Korean Journal of HBP Surgery □ 증 례 □
Vol. 15, No. 1, February 2011
62
Renoportal Anastomosis in Living Donor Liver Transplantation; An Effective Technique for Patient
with Diffuse Portal Vein Thrombosis and Large Splenorenal Shunts
End-stage liver disease is often accompanied by portal vein thrombosis (PVT) and large spontaneous splenorenal shunts (SRS). Recently, renoportal anastomosis (RP-A) of spontaneous splenorenal shunts in liver transplantation was reported as an effective method of portal vein reconstruction in cases of PVT with SRS. Here we report a successful case of RP-A in living donor liver transplantation (LDLT). A 46-year–old female with a large spontaneous splenorenal shunt and a portal vein thrombosis propagated to the superior mesenteric vein underwent living donor liver transplantation. At the operation, a side-to-end renoportal anastomosis was done using an interposing cadaveric iliac vein graft. Adequate portal venous blood flow was demonstrated by intraoperative and postoperative Doppler ultrasound studies. She has recovered well with normal graft function and renal function. Renoportal anastomosis for patients with large splenorenal shunts and expansive portal vein thrombosis to the superior mesenteric vein can be an effective and safe technique in patients PV thrombectomy.
Joo Dong Kim, M.D., Dong Lak Choi, M.D., Young Seok Han, M.D.
Department of Surgery, Daegu Catholic University College of Medicine
Corresponding Author Dong Lak Choi
Department of Surgery, Daegu Catholic University College of Medicine, 3056-6, Daemyung 4-dong, Nam-gu, Daegu 705-708, Korea
Tel: +82-53-650-4063 Fax: +82-53-650-4950 E-mail: [email protected]
Key Words : Renoportal anastomosis, Portal vein thrombosis, Splenorenal shunt, Living donor liver transplantation
Received: 2010. 12. 12 Accepted: 2011. 1. 10
Introduction
End-stage liver disease is often accompanied by portal vein (PV) stenosis or thrombosis and large spontaneous splenorenal shunts (SRS). In the early period of LT, PVT was considered a relative contraindication for operation because of technical difficulties.1,2 But many innovative surgical techniques have been introduced in recent years such as thrombectomy, PV reconstruction using vein grafts, and cavoportal hemitransposition.1 But, these procedures are associated with rethrombosis, high mortality rate and
not feasible when PV is complete occluded or propagated to the SMV.2,3
As the technique to solve this problem, renoportal anastomosis (RP-A) has been reported to be effective method in deceased donor liver transplantation (DDLT) and living donor liver transplantation (LDLT).4-7 We report a successful case of LDLT using side to end RP-A as PV reconstruction in PV thrombosis and large SRS.
Case Report
A 46-year-old woman was referred to our institution for
Joo Dong Kim, et al:Renoportal Anastomosis in Living Donor Liver Transplantation
63
Fig. 1. Preoperative image of the case. (A) Liver dynamic CT shows that PV is completely obstructed and PV thrombosis propagated to SMV (arrow). (B) Marked dilated SRS (arrow) is drained into the left renal vein (arrow head).
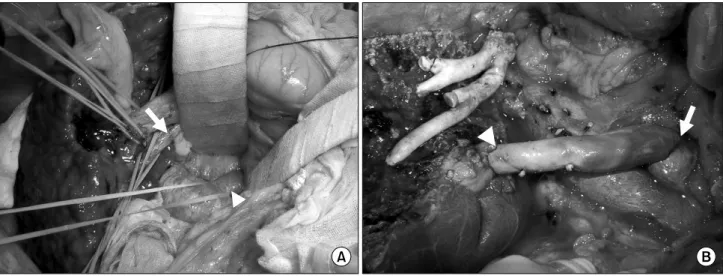
Fig. 2. Surgical procedures for RP-A. (A) After hepatic hilum dissection and Kocher maneuver, the thrombosed PV is exposed (arrow) and the LRV is encircled by umbilical tape (arrow head). (B) Interposition graft is anastomosed to upper border of LRV (arrow) and the Graft PV is anastomosed to proximal end of the interposition graft (arrow head).
liver cirrhosis due to hepatitis B.
