garber, 2009) Neutrophils are also reported to contain and secrete pro-angiogenic factors, including vascular endothelial growth factor (VEGF). Platelets play an important role in cancer progression. They affect tumor growth by angiogenesis via the cytokine VEGF. (Ohno et al., 2010) The absence of Von Hippel-Lindau gene and high VEGF expression is well established in RCC. (Kim et al., 2014) Elevated inflammatory factors were triggered by cancer related inflammatory factors, such as tumor necrotizing factor, interleukin-6, granulocyte colony stimulating factor, and myeloid growth factors. (Seidel et al., 2012) (Liang et al., 2012) Lymphocytes suppress tumor maturation, the cytotoxic T lymphocytes induce apoptosis of cancer cells with the interaction of Fas ligand on the cytotoxic T lymphocyte. (Yang et al., 2011) In breast cancer, tumor infiltrating lymphocytes are an important prognostic factor that higher lymphocytes level associated with a better outcome and better response to anthracycline-based chemotherapy. (Winter et al., 2010) (Kim et al., 2015)
Some studies concluded that high preoperative NLR value is a predictor indicating mortality in RCC. (Joslyn et al., 2005) (Fox et al., 2013) But, Pichler et al. reported that a high NLR is not a prognostic factor in RCC. (Pichler et al., 2013) They found high NLR as an independent prognostic factor in overall survival mortality, but not cancer specific mortality. Association of platelet count and prognosis also have some debates, but many
12
studies support platelet count and PLR is associated with poor prognosis. (Fox et al., 2013; Gu et al., 2015) In our study NLR was not an independent prognostic factor in multivariate analysis. The difference may be our study has relatively short follow-up period and lower recurrence rate, and previous other studies have mixed histological subtype RCC and metastatic tumors also included. Metastatic tumors have more aggressive behavior and have more elevated systemic inflammation. These differences may affect the results. Other study found high NLR in clear cell RCC is related with overall survival rate, but not with recurrence free survival rate nor with cancer specific survival rate. (Zhang et al., 2013) They considered overall survival rate was associated with higher adverse cardiac events, diabetes or susceptibility to bacteremia might contribute to overall survival rate.
The studies to find the optimal cutoff value of NLR or PLR were tried in many cancers (Watanabe et al., 2014) (Azab et al., 2013). The cutoff values were decided by the median value, compare values of 4 quartiles, most significant value according to the log rank test with all possible cutoffs.
Radical nephrectomy remains a standard treatment in management of RCC. Approximately, one-third of patients with RCC have metastases at diagnosis. For patients who diagnosed with localized tumor, one-third will develop recurrence and progression. (Leibovich and Blute, 2008) Bad pathologic features of the primary renal tumor (nuclear grade 3 or 4, presence of a sarcomatoid component, tumor size >10cm, tumor stage pT3 or pT4 and presence of coagulative tumor necrosis) Blute et al proposed a protocol for lymph node dissection (LND) based on metastatic risk. (Blute et al., 2004) Although level one evidence suggests that lymphadenectomy gives no survival benefit for clinical node-negative disease, the selected patients who underwent RN, found positive lymph node. But most pathologic features are not available before the treatment. Ohno et al suggested preoperative risk stratification model based on T stage and NLR. (Ohno et al., 2010)
The present study has a number of limitations. The patients may have concurrent morbidity, including infection that can affect the leukocyte counts. Follow-up period were short. Multi-center and large cohort study will overcome these limitations.
13
V. CONCLUSION
This study shows that an increased preoperative NLR and PLR were associated with a higher recurrence rate in patients with non-metastatic clear cell RCC, although it was not an independent prognostic factor for recurrence-free survival. Larger prospective studies are required to confirm the prognostic value of NLR and PLR.
