445
경요도전립선절제술의 배뇨개선효과
The Functional Effect of Palliative Transurethral Resection of the Prostate on Lower Urinary Tract Symptoms in Patients with Prostate Cancer
Ho Suck Chung, Chang Min Im, Sun-ouck Kim, Seung Il Jung, Dong Deuk Kwon, Kwangsung Park, Soo Bang Ryu
From the Department of Urology, Chonnam National University Medical School, Gwangju, Korea
Purpose: Voiding dysfunction occurs frequently in patients with prostate cancer. We investigated the functional effect of palliative transurethral resection of the prostate (pTURP) on lower urinary tract symptoms in patients with prostate cancer.
Materials and Methods: We retrospectively assessed all patients who had a pTURP at our institution between 1999 and 2006. Patients with incidental prostate cancer were excluded. In all, 64 patients were enrolled in the study. The International Prostate Symptom Score (IPSS), the quality of life (QoL), the maximal flow rate (Qmax), and the postvoid residual urine volume (PVR) were evaluated before and after 3 months of pTURP. A positive functional outcome was defined as PVR below 100 ml, no additional catheterization, no repeat pTURP, and no development of uri- nary incontinence.
Results: The patients' mean age was 76.32±6.8 years, and their mean prostate volume was 46.38±19.43 g. After pTURP, the mean IPSS improved from 25.83±6.71 to 18.63±5.96, the mean QoL score improved from 4.33±
0.87 to 3.02±0.83, the mean maximal flow rate increased from 6.11±3.68 ml/sec to 14.20±6.30 ml/sec, and the PVR decreased from 153.69±32.03 ml to 41.89±25.35 ml. All voiding parameters showed significant improve- ment (p<0.001). Of the 64 patients, 12 had poor functional outcome after pTURP. The functional improvement rate of pTURP was 81.25%.
Conclusions: The pTURP performed in patients with prostate cancer showed a favorable effect and resulted in significant improvement in voiding dysfunction. In patients with high-stage metastatic prostate cancer or cancer unsuitable for curative therapy, pTURP could be considered as a safe treatment method to improve lower urinary tract symptoms.
(Korean J Urol 2009;50:445-449)
Key Words: Transurethral resection of prostate, Prostatic neoplasms, Treatment outcome
Korean Journal of Urology Vol. 50 No. 5: 445-449, May 2009 DOI: 10.4111/kju.2009.50.5.445
전남대학교 의과대학 비뇨기과학교실 정호석ㆍ임창민ㆍ김선옥ㆍ정승일 권동득ㆍ박광성ㆍ류수방
Received:January 6, 2009 Accepted:April 16, 2009 Correspondence to: Chang Min Im
Department of Urology, Chonnam National University Medical School, 8, Hak-dong, Doung-gu, Gwangju 501-757, Korea TEL: 062-220-6700 FAX: 062-227-1643
E-mail: [email protected]
Ⓒ The Korean Urological Association, 2009
서 론
전립선암은 전세계적으로 남성 비뇨기계 종양 중 가장 흔히 진단되는 암 중의 하나이며,1 최근 우리나라에서도 노 령 인구의 증가, 식생활의 서구화 등과 함께 전립선특이항
원을 포함한 진단 기술의 발달로 전립선암의 발생 빈도가 현저히 증가하고 있다.2,3 전립선 내에 국한된 전립선암은 주로 근치전립선절제술로 치료하나 국소적으로 진행된 혹 은 원격 전이된 전립선암은 방사선 치료, 남성호르몬 차단 요법이나 화학요법을 시행한다. 근치적 치료가 불가능한 전이성 전립선암 환자에서 하부요로증상 및 급성요폐, 방
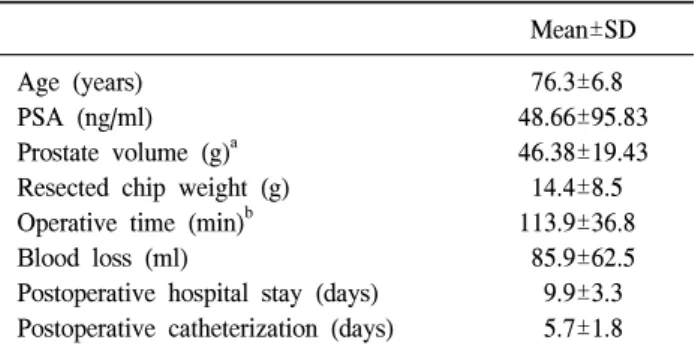
Table 1. Patients characteristics (n=64)
Mean±SD Age (years)
PSA (ng/ml) Prostate volume (g)a Resected chip weight (g) Operative time (min)b Blood loss (ml)
Postoperative hospital stay (days) Postoperative catheterization (days)
76.3±6.8 48.66±95.83 46.38±19.43
14.4±8.5 113.9±36.8
85.9±62.5 9.9±3.3 5.7±1.8 SD: standard deviation, PSA: prostate-specific antigen, a: measured by transrectal ultrasonography, b: palliative transurethral resection of the prostate and bilateral orchiectomy, if it was performed 광결석, 수신증 등을 동반하는 방광출구폐색은 흔한 합병
증으로 나타난다.4,5 전립선비대증에서 방광출구폐색은 수 술적 처치로 경요도전립선절제술 (transurethral resection of the prostate; TURP)이 표준 치료법으로 그 효과에 대하여 널리 알려져 시행되고 있지만6,7 전립선암에서 TURP의 효 과에 대한 연구는 미비한 실정이다. 저자들은 하부요로증 상을 보인 전립선암 환자에게 시행한 고식적 경요도전립선 절제술 (palliative transurethral resection of the prostate; pTURP) 의 기능적 효과를 알아보고자 하였다.
