DOI 10.17480/psk.2018.62.5.334
ABCB1 C3435T가 신장이식 수혜자에서 tacrolimus의 최저혈중농도에 미치는 영향: 체계적 문헌고찰 및 메타분석
신혜연* · 천부순**,#
*덕성여자대학교 약학대학, **인제대학교 약학대학 인제약학연구소
(Received June 19, 2018; Revised September 5, 2018; Accepted October 18, 2018)
The Effect of ABCB1 C3435T on Blood trough Concentrations of Tacrolimus in Renal Transplant Recipients: a Systematic Review and Meta-analysis
Hye Yeon Sin* and Pusoon Chun**,#
*College of Pharmacy, Duksung Women’s University, Seoul 03169, Republic of Korea
**College of Pharmacy and Inje Institute of Pharmaceutical Sciences and Research, Inje University, 197 Inje-ro, Gimhae, Gyeongnam 50834, Republic of Korea
Abstract — A large number of studies have investigated the influence of ABCB1 C3435T polymorphism on blood trough concentrations of tacrolimus in kidney transplant recipients. However, the results are inconsistent. The aim of the present study was to clarify the effects of ABCB1 C3435T on trough blood levels of tacrolimus in renal transplant recipients at dif- ferent post-transplantation times. The databases of PubMed, Embase, Ovid, and Cochrane Library were searched for all pub- lished studies from inception to March 2018. In addition, reference lists of articles were also examined. Using the Review Manager 5, weighted mean differences of dose-adjusted trough concentration of tacrolimus were pooled to estimate the effects of ABCB1 C3435T on tacrolimus levels. A total of 11 studies (968 recipients) were included in the present meta- analysis. The adult recipients with CC genotype had lower dose-adjusted trough concentration of tacrolimus than the CT and TT carriers at the first week after kidney transplantation (CC vs CT, WMD: -14.82; 95% CI: -24.73, -4.90; p=0.003;
CC vs TT, WMD: -30.73; 95% CI: -47.9, -13.57; p=0.0004). Similar results were observed in adult recipients at the first month after transplantation (CC vs CT, WMD: -19.61; 95% CI: -27.66, -11.56; p<0.00001; CC vs TT, WMD: -25.45; 95%
CI: -47.68, -3.22; p=0.02). Furthermore, at 3 months, the pediatric and adult recipients with CC or CT genotype had lower dose-adjusted trough concentration than the TT carriers (CT vs TT, WMD: -11.85; 95% CI: -18.65, -5.04; p=0.0006; CC vs TT, WMD: -30.98; 95% CI: -37.46, -24.50; p<0.00001). In addition, at the time of 6 months, the adult recipients carrying 3435C allele had lower dose-adjusted trough concentration than the TT carriers (CC vs CT, WMD: -19.00; 95% CI: -23.60, -14.39; p<0.00001; CT vs TT, WMD: -6.57; 95% CI: -12.87, -0.28; p=0.04; CC vs TT, WMD: -26.46; 95% CI: -32.04, -20.88;
p<0.00001). These results imply that the adult recipients carrying ABCB1 3435C allele need higher dose of tacrolimus to prevent acute rejection after kidney transplantation.
Keywords ABCB1 C3435T polymorphism, blood trough concentration, tacrolimus, kidney transplant recipients
서 론 (Introduction)
신장이식(kidney transplantation)은 장기적인 혈액투석에 비해 말기 신부전 환자의 생존율과 삶의 질(quality of life)을 향상시 키는 효과가 우수하며 경제성의 측면에서도 우월한 것으로 보고 되었다.1-3)질병관리본부의 장기이식 통계연보에 의하면 국내 신 장이식 건수는 2011년에 1,639건 이었으며 해마다 증가하여 2016 년에는 2,236건에 달했고 2017년에는 2,162건으로 집계되었다.4) 이처럼 신장이식이 말기 신부전 환자에게 가장 이상적인 치료법
#
Corresponding Author Pusoon Chun
College of Pharmacy and Inje Institute of Pharmaceutical Sci- ences and Research, Inje University, 197 Inje-ro, Gimhae, Gyeo- ngnam 50834, Republic of Korea
Tel.: 055-320-3886 Fax.: 055-320-3940 E-mail: [email protected]
Short Report
종설이며 이식건수가 현저하게 증가하게 된 것은 이식기술과 면역억 제제의 발달 덕분이라고 할 수 있다.5-7)