14
REFERENCES
1. Azab B, Shah N, Radbel J, Tan P, Bhatt V, Vonfrolio S, Habeshy A, Picon A, Bloom S: Pretreatment neutrophil/lymphocyte ratio is superior to platelet/lymphocyte ratio as a predictor of long-term mortality in breast cancer patients. Med Oncol 30: 432, 2013
2. Blute ML, Leibovich BC, Cheville JC, Lohse CM, Zincke H: A protocol for performing extended lymph node dissection using primary tumor pathological features for patients treated with radical nephrectomy for clear cell renal cell carcinoma. J Urol 172: 465-469, 2004
3. Bower JE, Lamkin DM: Inflammation and cancer-related fatigue: mechanisms, contributing factors, and treatment implications. Brain Behav Immun 30 Suppl: S48-57, 2013
4. Cho DS, Kim SJ, Lee SH, Ahn HS, Kim YS, Kim SI: Prognostic significance of preoperative C-reactive protein elevation and thrombocytosis in patients with non-metastatic renal cell carcinoma. Korean J Urol 52: 104-109, 2011 5. Eggener SE, Yossepowitch O, Pettus JA, Snyder ME, Motzer RJ, Russo P:
Renal cell carcinoma recurrence after nephrectomy for localized disease: predicting survival from time of recurrence. J Clin Oncol 24: 3101-3106, 2006
6. Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM: Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer 127: 2893-2917, 2010
7. Fox P, Hudson M, Brown C, Lord S, Gebski V, De Souza P, Lee CK: Markers of systemic inflammation predict survival in patients with advanced renal cell cancer. Br J Cancer 109: 147-153, 2013
8. Garber K: First results for agents targeting cancer-related inflammation. J Natl Cancer Inst 101: 1110-1112, 2009
15
Cell 140: 883-899, 2010
10. Gu L, Li H, Gao Y, Ma X, Chen L, Li X, Zhang Y, Fan Y, Zhang X: The association of platelet count with clinicopathological significance and prognosis in renal cell carcinoma: a systematic review and meta-analysis. PLoS One 10: e0125538, 2015
11. Joslyn SA, Sirintrapun SJ, Konety BR: Impact of lymphadenectomy and nodal burden in renal cell carcinoma: retrospective analysis of the National Surveillance, Epidemiology, and End Results database. Urology 65: 675-680, 2005
12. Kaynar M, Yildirim ME, Badem H, Cavis M, Tekinarslan E, Istanbulluoglu MO, Karatas OF, Cimentepe E: Bladder cancer invasion predictability based on preoperative neutrophil-lymphocyte ratio. Tumour Biol 35: 6601-6605, 2014
13. Kemal Y, Yucel I, Ekiz K, Demirag G, Yilmaz B, Teker F, Ozdemir M: Elevated Serum Neutrophil to Lymphocyte and Platelet to Lymphocyte Ratios Could be Useful in Lung Cancer Diagnosis. Asian Pacific Journal of Cancer Prevention 15: 2651-2654, 2014
14. Kim S, Miller BJ, Stefanek ME, Miller AH: Inflammation-induced activation of the indoleamine 2,3-dioxygenase pathway: Relevance to cancer-related fatigue. Cancer, 2015
15. Kim T, Zargar-Shoshtari K, Dhillon J, Lin HY, Yue B, Fishman M, Sverrisson EF, Spiess PE, Gupta S, Poch MA, Sexton WJ: Using Percentage of Sarcomatoid Differentiation as a Prognostic Factor in Renal Cell Carcinoma. Clin Genitourin Cancer, 2014
16. Leibovich BC, Blute ML: Lymph node dissection in the management of renal cell carcinoma. Urol Clin North Am 35: 673-678; viii, 2008
17. Liang ZL, Kang K, Yoon S, Huang SM, Lim JS, Kim JM, Lim JS, Lee HJ: NDRG2 is involved in the oncogenic properties of renal cell carcinoma and its loss is a novel independent poor prognostic factor after
16
nephrectomy. Ann Surg Oncol 19: 2763-2772, 2012
18. Lipworth L, Tarone RE, McLaughlin JK: The epidemiology of renal cell carcinoma. J Urol 176: 2353-2358, 2006
19. Lorente D, Mateo J, Templeton AJ, Zafeiriou Z, Bianchini D, Ferraldeschi R, Bahl A, Shen L, Su Z, Sartor O, de Bono JS: Baseline neutrophil-lymphocyte ratio (NLR) is associated with survival and response to treatment with second-line chemotherapy for advanced prostate cancer independent of baseline steroid use. Ann Oncol 26: 750-755, 2015
20. Mantovani A, Allavena P, Sica A, Balkwill F: Cancer-related inflammation. Nature 454: 436-444, 2008
