www.kafm.or.kr
122
INTRODUCTION
In Korea, there has been an improvement in thyroid nodule detection through ultrasonography (US) owing to advancements in imaging tech- nologies and growth in the field of health screening.1,2) Multiple guide- lines for thyroid nodules recommend that serum thyrotropin (TSH) lev- els be measured during the initial evaluation of a patient with clinically
or incidentally discovered thyroid nodules (strong recommendation, moderate-quality evidence).3-5) However, despite the high prevalence of thyroid nodules detected on US exams,6-9) little is known about the rela- tionship between the presence of thyroid nodules on US and thyroid function test (TFT) results; hence, the present study aimed to evaluate this relationship.
Received July 25, 2017 Revised August 18, 2017 Accepted August 18, 2017
Corresponding author Soo Hyoung Lee Tel: +82-2-2276-8621, Fax: +82-2-2276-8504 E-mail: [email protected]
ORCID: http://orcid.org/0000-0002-0064-0388
Copyright © 2019 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons At- tribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Brief
Communication
https://doi.org/10.21215/kjfp.2019.9.1.122 eISSN 2233-9116
Korean J Fam Pract. 2019;9(1):122-124
Korean Journal of Family Practice
KJFP
건강한 사람들에게서 초음파로 발견한 갑상선 결절과 갑상선 기능 검사 사이의 관계
정혜진1, 문용식1, 김무영1, 이수형1,*, 박기현1, 김현준1, 황인영1, 손윤정1, 김태호2
1서울의료원 가정의학과, 2서울의료원 내분비대사내과
The Relationship between Thyroid Nodules Detected through Ultrasonography and Thyroid Function Test Results in Healthy Individuals
Hye Jin Jeong1, Yong Sik Moon1, Moo Young Kim1, Soo Hyoung Lee1,*, Ki Hyun Park1, Hyun Joon Kim1, In Young Hwang1, Youn Jung Son1, Tae Ho Kim2
Departments of 1Family Medicine, 2Endocrinology, Seoul Medical Center, Seoul, Korea
Background: The detection of thyroid nodules through ultrasonography (US) has improved with the development of imaging technologies and thyroid cancer screening in Korea. We evaluated the relationship between the presence of thyroid nodules on US and thyroid function test (TFT) results in healthy individuals.
Methods: We performed a retrospective review of data from 449 adults (313 men and 136 women) who underwent tests to evaluate serum thyrotropin (TSH) and free thyroxine levels, thyroid US, and if needed, fine needle aspiration cytology (FNAC).
Results: Of the 449 subjects, 144 subjects (32.1%) had thyroid nodules. Among the 144 with thyroid nodules, 24 (16.7%) were advised to undergo FNAC, and all of them showed normal serum TSH levels. Logistic regression analysis showed that the presence of thyroid nodules was not related to abnormalities noted on TFTs after adjusting for age, sex, smoking status, and presence of risky drinking behavior and hypertension (P=0.647).
Conclusion: The presence of thyroid nodules on US in healthy adults was not associated with abnormal TFT results. Serum TSH check-ups during the evaluation of thyroid nodules discovered through US in asymptomatic individuals living in areas with a low prevalence of autonomous functioning thyroid nodules might not be necessary from the perspective of cost-effectiveness and subject convenience.
Keywords: Thyroid Nodules; Ultrasonography; Thyroid Function Tests; Thyrotropin
www.kafm.or.kr 정혜진 외. 갑상선 결절과 갑상선 기능 검사
Korean J Fam Pract. 2019;9(1):122-124 123
Korean Journal of Family Practice
KJFP
METHODS
1. Study subjects
We retrospectively reviewed the general health check-up database of a health promotion center in Seoul Medical Center. Study subjects were 451 healthy Korean adults who underwent cancer screening between January 1, 2014 and June 30, 2014. All subjects underwent thyroid US and tests to examine TSH and free thyroxine (free T4) levels. Two patients who had undergone total thyroidectomy were excluded. Data on hyper- tension, diabetes, smoking status, and alcohol-drinking behavior were collected through questionnaires. This study was approved by the Insti- tutional Review Board of Seoul Medical Center (2017-02-005).
2. Thyroid ultrasonography and thyroid function tests Thyroid US was performed using a Logos EUB7500 device (Hitachi, Tokyo, Japan) with linear-array probe (13 MHz). Thyroid nodules were classified into three categories: <5 mm, 5–10 mm, and >10 mm, accord- ing to the maximum diameter of the largest nodule. Ultrasound-guided fine needle aspiration cytology (FNAC) was performed when suspicious US findings were observed. Serum TSH and free T4 levels were measured using chemiluminescence immunoassays; the normal range of TSH was 0.35–4.94 uIU/mL and that of free T4 was 0.70–1.50 ng/dL. If either the TSH or free T4 level was abnormal, subjects were classified into the ab- normal TFT group.