대상 및 방법
1999년 1월에서부터 2006년 12월까지 본원에서 경직장전 립선초음파를 이용한 전립선생검을 통하여 전립선암으로 진단되었으며 급성요폐 혹은 하부요로증상으로 경요도전 립선절제술을 시행 받은 후 1년 이상 추적관찰이 가능하였 던 64명의 환자를 대상으로 의무기록을 통해 수술 시 환자 의 나이, 혈청전립선특이항원 (s-prostate-specific antigen; s- PSA), 경직장전립선초음파에서 전립선용적, 임상적 병기, 절제된 전립선용적, 수술 전후의 국제전립선증상점수, 삶의 질 점수, 최대요속, 잔뇨량을 후향적으로 분석하였다. 대상 환자들은 임상적 병기 cT2 이하인 환자에서 80세 이상의 고령, Eastern Cooperative Oncology Group (ECOG) perfor- mance status의 grade 4 이상, 고혈압, 당뇨, 뇌혈관계질환 등 의 동반 질환 등으로 근치전립선절제술을 시행하지 못한 경우와 임상적 병기가 cT3a 이상인 환자의 경우에 해당되 었다. 또한 수술 후 조직검사에서 우연히 전립선암으로 진 단된 경우는 제외하였다. 수술 후 기능적 성공은 배뇨 후 잔뇨량이 100 ml 이하, 1년 이내에 추가적인 요도 카테터 삽입이나 재수술을 필요로 하지 않으며 요실금이 발생하지 않는 경우로 정의하였다.8-10
수술은 전신마취 또는 경막외 척추마취하에 시행하였다.
수술 전처치, 수술도구 및 절제방법은 전립선비대증에서의 경요도전립선절제술과 동일하였으며 절제 시에 전립선 피 막 가까이는 절제하지 않아 피막천공을 피하였으며 방광출 구폐색을 완화시켜 배뇨통로를 확보할 정도로 시행하였다.
절제된 전립선조직은 무게를 측정한 후 조직 검사를 하였 다. 술 후 22 Fr 도뇨관을 이용하여 세척하였으며 수일 후에 제거하였다.
통계처리는 통계 전문 상용 소프트웨어인 SPSS for windows version 15를 이용하여 국제전립선증상점수, 삶의 질 점수, 최고요속, 잔뇨량의 수술 전후 변화에 대해 paired t-test를 시행하였으며 p 값이 0.05 미만인 경우를 통계학적 으로 유의하다고 판정하였다.
결 과
대상 환자들의 평균연령은 76.3±6.8세, 술 전 평균 전립선 용적은 46.38±19.43 g, 평균 s-PSA는 48.66±95.83 ng/ml, T2 이하이면서 80세 이상의 고령이거나, ECOG performance status의 grade 4 이상, 고혈압, 당뇨, 뇌혈관계질환 등의 동 반 질환을 가진 경우로 근치전립선절제술에 대한 수술적인 위험도가 높은 경우는 30명, 술 전 임상적 병기가 cT3a 이상 은 34명이었다. 절제된 평균 전립선용적은 14.4±8.46 g, 술 후 평균 도뇨관 유치기간은 5.67±1.77일, 평균 입원기간은 9.97±3.29일이었으며 도뇨관을 재유치한 2명을 제외한 나 머지 환자는 도뇨관 제거 후 다음날 자연배뇨 확인 후 퇴원 하였다 (Table 1). 수술 전과 수술 3개월 후의 국제전립선증 상점수는 25.83±6.71점에서 18.63±5.96점으로 감소하였다.