신장이식 후 발생하는 급성거부반응(acute rejection)은 이식신 (allograft)과 신장 수혜자의 생존율에 영향을 주는 대표적인 인자 이다.8)그러므로, 신장이식 후 면역억제제의 사용은 성공적인 이 식의 핵심요소라 할 수 있으며 calcineurin 억제제인 cyclosporine 혹은 tacrolimus 중 1개, DNA 합성을 방해하여 림프구증식을 억 제하는 약물인 mycophenolate mofetil 혹은 azathioprine 중 1개, 그리고 steroid로 구성된 3제요법이 널리 사용된다.9)
Tacrolimus(FK506)는 Streptomyces tsukubaensis에서 생성된 macrolide계 면역억제제로 세포내 단백 FK-binding proteins와 복합체를 형성한 후 칼슘 및 칼모듈린 의존성 단백인산화 효소 (Ca2+/calmodulin-dependent protein kinase)인 calcineurin과 결 합함으로써 calcineurin의 활성을 억제하여 결국 T-림프구 활성 화를 저해한다.10) Tacrolimus가 cylosporine에 비해 단위 mg당 10-100배 더 강력한 calcineurin 억제효능이 있다고 알려짐에 따 라 tacrolimus의 사용이 꾸준히 증가해 왔음에도 불구하고11)치 료역(therapeutic index)이 좁고 개체 간에 약동학적인 차이가 커 서 tacrolimus의 적정한 혈중농도를 예측하고 유지하는 것은 여전 히 난제가 되고 있다.12)적정 최저혈중농도(trough concentration, C0)보다 낮은 경우 발생하는 급성거부반응과 적정 혈중농도 범위 를 초과하는 경우 발생하는 진전, 두통, 불면 등의 신경독성, 사 구체 손상으로 인한 신장독성 등의 부작용을 예방하기 위해서는 tacrolimus를 투약하는 중에 치료적 약물농도 모니터링(therapeutic drug monitoring, TDM)이 필수적이다.13-15) Tacrolimus의 혈중농 도에 영향을 주는 다양한 인자들이 보고되어왔다. 소아에서 성인 과 유사한 최저혈중농도를 유지하기 위해서는 성인보다 고용량의 tacrolimus를 투여해야 하며, 혈중 albumin 및 hematocrit 수치 가 낮을수록 tacrolimus의 혈중농도가 낮고, 고지방식이는 tacrolimus의 흡수를 감소시키는 것이 관찰되었다.12,16) Tacrolimus 의 생체이용률은 P-당단백질(p-glycoprotein, P-gp)에 의해서도 영 향을 받아 장에서 P-당단백질의 활성이 비정상적으로 높은 경우 tacrolimus의 생체이용률이 감소했다.17)이와 유사하게, 장에서의 ABCB1(MDR1) mRNA 발현이 많을수록 tacrolimus의 투여용량 대비 혈중농도 비(concentration/dose, C/D)가 낮고 급성거부반응 발생률은 높았다.18-20) P-당단백질은 ATP-binding cassette subfamily B member 1(ABCB1) 혹은 multidrug resistance protein 1 (MDR1)이라고도 불리며 에너지 의존성 배출 펌프(energy- dependent efflux pump)로서 다약제내성 기전에 핵심적인 역할을 한다. P-당단백질은 7번 염색체의 장완에 위치하는 것으로 알려 진 ABCB1 (MDR1) 유전자에 의해 인코딩되고 장상피(intestinal epithelium), 간세포, 신장의 근위세뇨관, 혈액뇌장벽(blood-brain barrier) 및 혈액고환장벽의 모세혈관 내피세포 등에 광범위하 게 존재하면서 다양한 약물의 흡수를 억제하거나 배설을 촉진
한다.21,22)
ABCB1 유전자 변이가 소장에서 발현하는 P-당단백질의 양과 활성에 유의한 영향을 미치는 것이 증명됨으로써 개체간 차이가 큰 tacrolimus의 약동학적 특징이 일부 설명되지만23,24) ABCB1 C3435T가 신장이식 수혜자에서 tacrolimus의 혈중농도에 미치는 영향에 관해서는 연구결과들간에 일관성이 없다. ABCB1 C3435T(rs1045642)는 ABCB1 단일염기다형성(single nucleotide polymorphisms, SNPs) 중 발현이 빈번하며 가장 널리 연구된 SNPs 중 하나로서 exon 26에 위치하며 아미노산 서열 변이가 없 는 synonymous SNP이다.25)
Li 등은 메타분석을 통해 신장이식 후 1주일째에 ABCB1 3435CC 유전자형을 가진 수혜자에서의 tacrolimus 최저혈중농 도가 3435CT 유전자형을 가진 수혜자에서의 최저혈중농도보다 낮았으며, 이식 후 6개월째에는 3435CT 유전자형을 가진 수혜 자에서의 최저혈중농도가 3435TT 유전자형을 가진 수혜자에 비 해 낮았다고 발표했다.26)반면, 유사한 시기에 Terrazzino 등이 수행한 메타분석에서는 이식 후 3~6개월이 지난 시점에 ABCB1 3435TT 유전자형을 가진 수혜자에서의 최저혈중농도가 3435CC 혹은 3435CT 유전자형을 가진 수혜자에 비해 미약하지만 오히 려 낮았던 것으로 나타났다.27)
신장이식 수혜자에서 tacrolimus의 혈중농도에 대한 유전자의 영향을 규명하는 것은 이식 후 발생하는 급성거부반응을 예방하 고 이식신과 수혜자의 생존율을 향상시키기 위해 매우 중요하다.
따라서 본 메타분석은 ABCB1 C3435T가 신장이식 수혜자에서 tacrolimus의 혈중농도에 미치는 영향을 규명하고자 수행되었다.
연구 방법 (Methods)
문헌 검색
2018년 3월 현재까지 발표된 모든 출판물을 대상으로 PubMed, Embase, Ovid, Cochrane Library 데이터베이스를 검색하였다. 검 색어로는 ‘ABCB1’, ‘ABC transporter subfamily B’, ‘multidrug resistance protein 1’, ‘MDR1’, 혹은 ‘P-glycoprotein’을 ‘tacrolimus’
와 ‘AND’로 연결하여 사용했으며 문헌의 출판 언어에 제한을 두 지 않았다. 또한, 데이터베이스 검색으로 선택된 문헌 및 선행된 메타분석 논문의 참고문헌을 자료원으로 수기검색을 추가하였다.
문헌 선택
본 연구에 포함할 문헌의 선택과 선택된 문헌으로부터의 자료 추출은 두 명의 연구자가 독립적으로 수행하여 공통으로 선택된 문헌 및 자료를 선정하였으며 의견이 일치 하지 않은 경우는 충 분한 논의를 통해 결정하였다. 신장이식 수혜자에서 ABCB1 C3435T와 tacrolimus의 혈중농도에 관한 연구로서 ABCB1 C3435T 유전자형에 따른 tacrolimus의 ‘체중당 투여용량 대비
최저혈중농도 비(C0/D/kg)’의 평균 차이를 산출 할 수 있는 데이 터를 보여주는 연구를 선택하였다. 반면 종설, 사례보고, 논평, 초록만 발표된 연구, 선행연구의 증보, 유전자형에 따른 tacrolimus 의 용량 조정된 최저혈중농도 차이를 산출할 수 없는 연구, 신장 이식 후 tacrolimus의 혈중농도 관측 기간을 기술하지 않은 연구 는 배제하였다.