Preoperative abdominal computed tomography (CT) showed PV thrombosis propagated to SMV, PV complete occlusion and a large spontaneous SRS (Fig. 1). LDLT using modified right lobe graft from her son was performed.
At exploration, we found thrombosed residual PV after dissection of hepatoduodenal ligament (Fig. 2A). PVT has severe phlebosclerotic change and so, thrombectomy was impossible. The left renal vein (LRV) was exposed with
Kocher maneuver and encircled with umbilical tape. LRV was mobilized toward the left renal hilum and vascular clamps were applied between the IVC wall of LRV origin level and the opposite side toward left renal hilum. The LRV was incised along the upper border and was anastomosed to the lower end of the interposition cadaveric iliac vein graft. After removal of the recipient’s liver, donor’s right hepatic vein of graft was anastomosed to recipient’s hepatic vein. The graft’s PV was anastomosed
한국간담췌외과학회지:제15권 1호 2011
64
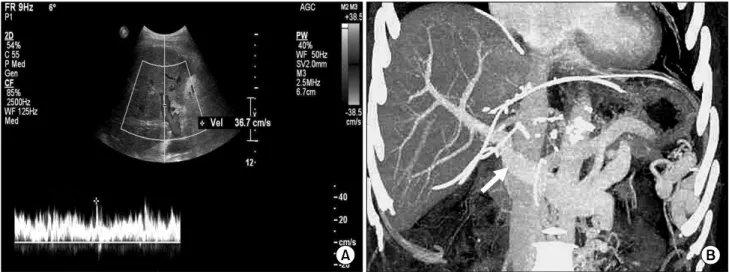
Fig. 3. Imaging studies after LDLT. (A) Postoperative Doppler ultrasonography shows satisfactory portal blood flow in the liver graft. (B) The RP-A is patent and no signs of portal vein system stenosis are visible in Liver dynamic CT at the 14th postoperative day. Interposition vessel graft are indicated by arrow.
to the proximal end of the interposition graft using an appropriate length (Fig. 2B). The graft was reperfused and then the anastomosis between the segment 5/8 outflow and the recipient’s middle-left hepatic vein was performed. The junction of LRV to IVC was occluded with vascular stapler.
Intraoperative Doppler assessment showed adequate PV blood flow. The PV patency was examed by regular Doppler monitoring and computed tomography (Fig. 3).
The patient was discharged postoperative 3 weeks without any complication and has been doing well for 13 months with normal graft function.
Discussion
Spontaneous SRS was first described in the 18th century as a type of portosystemic shunt. Although the incidence of SRS has not been clearly identified, several authors have described its incidence to be between 5 to 12% in cirrhotic patients.7,8 Patients with large SRS, because of their hemodynamic characteristics that superior mesenteric venous flow easily leaks to large collaterals, resulting in a reduced or reversed flow in the PV.5 It is often difficult to apply a conventional technique to such patients with SRS under the situation of LDLT.3,7 Therefore, some techniques
like direct ligation of SRS, LRV ligation, and/or splenectomy may be needed to prevent portal flow steal.5 However, division or ligation of the shunts markedly increase the complexity of the procedure and the splenectomy may have a adverse effect in host defence.4,6
Large SRS often accompanied by PV thrombosis. Since the successful bypass of thrombotic segments using vein grafts, many authors have reported that liver transplantation is feasible even in the presence of PV thrombosis.5,7 Nevertheless, the incidence of PV rethrombosis after liver transplantation has been reported to be as high as 6.6%
with high mortality rate by a meta-analysis.8 Other proce- dures such as ligation of LRV, PV thrombectomy, PV plasty have been reported to the effective procedure at the patients wth large spontaneous SRS.9 But, in cases of phlebosclerotic obstruction or extensive thrombosis to the SMV, complete thrombectomy and/or PV plasty is usually impossible because thrombectomy could develop PV wall damage.7
To solve these underlying problems, RP-A for patients with a surgical SRS in DDLT was first described by Kato et al. in 2000. They described that the method is simple, does not require splenectomy, provides adequate blood flow to the PV, and does not require venous jump graft
Joo Dong Kim, et al:Renoportal Anastomosis in Living Donor Liver Transplantation
65 in patients with PV thrombosis.4 First RP-A in LDLT was reported by Miyamoto et al. and Marubashi et al.5,6 described 3 RP-A cases in LDLT. Moon et al.7 reported 5 RP-A cases in LDLT and introduced S-to-E anastomosis technique in RP-A. They preferred S-to-E RP-A to E-to-E RP-A for several advantages such as less blood requirement, technical feasibility and better operation field due to maintenance of left renal vein continuity.7 Also we could perform S-to-E RP-A without technical difficulty.