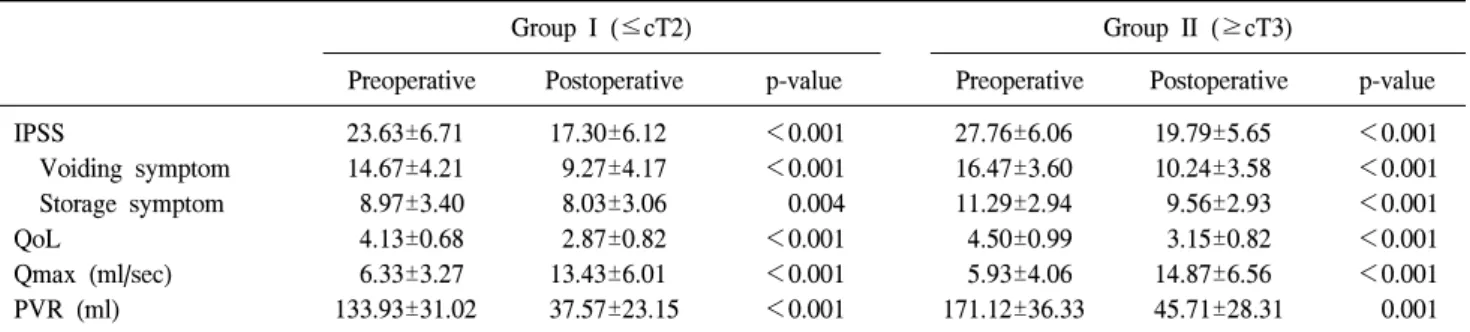
이 중 배뇨증상점수는 15.63±3.97점에서 9.78±3.86점으로, 저장증상점수는 10.20±3.35점에서 8.84±3.06점으로 감소하 였다. 삶의 질 점수는 4.33±0.87점에서 3.02±0.83점으로 감 소하였으며, 최고요속은 6.11±3.68 ml/s에서 14.20±6.30 ml/s 로 증가하였다. 잔뇨량은 153.69±32.03 ml에서 41.89±25.35 ml로 감소하여 모두 통계학적으로 의미있는 향상을 보였다 (p<0.001) (Table 2). 또한 임상적 병기가 cT2 이하인 경우 와 cT3 이상인 경우에서 모두 의의있는 결과를 보였다 (p<
0.05) (Table 3).
술 후 특별한 합병증은 관찰되지 않았으나 배뇨 후 잔뇨 량이 100 ml 이상인 경우는 8례, 이 중에서 도뇨관을 다시 유치한 경우는 2례였다. 재수술을 받은 경우는 5례였는데, 이들은 방광경부로의 전이가 있는 경우 등 진단 당시 임상 적 병기가 cT4 이상인 환자에 해당되었고 평균 13.6±6.1개 월 후에 재수술을 시행하였으며 이 중 3례는 잔뇨가 100 ml 이상이었다. 요실금은 2례에서 발생하였으나 추적기간 중
Table 2. Comparison of the preoperative and postoperative out- comes
Preoperative Postoperative p-value IPSS
Voiding symptom Storage symptom QoL
Qmax (ml/sec) PVR (ml)
25.83±6.71 15.63±3.97 10.20±3.35 4.33±0.87 6.11±3.68 153.69±32.03
18.63±5.96 9.78±3.86 8.84±3.06 3.02±0.83 14.20±6.30 41.89±25.35
<0.001
<0.001
<0.001
<0.001
<0.001
<0.001 IPSS: International Prostate Symptom Score, QoL: quality of life, Qmax: maximal urine flow rate, PVR: postvoid residual urine volume
Table 4. Poor outcomes after palliative transurethral resection of the prostate (n=12)
Poor outcomes Case (%) Postvoid residual urine volume >100 ml
Re-catheterization Re-operatiosna Urinary incontinence
8 (12.5) 2 (3.1) 5 (7.8) 2 (3.1)
a: three patients had postvoid residual volume of >100 ml before re-operation
Table 3. Comparison of the preoperative and postoperative outcomes between the 2 groups
Group I (≤cT2) Group II (≥cT3)
Preoperative Postoperative p-value Preoperative Postoperative p-value IPSS
Voiding symptom Storage symptom QoL
Qmax (ml/sec) PVR (ml)
23.63±6.71 14.67±4.21 8.97±3.40 4.13±0.68 6.33±3.27 133.93±31.02
17.30±6.12 9.27±4.17 8.03±3.06 2.87±0.82 13.43±6.01 37.57±23.15
<0.001
<0.001 0.004
<0.001
<0.001
<0.001
27.76±6.06 16.47±3.60 11.29±2.94 4.50±0.99 5.93±4.06 171.12±36.33
19.79±5.65 10.24±3.58 9.56±2.93 3.15±0.82 14.87±6.56 45.71±28.31
<0.001
<0.001
<0.001
<0.001
<0.001 0.001 IPSS: International Prostate Symptom Score, QoL: quality of life, Qmax: maximal urine flow rate, PVR: postvoid residual urine volume 자연소실 되었다 (Table 4). 연구대상인 64례 중 수술 후 경
과가 좋지 않은 12례를 제외한 52례에서 하부요로증상에 대한 기능적 효과가 있어 고식적 경요도전립선절제술의 기 능적 성공률은 81.25%로 조사되었다.
