Original Article Korean J Urogenit Tract Infect Inflamm 2014;9(1):44-49
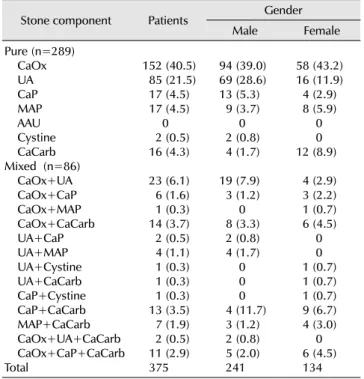
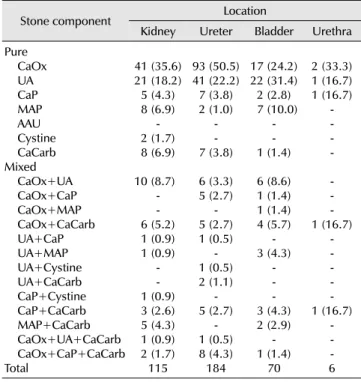
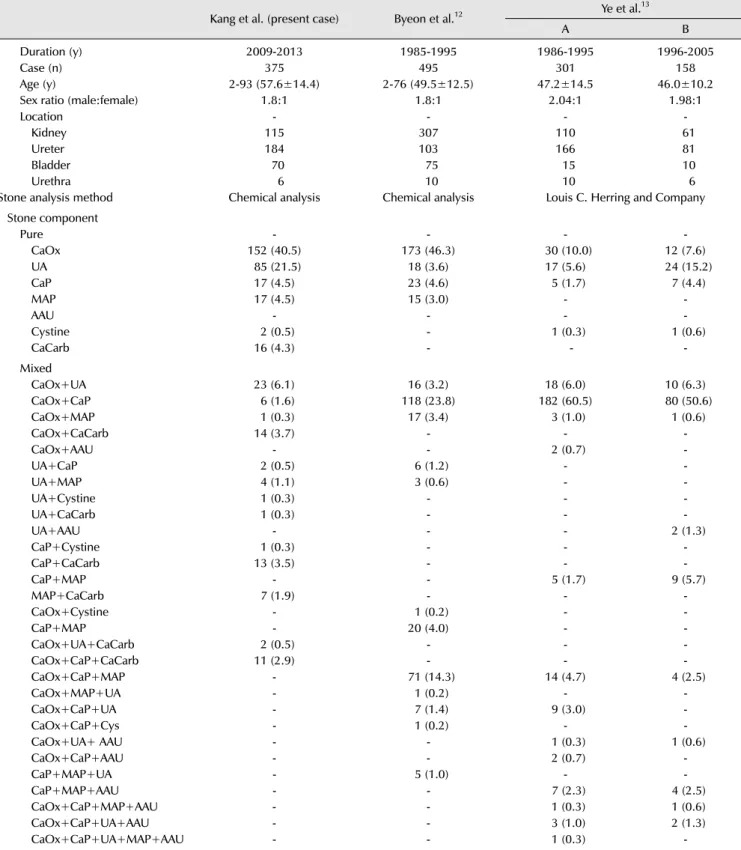
요로결석의 성분분석: 최근 5년간 단일기관 분석 결과(2009년- 2013년)
강필문, 서원익, 강동일
인제대학교 의과대학 비뇨기과학교실
전체 글
인제대학교 의과대학 비뇨기과학교실
수치
관련 문서
Season, sex, age, and education as modifiers of the effects of outdoor air pollution on daily mortality in Shanghai, China: The Public Health and Air Pollution in Asia
In the late nineteenth century, although the proportion of ether was increased and that of chloroform decreased due to the raised awareness of the high
The foreign policy triumphs with China and the Soviet Union and the administration’s announcement that peace “is at hand” in Vietnam helped reelect Nixon as
Comparison of clinical risk factors and distribution of age, sex of patients aged ≧80 years and <80 years... Comparison of the stroke subtype and thrombolysis of
Drug-intoxicated patients were predominantly male, with the highest incidence of intoxication among patients above the seventh decade of age(21.5%) and the
- Renewable E, waste recycling, technology / industrial clusters, infrastructure integrated design Underground transportation
First, after the Group Art Therapy, the scale of hopelessness depression in the test group decreased significantly in comparison with that before the group
With these results, we can suggest the hypothesis that increased cardiac output in the patients who administered ketamine increased muscle blood flow, and this is the