3. Statistical analysis
General subject characteristics were compared using Pearson’s chi- squared test or Fisher’s exact test for categorical variables, and using the independent samples t-test or Mann-Whitney U-test for continuous vari- ables. To examine whether there was an independent relationship be- tween thyroid nodules and function, multiple logistic regression analysis was performed. Statistical analyses were performed using PASW Statis- tics 18.0 software (IBM Co., Armonk, NY, USA).
RESULTS
1. General characteristics based on the presence of thyroid nodules
Of the 449 subjects, 144 patients (32.1%) had thyroid nodules. The mean age of the group with thyroid nodules was significantly higher than that of the group without thyroid nodules (51.55±8.68 years vs.
47.54±9.89 years, P<0.001). The other baseline features, such as sex, smok- ing status, alcohol-drinking behavior, presence of hypertension or diabe- tes, and TSH and free T4 levels, were not associated with the presence of thyroid nodules (Table 1).
2. Abnormal TFT results based on the presence of thyroid nodules, nodular size, and FNAC recommendation
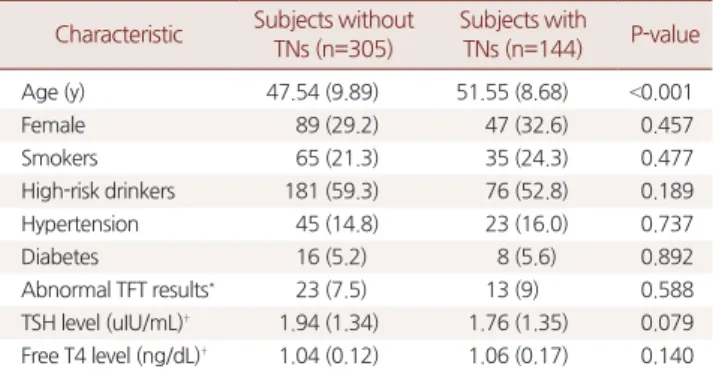
The proportion of individuals with abnormal TFT results did not dif- fer according to the presence of thyroid nodules and nodular size (P=0.588, P=0.932, respectively) (Table 2). Logistic regression analysis Table 1. Characteristics of study subjects
Characteristic Subjects without TNs (n=305)
Subjects with TNs (n=144) P-value
Age (y) 47.54 (9.89) 51.55 (8.68) <0.001
Female 89 (29.2) 47 (32.6) 0.457
Smokers 65 (21.3) 35 (24.3) 0.477
High-risk drinkers 181 (59.3) 76 (52.8) 0.189
Hypertension 45 (14.8) 23 (16.0) 0.737
Diabetes 16 (5.2) 8 (5.6) 0.892
Abnormal TFT results* 23 (7.5) 13 (9) 0.588
TSH level (uIU/mL)† 1.94 (1.34) 1.76 (1.35) 0.079 Free T4 level (ng/dL)† 1.04 (0.12) 1.06 (0.17) 0.140 TNs, thyroid nodules; TFT, thyroid function test; TSH, thyrotropin; Free T4, free thyroxine.
Values are presented as mean±standard deviation or number (%).
P-values were calculated using an independent samples t-test (continuous vari- ables) or Pearson's chi-squared test or Fisher's exact test (categorical variables).
*If either TSH or free T4 levels were abnormal, patients were classified into the abnormal TFT group. †Both TSH and free T4 levels showed deviations from a normal distribution; therefore, the Mann-Whitney U-test was performed.
Table 2. Relationship between the presence of thyroid nodules and TFT results
Variable Normal TFT Abnormal TFT* P-value
TNs 413 36
Presence 131 (90.9) 13 (10.1) 0.588
Absence 282 (92.4) 23 (7.6)
TNs size (mm) 131 13
<5 44 (89.8) 5 (10.2) 0.932
5–10 59 (90.8) 6 (9.2)
>10 28 (93.3) 2 (6.7)
TFT, thyroid function test; TNs, thyroid nodules.
Values are presented as number only or number (%).
P-values were calculated using Pearson's chi-squared test or Fisher's exact test.
*If either thyrotropin (TSH) or free thyroxine (T4) levels were abnormal, patients were classified into the abnormal TFT group. The normal reference range of TSH is 0.35–4.94 uIU/mL and that of free T4 is 0.70–1.50 ng/dL.
Brief
Communication
Korean Journal of Family Practice
Hye Jin Jeong, et al. Thyroid Nodules and Thyroid Function Test Results
www.kafm.or.kr
124 Korean J Fam Pract. 2019;9(1):122-124
Korean Journal of Family Practice
KJFP
showed that the presence of thyroid nodules was not related to abnormal TFT results after adjusting for age, sex, smoking status, risky drinking behavior, and presence of hypertension (P=0.647). Among 144 individu- als with thyroid nodules, 24 were advised to undergo FNAC; 3 showed cytological malignancy but all of them showed normal TFT findings.
DISCUSSION
Our study showed that the presence of thyroid nodules on US did not affect thyroid function results in healthy individuals. Although serum TSH is well-known to be a growth factor for thyroid nodules,10) its levels did not show any relationship with the presence of thyroid nodules in as- ymptomatic individuals.