고 찰
근치적 치료가 불가능한 전이 전립선암 환자에서 하부요 로증상 및 급성요폐, 방광결석, 수신증 등을 동반한 방광출 구폐색은 흔한 합병증으로 관찰되며,4,5 이에 대한 호르몬 치료의 효과는 여러 연구에서 보고되었다. Hand11에 의하면 급성요폐 전립선암 환자에서 호르몬 치료만으로 자연배뇨 가 가능하였다고 하였으며, Chute 등12은 13명의 급성요폐 환자에서 9명이 고환절제술 후 자연배뇨가 가능하였으며, 추적관찰 결과 전립선암의 크기 또한 감소하였다고 보고하 였다. Fleischmann과 Catalona13는 35명의 요폐증상을 보인 전립선암 환자에서 고환절제술을 시행한 후에 24명 (68%) 이 자연배뇨가 가능하였으나, 이 중 절반가량에서는 21일 에서 60일 동안 요도 카테터를 통하여 배뇨하였다고 보고 하였다. 전립선암 환자에서 호르몬 치료는 방광출구폐색을 완화시키고 전립선의 크기를 감소시킬 수 있지만 많은 시
간이 소요된다는 한계점이 있다.14,15 그럼에도 불구하고 최 근까지 고식적 경요도전립선절제술은 수술에 대한 부정적 인 인식으로 전립선암 환자에서 발생한 요폐에 대한 일차 적인 치료 방법으로 고려되지 못하였다.16
Pergament 등17은 전립선암 환자에서 술 중 및 술 후의 출 혈경향과 파종성혈관내응고 (disseminated intravascular coa- gulopathy)의 위험성에 관하여 보고한 바 있으나, 최근 보고 에 의하면 고식적 경요도전립선절제술은 전립선비대증 환 자에서 시행한 경요도전립선절제술과 비교하여 실혈량, 재 원기간, 합병증 등에 의의있는 차이를 보이지 않고 안전하 게 시행될 수 있었으며,18,19 Crain 등19은 전이 전립선암 환자 에서의 수혈은 술 중 실혈에 의한 것보다 술 전 악성빈혈이 원인일 수 있음을 주장하였다.
