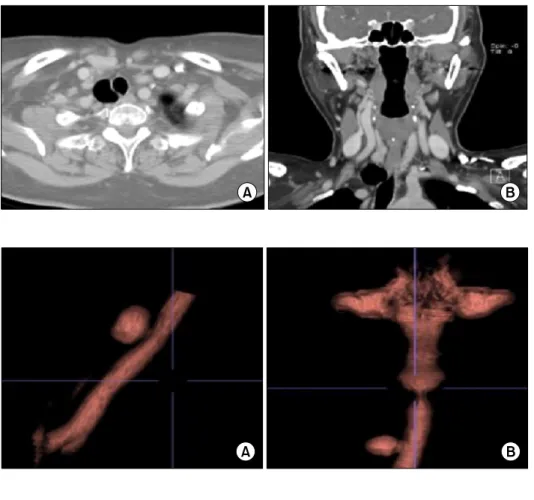
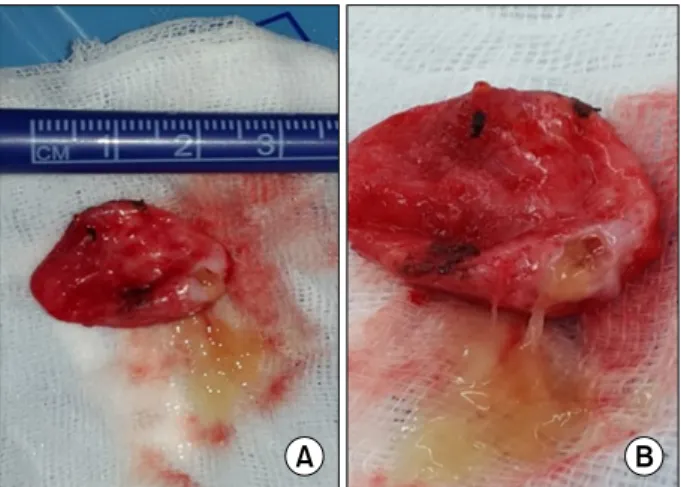
A Case of Symptomatic Tracheal Diverticulum and Surgical Resection as a Treatment Modality
3
0
0
전체 글
(2)
(3)
수치
관련 문서
It considers the energy use of the different components that are involved in the distribution and viewing of video content: data centres and content delivery networks
Post-surgical use of radioiodine (131I) in patients with papillary and follicular thyroid cancer and the issue of remnant ablation: a consensus
After first field tests, we expect electric passenger drones or eVTOL aircraft (short for electric vertical take-off and landing) to start providing commercial mobility
Elevated body mass index as a causal risk factor for symptomatic gallstone disease: a Mendelian randomization study.. Banim PJ, Luben RN, Bulluck
Elevated body mass index as a causal risk factor for symptomatic gall- stone disease: a Mendelian randomization study.. Banim PJ, Luben RN, Bulluck
1 John Owen, Justification by Faith Alone, in The Works of John Owen, ed. John Bolt, trans. Scott Clark, "Do This and Live: Christ's Active Obedience as the
Method We obtained blood samples from 49 patients who underwent surgical treatment for esophageal squamous cell cancer (ESCC) We performed ctDNA analysis with
Conclusion : The treatment using facet joint block with lumbar surgical operation seems to have short term clinical effects, however can't prevent
