Korean Circulation Journal
Ventricular Tachycardia Associated Syncope in a Patient of Variant Angina without Chest Pain
Soo Jin Kim, MD, Ji Young Juong, MD, and Tae-Ho Park, MD
Department of Cardiology, Dong-A University Medical Center, Busan, Korea
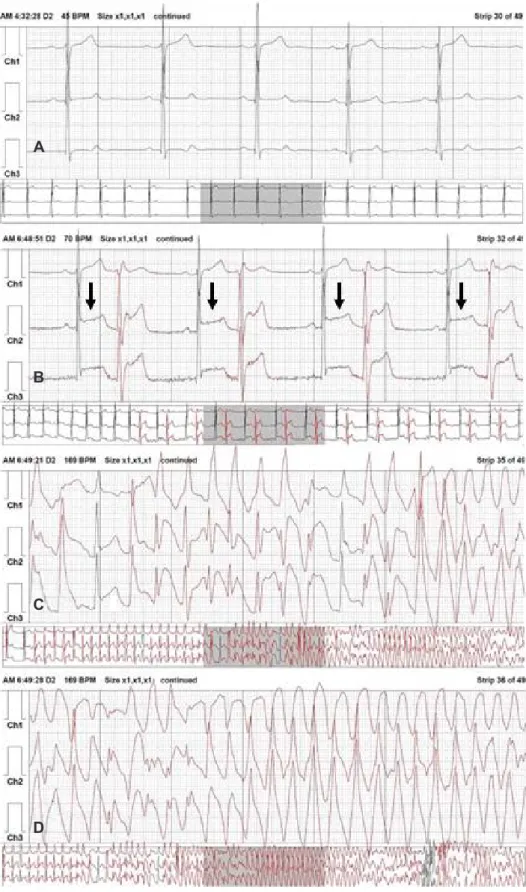
A 68-year-old man was admitted for a syncope workup. After routine evaluation, he was diagnosed with syncope of an unknown cause and was discharged from the hospital. He was readmitted due to dizziness. On repeated Holter monitoring, polymorphic ventricular tachycardia was detected during syncope. We performed intracoronary ergonovine provocation test; severe coronary spasm was induced at 70% stenosis of the proximal left anterior descending artery. The patient was treated with percutaneous coronary intervention. We present a rare case of syncope induced by ventricular arrhythmia in a patient with variant angina without chest pain. (Korean Circ J 2016;46(1):102-106)
KEY WORDS: Prinzmetal’s variant angina; Coronary vasospasm; Tachycardia, ventricular.
Introduction
Variant angina commonly manifests as chest pain and transient ST elevation by coronary spasm, and generally follows a benign clinical course.
1)Rarely, syncope induced by ventricular arrhythmia associated with transient myocardial ischemia can be developed by coronary spasm.
2)3)If the cause of syncope is not correctly diagnosed, patients are at risk of recurrent syncope.
4)In particular, syncope without chest pain is an uncommon manifestation of variant angina. Thus, as in this case, it can be missed as the cause of syncope.
Case
A 68-year-old man visited our emergency room due to recurrent syncope. He had experienced four episodes of syncope with dizziness and chest discomfort during the prior 2 months. The episodes were evoked when he was preparing his boat for sailing in early morning. On admission, his mentality was clear. Vital signs showed blood pressure (BP) of 120/80 mmHg, pulse rate of 60 beats/min, respiratory rate of 20 breaths/min and body temperature of 36.5°C. He had a 10-year history of diabetes mellitus with application of oral hypoglycemic agents. He had stopped smoking 40 years previously. He drank 1 bottle of soju per week. Physical examination, chest radiography and laboratory findings were unremarkable. The initial electrocardiogram (ECG) showed sinus rhythm with T inversion in the V5 and V6 leads. Transthoracic echocardiogram revealed left ventricular hypertrophy, mildly decreased ejection fraction, and hypokinetic left ventricular wall motion. Twenty four hour Holter monitoring showed normal sinus rhythm and infrequent premature ventricular complexes (PVCs).
Coronary angiography revealed 70% stenosis at proximal left anterior descending artery (LAD) (Fig. 1A). Stenosis persisted after intracoronary nitrates administration (Fig. 1B). We planned medical treatment instead of coronary angioplasty. The tilt table test and brain magnetic resonance angiography were unremarkable. The patient was discharged and regarded as an unexplained syncope.
After 4 days, he was readmitted because of severe dizziness and
Print ISSN 1738-5520 • On-line ISSN 1738-5555