또한 고식적 경요도전립선절제술이 전립선암의 진행에 부정적인 영향을 미칠 수 있다는 일부 연구결과가 보고되
었으나,20-22 이에 대한 가능성은 명확하지 않으며 근거 또한
충분하지 못하다. Pansadoro 등23은 전립선암에서의 경요도 전립선절제술은 암의 전이를 증가시키지 않는다고 하였으 며, Nativ 등24과 Paul 등25은 전립선 생검을 통하여 진단된 환자와 경요도전립선절제술에 의해 우연히 진단된 전립선 암에서 경요도전립선절제술이 전립선암의 진행에 영향을 미치지 않는다고 주장하였다. 이밖에 여러 연구에서 고식 적 경요도전립선절제술의 긍적적인 결과가 보고되었으며
방광출구폐색이 있는 전립선암 환자에서 안전하게 시행될 수 있다는 것이 입증되었다.26-29
전립선암에 시행한 고식적 경요도전립선절제술의 기능 적 결과에 대하여는 몇몇 연구에서 보고된 바 있다.8-10 Marszalek 등8은 89명의 환자를 대상으로 한 번의 수술 후에 약 75%가 성공적인 결과를 보였으며 평균 2.6년의 추적관 찰기간으로 79%의 환자에서 특별한 문제없이 자연배뇨를 하였다고 하였으며, Gnanapragasam 등9도 46명의 환자 중 약 61%가 술 후 39개월의 추적기간에서 긍정적인 결과를 보였다고 하였다. 본 연구에서는 81.25%의 높은 배뇨개선 효과를 보였고 이러한 성공률의 차이는 몇 가지 원인에 의 한 것으로 생각한다. 저자들의 경우 64명의 환자들 중 43명 에서 고식적 경요도전립선절제술과 고환절제술을 동시에 시행하였고, 방사선치료 후 하부요로증상을 보인 환자는 2 명에 불과하였다. Varenhorst와 Alund14는 요폐가 있는 전립 선암 환자에서 외과적 및 내과적 호르몬치료 모두 효과적 이었으나 고환절제술을 시행한 환자에서 약물치료로만 시 행한 경우보다 자연배뇨까지의 기간이 단축되었다고 하였 으며 Gnanapragasam 등9과 Crain 등10은 방사선 치료가 수술 후 기능적 결과에 부정적인 영향을 줄 수 있다고 보고 한 바 있는데 이와 같은 결과가 본 연구에 영향을 주었을 것으 로 생각한다. 또한 술 후 배뇨기능에 영향을 줄 수 있다고 알려진 호르몬 불응성 전립선암 환자9가 대상에 포함되지 않은 것도 높은 성공률을 보이는 원인으로 생각한다.
이전의 보고에서는 후향적 연구로 인하여 술 전후의 기 능적 결과에 대한 객관적인 자료가 부족하였다.8,9 Mars- zalek 등8은 대부분의 환자들이 수술에 대한 강력한 적응증 을 가지고 있어 국제전립선증상점수 및 요속 검사를 모든 환자에게 시행하지는 못하였다고 하였으며, Gnanapragasam 등9도 수술에 대한 결정이 환자의 증상과 장기간 요도카테 터 유치를 피하기 위한 것이었기 때문에 객관적 자료가 부 족하였다. 그러나 저자들의 경우 환자들의 하부요로증상에 대하여 수술 전후의 국제전립선증상점수, 삶의 질 점수, 최 대요속 및 잔뇨량 검사를 모든 환자들을 대상으로 시행하 였고 수술 전과 후를 비교하였으며 이러한 점이 다른 연구 들과 차별되는 의의로 생각한다. 그러나 일차적인 호르몬 치료 후부터 수술을 시행한 시기까지의 기간에 대한 요인 을 고려하지 않은 것은 본 연구의 한계점으로 생각한다. 저 자들은 술 후 3개월에 시행한 기능적 성공에 대한 결과는 만족스러웠으며 대부분의 환자들은 술 후 배뇨에 대하여 큰 불편감 없이 추적관찰 중이며, 고식적 경요도전립선절 제술을 요하는 전립선암 환자를 예측할 수 있는 술 전 위험 인자에 대한 분석, 전립선암의 진행정도에 따른 술 후 기능 적 결과의 비교분석 역시 연구가치가 있을 것으로 생각한다.
결 론
저자들이 시행한 하부요로증상을 보인 전립선암 환자에 서의 고식적 경요도전립선절제술은 특별한 합병증을 보이 지 않고 81.25%의 높은 성공률을 보였다. 이는 고식적 경요 도전립선절제술이 전립선암의 병기가 높거나 근치적 수술 을 받기 어려운 상태의 전립선암 환자들에게 안전하며 하 부요로증상 완화에 효과적인 치료방법의 하나로 생각한다.
REFERENCES
1. Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Cancer statistics, 2007. CA Cancer J Clin 2007;57:43-66
2. Choe JH, Lee HM, Chai SE, Choi HY. Long-term health- related quality of life in patients with prostate cancer after treatment. Korean J Urol 2004;45:878-89
3. Lee HW, Kwak KW, Choi YH, Choi HY, Lee HM. New thresholds for prostate-specific antigen velocity for prostate cancer screening in Korean patients younger than 60 years old.