자료 추출
신장이식 수혜자에서 tacrlolimus의 최저혈중농도(C0)는 이식 후 급성거부반응의 발생과 유의한 관계가 있으며13,28) 혈중 약물 농도곡선하면적(area under the concentration-time curve)과도 매우 강한 양의 상관관계를 보이므로 tacrolimus의 혈중농도를 모니터링하기 위해 최저혈중농도를 사용하는 것이 타당하다는 연구결과에29)근거하여 본 메타분석은 유전자형에 따른 tacrolimus 의 혈중농도를 평가하기 위한 지표로서 ‘체중당 투여용량 대비 최저혈중농도 비(ng/ml/mg/kg)’를 추출하였다. 또한 동일한 환자 라 하더라도 이식 후 최저혈중농도를 유지하기 위해서는 시간 경 과에 따라 tacrolimus의 투여용량을 감량해야 한다는 연구결과 에30)근거하여 이식 후 tacrolimus의 혈중농도를 측정한 시점별
‘체중당 투여용량 대비 최저혈중농도 비’를 추출하였다. 본 연구 가 추출한 자료는 다음을 포함한다: 피험자의 민족성, 나이, 체중, 성(gender), tacrolimus와 병용된 약물, ABCB1 C3435T 다형성의 빈도, 이식 후 tacrolimus의 혈중농도를 측정한 시점별 ‘체중당 투 여용량 대비 최저혈중농도 비(ng/ml/mg/kg)’.
문헌의 질평가(Quality assessment)
본 연구에 포함된 문헌의 비뚤림 위험을 평가하기 위해 비무작 위연구의 질평가도구인 Newcastle-Ottawa Quality Assessment Scale(NOS)를 사용하였다.31)개개의 연구에 대해 선택(selection) 영역의 4개 문항, 비교가능성(comparability) 영역의 1개 문항, 결 과(outcome) 영역의 3개 문항을 평가하여 0~9점 사이의 점수를 부여했으며 0~3점은 ‘낮음’, 4~6점은 ‘보통’, 7~9점은 ‘우수’로 평가하였다.32)연구의 질 평가는 두 연구자가 독립적으로 수행 하였으며 두 연구자의 평가가 일치하지 못한 경우 충분한 논의 를 통하여 합의된 점수를 부여하였다.
자료의 통합 및 분석
Review Manager Version 5(Cochrane Collaboration, Oxford, United Kingdom)를 사용하여 메타분석을 수행했다. Tacrolimus 의 혈중농도에 대한 ABCB1 C3435T의 영향은 CC vs TT, CC vs CT, CT vs TT로 분석하였으며 ‘체중당 투여용량 대비 최저 혈중농도 비(ng/ml/mg/kg)’의 가중 평균 차이(weighted mean difference, WMD)를 산출하여 통합된 요약 추정치(pooled estimates)를 구하고 95% 신뢰구간(confidence intervals, CIs)으
로 나타내었다. Higgin’s I² 통계량이 50% 미만인 경우 고정효 과모형(fixed effect model)으로, 50% 이상인 경우는 변량효과모 형(random effect model)으로 분석하였다. 요약 추정치는 Z-test 의 P값이 0.05 미만일 때 통계적으로 유의한 것으로 판단하였다.
본 메타분석에 포함된 연구들간의 이질성은 Chisquare-based Q test에 의해 Chi2>df (자유도) 일 때 연구들간 이질성이 있는 것 으로 의심하고 P값이 0.1 미만일 때 통계적으로 유의한 것으로 판정하였다. 연구들간의 이질성은 Higgin’s I² 통계량으로도 분 석하였으며 I²의 값이 25% 미만인 경우 이질성이 ‘없음’으로, 25~50%인 경우 ‘낮음’으로, 50~75%인 경우 ‘중등도’로, 75%
이상인 경우를 ‘높음’으로 해석했다.33,34)출판편향(publication bias)은 funnel plot으로 관찰하였다.
결 과 (Results)
문헌 검색
데이터베이스 검색을 통해 750개의 문헌이 수집되었으며 선행 된 메타분석 논문의 참고문헌 목록을 수동으로 검토하는 과정에 서 찾은 논문 1개가 추가되었다. 제목과 초록을 검토하여 선정 및 배제 기준을 만족하는 195편의 문헌을 1차적으로 선택하고 전문(full-text)을 검토하여 본 메타분석에 포함할 최종 연구를 선 정하였다. 전문을 검토하는 과정에서 본 메타분석에 부적절한 문 헌 184개가 배제되고 최종 11개의 코호트 연구(cohort study)가 선정되었다. 문헌 184개가 배제된 사유는 다음과 같다: 신장이식 수혜자에서 tacrolimus 혈중농도에 대한 ABCB1 C3435T의 영 향에 관한 연구가 아닌 논문 86개, 유전자형에 따른 ‘체중당 투 여용량 대비 최저혈중농도 비’의 평균 차이를 산출할 수 있는 자 료를 보여주지 않는 연구 85개, tacrolimus의 최저혈중농도를 관 측한 명확한 시점을 기술하지 않는 논문 6개, 타 저널에 중복출 판된 연구로서 tacrolimus의 최저혈중농도를 유전자형 TT vs CC+CT로만 관측한 논문 3개, tacrolimus의 최저혈중농도를 유 전자형 CC vs CT+TT로만 관측한 연구 1개, 사례보고 1개, 논 평 1개, 학술대회 발표자료 1개(Fig. 1).
문헌의 질평가
본 연구에 11개의 후향적 코호트 연구가 포함되었다. NOS를 사용하여 문헌의 질평가를 수행한 결과 4개의 연구가35-38) 7점을, 6개의 연구가39-44) 8점을, 1개의 연구가45) 9점을 얻어 비뚤림 위 험이 낮다고 판단하였다.
연구대상의 특징
본 메타분석에 포함된 연구대상은 모두 968명 이었으며 다형 성별로는 ABCB1 3435CC가 332명(34.3%), 3435CT는 440명 (45.5%), 3435TT는 196명(20.2%)이었다. 연구대상의 민족성을
볼 때, 4개의 연구가 아시아 인종을,36,39,41,43) 5개의 연구는 코카 서스(Caucasus) 인종을37,38,40,44,45) 대상으로 하였다. 나머지 2개 연 구에 참여한 피험자는 백인, 흑인, 인도인 등으로 섞여있었다.35,42)
연구대상의 나이를 보면, 2개 연구가 평균연령이 11세 부근인 소 아 코카서스 인종을,37,44)나머지 연구는 모두 성인을 대상으로 하였다. Tacrolimus와 병용한 면역억제제로는, steroid와 함께
Fig. 1 − Flow of the study selection process for a systematic review and meta-analysis.