21. Ohno Y, Nakashima J, Ohori M, Hatano T, Tachibana M: Pretreatment neutrophil-to-lymphocyte ratio as an independent predictor of recurrence in patients with nonmetastatic renal cell carcinoma. J Urol 184: 873-878, 2010
22. Pichler M, Hutterer GC, Chromecki TF, Jesche J, Kampel-Kettner K, Pummer K, Zigeuner R: Renal cell carcinoma stage migration in a single European centre over 25 years: effects on 5- and 10-year metastasis-free survival. Int Urol Nephrol 44: 997-1004, 2012
23. Pichler M, Hutterer GC, Stoeckigt C, Chromecki TF, Stojakovic T, Golbeck S, Eberhard K, Gerger A, Mannweiler S, Pummer K, Zigeuner R: Validation of the pre-treatment neutrophil-lymphocyte ratio as a prognostic factor in a large European cohort of renal cell carcinoma patients. Br J Cancer 108: 901-907, 2013
24. Schetter AJ, Nguyen GH, Bowman ED, Mathe EA, Yuen ST, Hawkes JE, Croce CM, Leung SY, Harris CC: Association of inflammation-related and microRNA gene expression with cancer-specific mortality of colon adenocarcinoma. Clin Cancer Res 15: 5878-5887, 2009
25. Seidel C, Busch J, Weikert S, Steffens S, Fenner M, Ganser A, Grunwald V: Progression free survival of first line vascular endothelial growth
factor-17
targeted therapy is an important prognostic parameter in patients with metastatic renal cell carcinoma. Eur J Cancer 48: 1023-1030, 2012
26. Solinas G, Germano G, Mantovani A, Allavena P: Tumor-associated macrophages (TAM) as major players of the cancer-related inflammation. J Leukoc Biol 86: 1065-1073, 2009
27. Watanabe T, Shibata M, Nishiyama H, Soeda S, Furukawa S, Gonda K, Takenoshita S, Fujimori K: Serum levels of rapid turnover proteins are decreased and related to systemic inflammation in patients with ovarian cancer. Oncol Lett 7: 373-377, 2014
28. Winter H, Meimarakis G, Angele MK, Hummel M, Staehler M, Hoffmann RT, Hatz RA, Lohe F: Tumor infiltrated hilar and mediastinal lymph nodes are an independent prognostic factor for decreased survival after pulmonary metastasectomy in patients with renal cell carcinoma. J Urol 184: 1888-1894, 2010
29. Wu Y, Hu X, Song L, Zhu J, Yu R: The inhibitory effect of a novel polypeptide fraction from Arca subcrenata on cancer-related inflammation in human cervical cancer HeLa cells. ScientificWorldJournal 2014: 768938, 2014
30. Yang J, Li A, Yang Y, Li X: Identification of cyclophilin A as a potential prognostic factor for clear-cell renal cell carcinoma by comparative proteomic analysis. Cancer Biol Ther 11: 535-546, 2011
31. Zhang J, Wang P, Ouyang H, Yin J, Liu A, Ma C, Liu L: Targeting cancer-related inflammation: Chinese herbal medicine inhibits epithelial-to-mesenchymal transition in pancreatic cancer. PLoS One 8: e70334, 2013
18 -국문요약-
비전이 투명 신세포암 환자의 수술 전 호중구/림프구 비율과
혈소판/림프구 비율의 예후적 중요도
아주대학교 대학원 의학과 이정환 (지도교수: 김선일) 목적: 비전이 투명 신세포암 환자의 수술 전 호중구/림프구 비율과 혈소판/림프 구 비율의 예후적 중요도에 관해 알아보고자 하였다. 대상 및 방법: 1995년 3월부터 2012년 7월까지 비전이 투명 신세포암으로 아주 대학교 병원에서 근치적 혹은 부분 신절제술을 시행 받은 341명의 환자 (남자 232명, 여자 109명; 나이 평균치 54.9세)를 대상으로 하였으며, 최소 12개월 이상의 경과 관찰이 시행된 환자를 대상으로 하였다. 일변량 분석 및 다변량 분 석을 통해 여러 임상병리 변수들이 재발 없는 잔존율 및 암특이 생존율에 미치 는 예후적 가치에 관해 조사하였다. 결과: 추적 관찰 기간의 중앙치는 48개월(평균 54.1, 범위: 12-215개월)이였으 며, 341명의 환자 중 37명(10.9%)의 환자에서 재발 하였으며 21명의 환자가 사망하였고 이 중 14명(4.1%)의 환자가 암으로 인해 사망하였다. 술 전 호중구 /림프구 비율은 증상발현(p=0.008), 종양 크기(p=0.022), T 병기(p=0.004), 호중구수(p<0.001), 림파구수(p<0.001), 암재발(p=0.006)과 통계적 상관 관계 를 보였고, 술 전 혈소판/림파구 비율은 증상발현(p<0.001), 림파구수 (p<0.001), 암재발(p=0.002)과 통계적 상관관계를 보였다. 일변량 분석에서는 증상발현, 종양 크기, T 병기, Furhman 등급, 술 전 적혈구 수, 호중구 수, 호중 구/림프구 비율, 혈소판/림프구 비율이 재발 없는 잔존율의 의미 있는 예후 인자19 로 확인되었으며, 5년 재발 없는 생존율은 높은 호중구/림프구 비율(≥2.5)을 가 진 환자에서 의미 있게 낮았으며(86.5% vs. 96.7%, p=0.006) 높은 혈소판/림 프구 비율(≥130)을 가진 환자도 낮았다. (89.4% vs. 96.8%, p=0.022) 다변량 분석에서는 종양크기(p<0.001), T 병기(p<0.001), Fuhrman 등급(p=0.015), 술 전 적혈구 수(p=0.026)가 5년 재발 없는 생존율의 독립적인 예후 인자로 확 인되었다. 결론: 비전이 투명 신세포암 환자의 수술 전 호중구/림프구 비율과 혈소판/림프 구 비율의 증가는 높은 재발률과 연관이 있었으나 독립적인 예후 인자는 아니다. 핵심어: 신장암, 염증, 예후 인자