A previous study demonstrated that autonomous functioning thyroid nodules (AFTN) comprise approximately 12% of all thyroid nodules.11) However, in our study, 6 patients (4.2%, 6/144) showed low TSH levels and only 1 (0.7%, 1/144) had overt hyperthyroidism. As AFTN occur more frequently in iodine-deficient areas,12-14) this low prevalence could be explained by the fact that our study subjects might have been healthy and had normal iodine levels.
The correlation between thyroid nodule size and TSH levels was not significant (P=0.747). A previous study15) suggested that TSH levels were not effective in assessing the presence of AFTN when the nodule size was small, because thyrotoxicosis was rare with nodules sized less than 2.5 cm. Most thyroid nodules in our study were small, sized less than 1.5 cm.
Our study had several limitations. First, our results cannot be applied to the general Korean population due to some selection bias and the small number of study subjects. Second, patient history and physical ex- amination results could not be obtained owing to the limitations of the health check-up system.
In conclusion, our study showed that the presence of thyroid nodules discovered through US in healthy individuals was not associated with TFT findings. TSH check-ups during the evaluation of thyroid nodules discovered through US in asymptomatic individuals living in areas with a low prevalence of AFTN might not be necessary from the perspective of cost-effectiveness and patient convenience.
REFERENCES
1. Suk JH, Kim TY, Kim MK, Kim WB, Kim HK, Jeon SH, et al. Prevalence of ultrasonographically-detected thyroid nodules in adults without previous history of thyroid disease. J Korean Endocr Soc 2006; 21: 389-93.
2. Kim WJ, Kim JH, Park DW, Lee CB, Park YS, Kim DS, et al. Prevalence of thyroid nodules detected by ultrasonography in adults for health check-ups and analysis of fine needle aspiration cytology. J Korean Endocr Soc 2008;
23: 413-9.
3. Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid 2016; 26: 1-133.
4. Gharib H, Papini E, Paschke R, Duick DS, Valcavi R, Hegedüs L, et al. Ameri- can Association of Clinical Endocrinologists, Associazione Medici Endocri- nologi, and European Thyroid Association medical guidelines for clinical practice for the diagnosis and management of thyroid nodules. J Endocrinol Invest 2010; 33(5 Suppl): 1-50.
5. Yi KH, Lee EK, Kang HC, Koh Y, Kim SW, Kim IJ, et al. 2016 revised Korean Thyroid Association management guidelines for patients with thyroid nod- ules and thyroid cancer. Int J Thyroidol 2016; 9: 59-126.
6. Carroll BA. Asymptomatic thyroid nodules: incidental sonographic detec- tion. AJR Am J Roentgenol 1982; 138: 499-501.
7. Brander A, Viikinkoski P, Nickels J, Kivisaari L. Thyroid gland: US screening in a random adult population. Radiology 1991; 181: 683-7.
8. Ezzat S, Sarti DA, Cain DR, Braunstein GD. Thyroid incidentalomas. Preva- lence by palpation and ultrasonography. Arch Intern Med 1994; 154: 1838- 40.
9. Jiang H, Tian Y, Yan W, Kong Y, Wang H, Wang A, et al. The prevalence of thyroid nodules and an analysis of related lifestyle factors in Beijing com- munities. Int J Environ Res Public Health 2016; 13: 442.
10. Polyzos SA, Kita M, Efstathiadou Z, Poulakos P, Slavakis A, Sofianou D, et al.
Serum thyrotropin concentration as a biochemical predictor of thyroid ma- lignancy in patients presenting with thyroid nodules. J Cancer Res Clin On- col 2008; 134: 953-60.
11. Hurtado-López LM, Monroy-Lozano BE, Martínez-Duncker C. TSH alone is not sufficient to exclude all patients with a functioning thyroid nodule from undergoing testing to exclude thyroid cancer. Eur J Nucl Med Mol Im- aging 2008; 35: 1173-8.
12. Belfiore A, Sava L, Runello F, Tomaselli L, Vigneri R. Solitary autonomously functioning thyroid nodules and iodine deficiency. J Clin Endocrinol Metab 1983; 56: 283-7.
13. Baltisberger BL, Minder CE, Bürgi H. Decrease of incidence of toxic nodu- lar goitre in a region of Switzerland after full correction of mild iodine defi- ciency. Eur J Endocrinol 1995; 132: 546-9.
14. Georgopoulos NA, Sykiotis GP, Sgourou A, Papachatzopoulou A, Markou KB, Kyriazopoulou V, et al. Autonomously functioning thyroid nodules in a former iodine-deficient area commonly harbor gain-of-function mutations in the thyrotropin signaling pathway. Eur J Endocrinol 2003; 149: 287-92.
15. Cai H, Qiao Y, Xi H, Luo Q, Yuan X, Yang Y, et al. Is TSH necessary for initial assessment of thyroid nodules? Clin Endocrinol (Oxf) 2017; 86: 263-9.