Table I − Characteristics of the included studies and genotype frequencies of ABCB1 C3435T polymorphism in renal transplant recipients
Study Ethnicity Age (years)
(mean±SD)
Body weight (kg)
(mean±SD) Male/female Immunosuppressive protocol
Genotypes (n)
CC CT TT
Anglicheau et al. 2003 73 White, 7 Black, 1
Indian 40.9±11.3 62.7±13.7 41/40 TAC, AZA/MMF, steroid 29 34 18
Wang et al. 2005* Asian 46±10 68±13 39/47 TAC, AZA, steroid 26 35 23
Zhang et al. 2005 Asian 44.3±15.3 61.6±10.2 90/28 TAC, MMF, steroid 40 55 23
Akbas et al. 2006 Caucasian 37.38±10.74 NR 63/29 TAC, MMF, steroid 28 44 20
Jun et al. 2009* Asian 55.4±11.89 62.8±10.08 377/129 NR except TAC 59 83 30
Turolo et al. 2010* Caucasian 11.6±4.8 NR 56/31 TAC, MMF, steroid 10 10 6
Provenzani et al. 2011 Caucasian 42.94±13.55 NR 26/24 TAC, MMF, steroid 11 26 13
Singh et al. 2011* Mixed 35 (median) 53 (median) 257/43 TAC, AZA/MMF, steroid 17 37 21
Kim et al. 2012 Asian 38.6±11.5 60.1±10.36 79/53 TAC, MMF, steroid 53 68 11
Ciftci et al. 2013 Caucasian 35.47±11.58 60.57±±11.33 47/53 TAC, AZA/MMF, steroid 44 33 23
Shilbayeh et al. 2013 Caucasian
CC: 11.5±2.6 CT: 11.1±3.2 TT: 11.3±3.3
CC: 28.9±7.9 CT: 29.5±11.4 TT: 31.2±12.2
CC: 4/11 CT: 10/5 TT: 3/5
TAC, MMF, steroid 15 15 8
AZA, azathioprine; TAC, tacrolimus; MMF, mycophenolate mofetil; steroid, methylprednisolone/prednisone; NR, not reported; *, data
from the total subjects participated in the study except genotypes
mycophenolate mofetil (MMF)을 사용한 연구가 6개,36-38,40,43,44)
azathioprine (AZA)을 사용한 연구가 1개,39) MMF 혹은 AZA를 사용한 연구가 3개였으며35,42,45)병용한 약물을 기술하지 않은 연 구가41) 1개였다(Table 1).
ABCB1 C3435T가 신장이식 수혜자의 tacrolimus 혈중농 도에 미치는 영향
본 메타분석에 포함된 각 연구의 결과를 ‘신장이식 후 tacrolimus 의 최저혈중농도를 관측한 시점’에 따라 분류한 후 유전형에 따 른 ‘체중당 투여용량 대비 최저혈중농도 비(ng/ml/mg/kg)’의 가중 평균 차이(WMD)를 합성하였다. 또한, 연구대상이 성인으로만 구성된 경우와 소아를 포함한 경우, 아시아 인종인 경우와 코카 서스 인종인 경우로 세분하여 각 그룹에서 ABCB1 C3435T의 영향을 분석하였다.
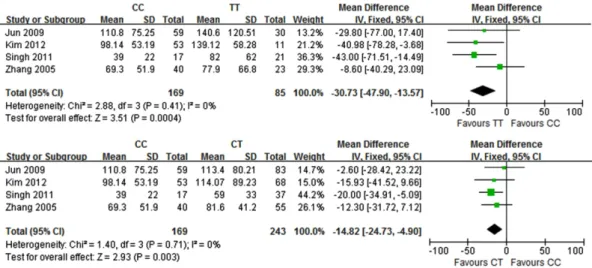
이식 후 1주째에 관측된 영향
이식 후 1주째에 tacrolimus의 최저혈중농도를 관측한 5개의 연구결과를 합성했을 때 3435CC와 3435TT 간에 통계적으로 유 의한 차이가 발견되지 않았다(CC vs TT, WMD: -18.71; 95%
CI: -47.79, 10.36; p=0.21; I2: 79%).36,37,41-43)하지만 소아를 대 상으로 한 Turolo 등의 연구를37)제외하고 성인 대상 연구만으 로 분석했을 때, 3435CC에서의 혈중농도는 3435TT 및 3435CT 에서의 혈중농도에 비해 유의한 수준으로 낮았으며 연구들간 이 질성은 없었다(Fig. 2). 반면, 3435CT와 3435TT 간에 유의한 차 이는 나타나지 않았다(CT vs. TT, WMD: -14.99; 95% CI: - 31.99, 2.02; p=0.08; I2: 0%).36,41-43)
한편, 아시아 인종에서의 영향을 분석했을 때 3435TT 유전형 에 비해 3435CC에서의 혈중농도가 통계적으로 유의한 수준으로
낮았지만 3435CC와 3435CT 간에 차이는 없었다. 3435CT는 또 한 3435TT와도 차이를 보이지 않았다(CC vs. TT, WMD: - 23.75; 95% CI: -45.25, -2.26; p=0.03; I2: 0%; CC vs. CT, WMD: -10.71; 95% CI: -23.98, 2.56; p=0.11; I2: 0%; CT vs.