Korean J Urol 2008;49:113-7
4. Moul JW, Davis R, Vaccaro JA, Sihelnik SA, Belville WD, McLeod DG. Acute urinary retention associated with prostatic carcinoma. J Urol 1989;141:1375-7
5. Scherr D, Swindle PW, Scardino PT. National Comprehensive Cancer Network guidelines for the management of prostate cancer. Urology 2003;61(2 Suppl 1):14-24
6. Varkarakis J, Bartsch G, Horninger W. Long-term morbidity and mortality of transurethral prostatectomy: a 10-year follow- up. Prostate 2004;58:248-51
7. Djavan B, Madersbacher S, Klingler HC, Ghawidel K, Basharkhah A, Hruby S, et al. Outcome analysis of minimally invasive treatments for benign prostatic hyperplasia. Tech Urol 1999;5:12-20
8. Marszalek M, Ponholzer A, Rauchenwald M, Madersbacher S.
Palliative transurethral resection of the prostate: functional outcome and impact on survival. BJU Int 2007;99:56-9 9. Gnanapragasam VJ, Kumar V, Langton D, Pickard RS, Leung
HY. Outcome of transurethral prostatectomy for the palliative management of lower urinary tract symptoms in men with prostate cancer. Int J Urol 2006;13:711-5
10. Crain DS, Amling CL, Kane CJ. Palliative transurethral prostate resection for bladder outlet obstruction in patients with locally advanced prostate cancer. J Urol 2004;171:668-71 11. Hand JR. Conservative operations for carcinoma of the
prostate: analysis of 109 cases. J Urol 1950;64:123-48 12. Chute R, Willetts AT, Gens JP. Experiences in the treatment
of carcinoma of the prostate with stilbestrol and with castration by the technique of intra-capsular orchiectomy. J Urol 1942;
48:682
13. Fleischmann JD, Catalona WJ. Endocrine therapy for bladder outlet obstruction from carcinoma of the prostate. J Urol 1985;134:498-500
14. Varenhorst E, Alund G. Urethral obstruction secondary to carcinoma of prostate: response to endocrine treatment.
Urology 1985;25:354-6
15. Carpentier PJ, Schroder FH. Transrectal ultrasonography in the follow up of prostatic carcinoma patients: a new prognostic parameter? J Urol 1984;131:903-5
16. Thomas DJ, Balaji VJ, Coptcoat MJ, Abercrombie GF. Acute urinary retention secondary to carcinoma of the prostate. Is initial channel TURP beneficial? J R Soc Med 1992;85:318-9 17. Pergament MC, Swaim WR, Blackard CE. Disseminated
intravascular coagulation in the urological patient. J Urol 1976;116:1-7
18. Madersbacher S, Marberger M. Is transurethral resection of the prostate still justified? BJU Int 1999;83:227-37
19. Crain DS, Amling CL, Kane CJ. Palliative transurethral prostate resection for bladder outlet obstruction in patients with locally advanced prostate cancer. J Urol 2004;171:668-71 20. Hanks GE, Leibel S, Kramer S. The dissemination of cancer
by transurethral resection of locally advanced prostate cancer.
J Urol 1983;129:309-11
21. Bandhauer K. The possible role of transurethral resection in the dissemination of prostatic cancer. Eur Urol 1975;1:272-4 22. Sandler HM, Hanks GE. Analysis of the possibility of that
transurethral resection promotes metastasis in prostate cancer.
Cancer 1988;62:2622-7
23. Pansadoro V, Sternberg CN, DePaula F, Florio A, Giannarelli D, Arcangeli G. Transurethral resection of the prostate and metastatic prostate cancer. Cancer 1991;68:1895-8
24. Nativ O, Bergstralh EJ, Boyle ET Jr, Zincke H. Transurethral resection versus needle biopsy prior to radical prostatectomy for stage C prostate cancer. Influence on progression and survival. Urology 1991;37:22-7
25. Paul R, Knebel C, van Rondenborgh H, Kubler H, Alschibaja M, Gunther M, et al. Incidental carcinoma of the prostate: can we and should we recommend radical prostatectomy? Urologe A 2005;44:1052, 1054-8
26. Levine ES, Cisek VJ, Mulvihill MN, Cohen EL. Role of transurethral resection in dissemination of cancer of prostate.
Urology 1986;28:179-83
27. Paulson DF, Cox EB. Does transurethral resection of the prostate promote metastatic disease? J Urol 1987;138:90-1 28. Meacham RB, Scardino PT, Hoffman GS, Easley JD,
Wilbanks JH, Carlton CE Jr. The risk of distant metastases after transurethral resection of the prostate versus needle biopsy in patients with localized prostate cancer. J Urol 1989;142:320-5
29. Mazur AW, Thompson IM. Efficacy and morbidity of channel TURP. Urology 1991;38:526-8