RP-A in LDLT recipients also requires an appropriate interposition graft to connect the LRV to the PV of liver graft. Marubashi et al. used internal jugular vein auto-graft, but additional incision to the neck of the recipient can harm cosmesis and cause some neurological sequels.7,10 Hence, Moon et al.7 used variable types of cadaveric vessel graft including iliac vein, IVC, aorta etc. and they have more advantages to make a wide anastomosis venting augmented portal venous flow than internal jugular vein graft.
An RP-A in LDLT could be the most appropriate treatment for patients with PV thrombus and a large SRS according to Marubashi et al.5 But, in our center, PV thrombectomy and interruption of SRS including ligation of LRV was tried preferentially in cases of PV thrombosis and SRS. However, in this patient, PV is completely obstructed by severe phlebosclerotic change and expanded to SMV and therefore, we could not perform PV thrombectomy.
In conclusion, RP-A for patients with large SRS could be an effective and safe technique in cases that be unable to thrombectomy due to severe phleboselerotic change or expansive PV thrombosis to the SMV. It could be considered as the treatment option for patients with diffuse PV thrombosis with large SRS.
References
1. Orlando G, De Luca L, Toti L, et al. Liver transplantation in the presence of portal vein thrombosis: report from a single center. Transplant Proc 2004;36:199-202.
2. Manzanet G, Sanjuán F, Orbis P, et al. Liver transplantation in patients with portal vein thrombosis. Liver Transpl 2001;7:125-131.
3. Cescon M, Sugawara Y, Kaneko J, Ohtsuka H, Takayama T, Makuuchi M. Restoration of portal vein flow by splenorenal shunt ligation and splenectomy after living-related liver transplantation. Hepatogastroenterology 2001;48:1453-1454.
4. Kato T, Levi DM, DeFaria W, Nishida S, Tzakis AG. Liver transplantation with renoportal anastomosis after distal splenorenal shunt. Arch Surg 2000;135:1401-1404.
5. Marubashi S, Dono K, Nagano H, et al. Living-donor liver transplantation with renoportal anastomosis for patients with large spontaneous splenorenal shunts. Transplantation 2005;
80:1671-1675.
6. Miyamoto A, Kato T, Dono K, et al. Living-related liver transplantation with renoportal anastomosis for a patient with large spontaneous splenorenal collateral. Transplantation 2003;75:1596-1598.
7. Moon DB, Lee SG, Ahn CS, et al. Technical modification of reno-portal anastomosis in living donor liver transplantation for patients with obliterated portal vein and large sponta- neous splenorenal shunts. Hepatogastroenterology 2008;55:
2193-2199.
8. Robles R, Fernandez JA, Hernández Q, et al. Eversion thromboendovenectomy in organized portal vein thrombosis during liver transplantation. Clin Transplant 2004;18:79-84.
9. Lee SG, Moon DB, Ahn CS, et al. Ligation of left renal vein for large spontaneous splenorenal shunt to prevent portal flow steal in adult living donor liver transplantation. Transpl Int 2007;20:45-50.
10. Rolffs J, Schmelzle R. Serious cerebral complications follow- ing unilateral ligation of the internal jugular vein. Review of the literature and a case report. J Maxillofac Surg 1977;5:
118-123.