TT, WMD: -10.59; 95% CI: -31.75, 10.58; p=0.33; I2: 0%).36,41,43)
이식 후 1개월째에 관측된 영향
이식 후 1개월째에 tacrolimus의 최저혈중농도를 관측한 9개 의 연구결과를 결합했을 때 3435CC와 3435TT 간에 통계적으 로 유의한 차이가 발견되지 않았다(CC vs TT, WMD: -19.43;
95% CI: -38.45, -0.41; p=0.05; I2: 77%).35-38,40,42-45)반면, 소아 를 대상으로 한 Turolo 등의 연구와37) Shilbayeh 등의 연구를44) 제외한 후 성인대상 연구만으로 분석했을 때 tacrolimus의 혈중 농도는 3435TT 및 3435CT에 비해 3435CC에서 유의한 수준으 로 낮았다(Fig. 3). 하지만 3435TT와 3435CT 간에 통계적으로 유의한 차이는 없었다(CT vs TT, WMD:-8.18; 95% CI: -18.32, 1.97; p=0.11; I2: 25%).35,36,38,40,42,43,45)
코카서스 인종의 성인 및 소아에서의 영향을 분석했을 때 3435CC와 3435TT 간에 통계적으로 유의한 차이가 없었다(CC vs TT, WMD:-18.81; 95% CI: -52.33, 14.71; p=0.27; I2: 87%).37,38,40,44,45) 반면, 코카서스 인종 성인대상 연구만으로 분석 했을 때는, 3435CC에서의 혈중농도는 3435TT 및 3435CT에 비 해, 3435CT에서의 혈중농도는 3435TT에 비해 유의한 수준으로 낮았다(CC vs. TT, WMD: -40.17; 95% CI: -53.95, -26.39;
p<0.00001; I2: 90%); CC vs. CT, WMD: -19.62; 95% CI:
-33.94, -5.31; p=0.007; I2: 38%; CT vs. TT, WMD: -18.26;
95% CI: -34.64, -1.88; p=0.03; I2: 58%).38,40,45)
Fig. 2 − Forest plots of the association between ABCB1 C3435T polymorphism and dose-adjusted trough concentration of tacrolimus in adult
recipients at the first week after kidney transplantation. Squares represent study-specific weight mean difference (WMD); horizontal
lines represent 95% CIs; diamond represents the summary pooled WMD.
이식 후 3개월째에 관측된 영향
이식 후 3개월째에 tacrolimus의 최저혈중농도를 관측한 7개 연구의 결과를 합성했을 때 3435CC는 3435TT에 비해, 3435CT 는 3435TT에 비해 tacrolimus의 혈중농도가 유의한 수준으로 낮 았으며 연구들간 이질성은 발견되지 않았다(Fig. 4). 출판편향을 관찰했을 때 표본수가 작은 연구들이 누락되었을 가능성을 배제 하기는 어려워 보인다(Fig. 5). 이식 후 3개월째에 3435CC와 3435CT 간에 tacrolimus 혈중농도의 유의한 차이는 나타나지 않
았다(CC vs CT, WMD:-8.59; 95% CI: -20.86, 3.67; p=0.17;
I2: 66%).36,38,39,42-45)
소아를 대상으로 한 Shilbayeh 등의 연구를44) 제외한 후 성인 대상 연구만으로 분석했을 때 3435CC는 3435TT 및 3435CT에 비해, 3435CT는 3435TT에 비해 tacrolimus의 혈중농도가 유의한 수준으로 낮았으며 연구들간 이질성은 없거나 낮은 정도였다(CC vs. TT, WMD: -31.54; 95% CI: -38.18, -24.91; p<0.00001; I2: 0%); CC vs. CT, WMD: -19.66; 95% CI: -24.61, -14.70;
Fig. 3 − Forest plots of the association between ABCB1 C3435T polymorphism and dose-adjusted trough concentration of tacrolimus in adult recipients at the first month after kidney transplantation. Squares represent study-specific weight mean difference (WMD); horizontal lines represent 95% CIs; diamond represents the summary pooled WMD.
Fig. 4 − Forest plots of the association between ABCB1 C3435T polymorphism and dose-adjusted trough concentration of tacrolimus in pediatric and adult kidney transplant recipients at 3 months after operation. Squares represent study-specific weight mean difference (WMD);
horizontal lines represent 95% CIs; diamond represents the summary pooled WMD.
p<0.00001; I2: 40%; CT vs. TT, WMD: -11.00; 95% CI: -17.99, -4.01; p=0.002; I2: 0%).36,38,39,42,43,45)
한편, 아시아 인종에서의 영향을 분석했을 때 3435CC는 3435TT에 비해, 3435CT는 3435TT에 비해 tacrolimus의 혈중농 도가 통계적으로 유의하게 낮았지만, 3435CC와 3435CT 간에 유 의한 차이는 없었다(CC vs. TT, WMD: -29.75; 95% CI: -36.93, -22.57; p<0.00001; I2: 0%; CC vs. CT, WMD: -8.76; 95% CI:
-30.00, 12.48; p=0.42; I2: 74%; CT vs. TT, WMD: -8.97;
95% CI: -16.49, -1.46; p=0.02; I2: 0%).36,39,43) 이와 유사한 결 과가 코카서스 인종의 성인과 소아에서도 관찰되었다(CC vs. TT, WMD: -32.52; 95% CI: -50.16, -14.88; p=0.0003; I2: 0%; CC vs. CT, WMD: -4.13; 95% CI: -28.20, 19.95; p=0.74; I2: 62%; CT vs. TT, WMD: -23.66; 95% CI: -43.02, -4.31;
p=0.02; I2: 0%;).38,44,45)
Fig. 5 − Funnel plot for publication bias of the included studies for the effects of ABCB1 C3435T polymorphism on dose-adjusted trough concentration of tacrolimus in kidney transplant recipients at 3 months after operation. (A) CC vs TT (B) CT vs TT.
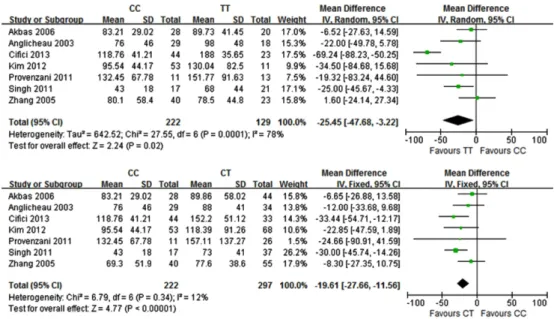
Fig. 6 − Forest plots showing the effects of ABCB1 C3435T polymorphism on dose-adjusted trough concentration of tacrolimus in adult
recipients at 6 months after kidney transplantation. Squares represent study-specific weight mean difference (WMD); horizontal lines
represent 95% CIs; diamond represents the summary pooled WMD.
이식 후 6개월째에 관측된 영향
이식 후 6개월째에 tacrolimus의 최저혈중농도를 관측한 7개 연구의 결과를 결합했을 때 3435CC에서의 농도는 3435TT에서 의 농도에 비해 유의한 수준으로 낮았다(CC vs. TT, WMD: -17.23;
95% CI: -33.56, -0.91; p=0.04; I2: 78%).38-40,42-45) 하지만, 3435CC와 3435CT, 3435CT와 3435TT 간에는 tacrolimus 최저 혈중농도에 있어 유의한 차이가 관찰되지 않았다(CC vs. CT, WMD: -9.54; 95% CI: -25.85, 6.77; p=0.25; I2: 87%; CT vs.
TT, WMD: -1.13; 95% CI: -13.06, 10.80; p=0.85; I2: 63%).38-
40,42-45)
반면, 소아를 대상으로 한 Shilbayeh 등의 연구를44)제외 한 후 성인대상 연구만으로 분석했을 때 3435CC에서는 3435TT 및 3435CT에 비해, 3435CT에서는 3435TT에 비해 tacrolimus의 혈 중농도가 유의한 수준으로 낮았으며 연구들간 이질성은 발견되 지 않았다(Fig. 6).
한편, 코카서스 인종의 성인과 소아에서의 영향을 분석했을 때 3435CC와 3435TT 간에 통계적으로 유의한 차이가 보이지 않았 다(CT vs. TT, WMD: -11.58; 95% CI: -39.33, 16.17; p=0.14;
I2: 81%).38,40,44,45)반면, 코카서스 인종의 성인대상 연구만을 분 석했을 때는 3435CC는 3435TT 및 3435CT에 비해 tacrolimus 의 혈중농도가 통계적으로 유의하게 낮았으나 3435CT와 3435TT 간에 유의한 차이는 없었다(CC vs. TT, WMD: -22.27; 95% CI:
-33.47, -11.08; p<0.0001; I2: 0%; CC vs CT, WMD: -16.42;
95% CI: -27.30, -5.54; p=0.003; I2: 0%; CT vs. TT, WMD: - 5.58; 95% CI: -18.63, 7.47; p=0.4; I2: 0%).38,40,45)
고 찰 (Discussion)
본 메타분석에서 ABCB1 C3435T는 신장이식 수혜자에서 tacrolimus의 최저혈중농도에 유의한 영향을 미치는 것으로 나타 났다. 성인 수혜자에서 이식 후 1주, 1개월, 3개월, 6개월째에 측 정한 tacrolimus의 최저혈중농도는 ABCB1 3435TT 혹은 3435CT 유전자형에 비해 3435CC 유전자형에서 유의하게 낮았다. 이는 신장이식 수혜자에서 tacrolimus의 최저혈중농도를 유사하게 유 지하기 위해 3435CC 유전자형을 가진 수혜자에게는 3435TT 혹 은 3435CT 유전자형을 가진 수혜자에 비해 고용량의 tacrolimus 를 투여해야 함을 의미한다. 유전자형 3435CT와 3435TT간 혈 중농도의 차이를 분석했을 때, 이식 후 1주 및 1개월째에는 3435CT와 3435TT 사이에 유의한 차이가 나타나지 않았으나 이 식 후 3개월과 6개월째에는 3435CT에서의 혈중농도가 3435TT 에 비해 낮았다. 따라서, 두 유전자형에서 유사한 혈중농도를 유 지하기 위해서는 3435CT 유전자형을 가진 수혜자에게는 3435TT 유전자형을 가진 수혜자보다 고용량의 tacrolimus를 투여해야 하 는 것으로 보인다. 반면, 연구대상이 소아를 포함한 경우 이식 후
1주와 1개월째에 3435CC와 3435TT 간에 유의한 차이가 관찰 되지 않았는데 이는 Turolo 등의37) 연구결과에 의한 영향으로 보 인다. Turolo 등은 평균연령이 11세인 이탈리아 소아에서 3435CC 에서의 혈중농도가 3435TT에서의 혈중농도보다 높았다고 보고 했는데 이 결과는 이후에 Shilbayeh 등이44)발표한 연구결과와 도 상반된다. Shilbayeh 등은 평균연령이 11세인 요르단 소아를 대상으로 수행한 연구에서 3435CC에서의 혈중농도가 3435TT 에서의 혈중농도보다 낮았음을 보여주었다.
본 메타분석에서 이식 후 6개월째에 3435CC 유전형에서의 ‘체 중당 투여용량 대비 최저혈중농도 비’는 3435TT 유전형에 비해 17.23 ng/ml/mg/kg만큼 낮았으나 3435CT와 3435TT 사이에서는 유의한 차이가 나타나지 않았다. 반면, 소아를 제외한 성인 수혜 자에서의 영향을 분석했을 때 3435TT 유전형에 비해, 3435CC 유전형은 26.46 ng/ml/mg/kg만큼, 3435CT 유전형은 6.57 ng/ml/
mg/kg만큼 낮았다. 이에 반해 Li 등이 선행한 메타분석에서는26) 이식 후 6개월째에 3435CC와 3435TT 간에 통계적으로 유의한
‘체중당 투여용량 대비 최저혈중농도 비’의 차이가 관찰되지 못 했다. 하지만 Li 등의 연구에서 3435CT에서의 ‘체중당 투여용량 대비 최저혈중농도 비’가 3435TT에 비해 21.15 ng/ml/mg/kg만 큼 낮았으며 이 결과는 3435CT와 3435TT에서 유사한 혈중농 도를 유지하기 위해 3435CT 유전자형을 가진 수혜자에게 tacrolimus의 투여량을 증가시켜야 할 것으로 관찰된 본 연구결 과와 일관성이 있다. 한편, Li 등의 연구와 비슷한 시기에 발표 된 Terrazzino 등의 메타분석에서27)이식 후 3~6개월째에 유전 자형 CC에서의 ‘체중당 투여용량 대비 최저혈중농도 비’는 CT+TT 유전자형에 비해 5.51 ng/ml/mg/kg만큼 낮았던 것으로 관찰되어 본 연구결과와 일관된다. 하지만 Terrazzino 등의 연구 에서는 이식 후 3~6개월째에 유전자형 TT에서의 ‘체중당 투여 용량 대비 최저혈중농도 비’가 CC+CT에 비해 0.6 ng/ml/mg/kg 만큼 낮았던 것으로 나타났다. 결과 값의 크기를 고려할 때 유전 자형 CC+CT와 TT 사이에 차이가 없었던 것으로 해석한다 하 더라도 이 결과는 본 연구 및 Li 등이 수행한 연구 결과와 큰 차 이를 보인다. 본 연구에서는 이식 후 3개월째에 3435CT의 ‘체중 당 투여용량 대비 최저혈중농도 비’는 3435TT에 비해 11.85 ng/
ml/mg/kg만큼 낮았으며, Li 등이 수행한 메타분석에서는 이식 후 6개월째에 3435CT에서의 ‘체중당 투여용량 대비 최저혈중농도 비’가 3435TT에 비해 21.15 ng/ml/mg/kg만큼 낮았다. 선행된 Terrazzino 등의 메타분석26)및 Li 등의 메타분석27)결과와 본 연구 결과들 간에 보이는 이러한 차이는, 근래에 발표된 연구로 서 선행된 2개의 메타분석에는 포함되지 못했던 연구들이 본 연 구에는 포함되어 분석된 것에 기인한다고 여겨진다. 또한 Li 등 은 tacrolimus의 ‘체중당 투여용량 대비 최저혈중농도 비’를 평 균값이 아닌 최소값과 최대값으로 보여주는 연구들도 포함시켜 분석한 반면 본 연구는 최소값과 최대값을 이용하여 평균을 산
출하는 경우 발생하는 오차를46)없애기 위해 그러한 연구들을 배 제하여 분석하지 않은 것도 두 연구의 결과들에서 차이가 나타 나는 이유가 된다.
본 연구결과와 선행 메타분석의 결과를 종합할 때, 신장이식 수혜자에서 tacrolimus의 혈중농도를 유사하게 유지하기 위해서 는 이식 후 적어도 6개월까지는 ABCB1 3435CC 유전자형에게 는 3435TT 및 3435CT 유전자형보다, 3435CT 유전자형에게는 3435TT 유전자형보다 고용량의 tacrolimus를 투여할 것을 고려 해야 하는 것으로 보인다. 이 결과는 ABCB1 C3435T가 P-당단 백질의 발현에 영향을 미치며 3435TT 유전자형을 가진 사람에 서는 3435CC 유전자형을 가진 사람에 비해 소장에서의 P-당단 백질의 발현이 낮고간 조직에서의 ABCB1 mRNA 수준이 낮음 을 보여준 연구들에 의해 지지된다.23,47)
한편, 연구대상을 아시아 인종인 경우와 코카서스 인종인 경우 로 나누어 각 인종에서 ABCB1 C3435T가 tacrolimus의 최저혈 중농도에 미치는 영향을 분석하였을 때 각각의 인종에서 관찰된 결과는 인종의 구분 없이 분석했을 때 나타난 결과와 일관되었다.
본 연구에서 ABCB1 C3435T가 신장이식 수혜자에서의 tacrolimus 최저혈중농도에 유의한 영향을 미치는 것으로 나타났 지만, 이 결과는 ABCB1 C3435T 외 tacrolimus의 최저농도에 영 향을 미치는 타 요소를 고려해야 하는 한계점을 지닌다. CYP3A5 가 tacrolimus의 대사에 주요하게 관여하며 간과 소장에서 CYP3A5 의 발현이 많은 사람에서는 tacrolimus의 최저혈중농도가 감소 되어 있음이 관찰되었다.49) 또한 tacrolimus의 최저혈중농도는 CYP3A5의 유전적 변이에 의해서도 영향을 받아 CYP3A5*1 allele을 가진 사람에서의 혈중농도는 CYP3A5*3/*3 allele을 가 진 사람에 비해 유의하게 낮았다.50)뿐만 아니라, tacrolimus의 최저혈중농도는, 본 메타분석에 포함된 연구들이 면역억제요법 으로 tacrolimus와 병용한 steroid에 의해서도 영향을 받는다.
Corticosteroid는 CYP3A와 P-당단백질을 유도하므로 각 연구에서 병용된 methylprednisolone/prednisone의 용량이 높을수록 tacrolimus의 최저혈중농도는 감소할 수 있다.51)
이 같은 한계점에도 불구하고 본 연구는 신장이식 후 급성거 부반응을 예방하고 이식신과 수혜자의 생존율을 향상시키는 등 임상적 치료성과를 극대화하기 위해 최적의 tacrolimus 투여용 량을 결정하는 것에 ABCB1 C3435T 단일염기다형성을 바이오 마커로서 활용할 것을 제안하는 것에 그 의의가 있다고 하겠다.
결 론 (Conclusion)
본 연구에서, 이식 후 6개월 동안 ABCB1 3435C allele을 가 진 신장이식 성인 수혜자는 3435C allele을 가지지 않은 성인 수 혜자에 비해 tacrolimus의 최저혈중농도가 유의한 수준으로 낮 았다. 따라서, 신장이식 후 발생하는 급성거부반응을 예방하기
위해 ABCB1 3435C allele을 가진 성인 수혜자에게는 3435C allele을 가지지 않은 성인 수혜자에 비해 고용량의 tacrolimus를 사용해야 할 것으로 여겨진다. 이러한 용량조정은 코카서스 인 종뿐 아니라 아시아 인종에서도 요구되는 것으로 보인다.
References
1) Kim, M. H., Kim, M. S., Kwon, O. J. and Kang, C. M.:
Comparison of Quality of Life between Kidney Transplant Patients and Dialysis Patients. J. Korean Soc. Transplant. 23, 65 (2009).
2) Tonelli, M., Wiebe, N., Knoll, G., Bello, A., Browne, S., Jadhav, D., Klarenbach, S. and Gill, J.: Systematic review: kidney transplantation compared with dialysis in clinically relevant outcomes. Am. J. Transplant. 11, 2093 (2011).
3) Kim, S. I., Kim, Y. S., Kim, M. S., Park, E. C., Jeon, K. O., Son, S. Y., Hahm, M. I. and Lee, H. Y.: A renal transplantation and hemodialysis cost-utility analysis in patients with end-stage renal disease. J. Korean Soc. Transplant. 24, 173 (2010).
4) Center for Korean Network for Organ Sharing. Organ transplantation status. Available at http://konos.go.kr/konosis/
common/bizlogic.jsp.: Accessed on 12 June 2018.
5) Karam, S. and Wali, R. K.: Current state of immunosuppression:
past, present, and future. Crit. Rev. Eukaryot. Gene Expr. 25, 113 (2015).
6) Shrestha, B., Haylor, J. and Raftery, A.: Historical perspectives in kidney transplantation: an updated review. Prog. Transplant.
25, 64 (2015).
7) Sá, H., Leal, R. and Rosa, M. S.: Renal transplant immunology in the last 20 years: A revolution towards graft and patient survival improvement. Int. Rev. Immunol. 36, 182 (2017).
8) Jalalzadeh, M., Mousavinasab, N., Peyrovi, S. and Ghadiani, M.
H.: The impact of acute rejection in kidney transplantation on long-term allograft and patient outcome. Nephrourol. Mon. 7, e24439 (2015).
9) Kim, C. D.: Kidney transplantation. Korean J. Med. 86, 142 (2014).
10) Azzi, J. R., Sayegh, M. H. and Mallat, S. G.: Calcineurin inhibitors: 40 years later, can't live without ... J. Immunol. 191, 5785 (2013).
11) Meier-Kriesche, H. U., Li, S., Gruessner, R. W., Fung, J. J., Bustami, R. T., Barr, M. L. and Leichtman, A. B.:
Immunosuppression: evolution in practice and trends, 1994- 2004. Am. J. Transplant. 6, 1111 (2006).
12) Staatz, C. E. and Tett, S. E.: Clinical pharmacokinetics and pharmacodynamics of tacrolimus in solid organ transplantation.
Clin. Pharmacokinet. 43, 623 (2004).
13) Staatz, C., Taylor, P. and Tett, S.: Low tacrolimus concentrations and increased risk of early acute rejection in
adult renal transplantation. Nephrol. Dial. Transplant. 16, 1905 (2001).
14) Kidokoro, K., Satoh, M., Nagasu, H., Sakuta, T., Kuwabara, A., Yorimitsu, D., Nishi, Y., Tomita, N., Sasaki, T. and Kashihara, N.: Tacrolimus induces glomerular injury via endothelial dysfunction caused by reactive oxygen species and inflammatory change. Kidney Blood Press. Res. 35, 549 (2012).
15) Andrews, L. M., Li, Y., De Winter, B. C. M., Shi, Y. Y., Baan, C.
C., Van Gelder, T. and Hesselink, D. A.: Pharmacokinetic considerations related to therapeutic drug monitoring of tacrolimus in kidney transplant patients. Expert. Opin. Drug Metab. Toxicol. 13, 1225 (2017).
16) Undre, N. A. and Schäfer, A.: Factors affecting the pharmacokinetics of tacrolimus in the first year after renal transplantation. European Tacrolimus Multicentre Renal Study Group. Transplant Proc. 30, 1261 (1998).
17) Zhang, Y. and Benet, L. Z.: The gut as a barrier to drug absorption. Combined role of cytochrome P450 3A and P- glycoprotein. Clin. Pharmacokinet. 40, 159 (2001).
18) Hashida, T., Masuda, S., Uemoto, S., Saito, H., Tanaka, K. and Inui, K.: Pharmacokinetic and prognostic significance of intestinal MDR1 expression in recipients of living-donor liver transplantation. Clin. Pharmacol. Ther. 69, 308 (2001).
19) Masuda, S., Goto, M., Okuda, M., Ogura, Y., Oike, F., Kiuchi, T., Tanaka, K. and Inui, K.: Initial dosage adjustment for oral administration of tacrolimus using the intestinal MDR1 level in living-donor liver transplant recipients. Transplant Proc. 37, 1728 (2005).
20) Masuda, S., Goto, M., Fukatsu, S., Uesugi, M., Ogura, Y., Oike, F., Kiuchi, T., Takada, Y., Tanaka, K. and Inui, K.: Intestinal MDR1/ABCB1 level at surgery as a risk factor of acute cellular rejection in living-donor liver transplant patients. Clin.
Pharmacol. Ther. 79, 90 (2006).
21) Hodges, L. M., Markova, S. M., Chinn, L. W., Gow, J. M.,Kroetz, D.
L., Klein, T. E. and Altman, R. B.: Very important pharmacogene summary: ABCB1 (MDR1, P-glycoprotein). Pharmacogenet.
Genomics 21, 152 (2011).
22) Wolking, S., Schaeffeler, E., Lerche, H., Schwab, M. and Nies, A. T.: Impact of genetic polymorphisms of ABCB1 (MDR1, P- Glycoprotein) on drug disposition and potential clinical implications: Update of the Literature. Clin. Pharmacokinet.
54, 709 (2015).
23) Hoffmeyer, S., Burk, O., von Richter, O., Arnold, H. P., Brockmöller, J., Johne, A., Cascorbi, I., Gerloff, T., Roots, I., Eichelbaum, M. and Brinkmann, U.: Functional polymorphisms of the human multidrug-resistance gene: multiple sequence variations and correlation of one allele with P-glycoprotein expression and activity in vivo. Proc. Natl. Acad. Sci. U S A. 97, 3473 (2000).
24) Hesselink, D. A., van Gelder, T. and van Schaik, R. H.: The pharmacogenetics of calcineurin inhibitors: one step closer toward individualized immunosuppression? Pharmacogenomics.
6, 323 (2005).
25) Fung, K. L. and Gottesman, M. M.: A synonymous polymorphism in a common MDR1 (ABCB1) haplotype shapes protein function.
Biochim. Biophys. Acta. 1794, 860 (2009).
26) Li, Y., Hu, X., Cai, B., Chen, J., Bai, Y., Tang, J., Liao, Y. and Wang, L.: Meta-analysis of the effect of MDR1 C3435T polymorphism on tacrolimus pharmacokinetics in renal transplant recipients.
Transpl. Immunol. 27, 12 (2012).
27) Terrazzino, S., Quaglia, M., Stratta, P., Canonico, P. L. and Genazzani, A. A.: The effect of CYP3A5 6986A>G and ABCB1 3435C>T on tacrolimus dose-adjusted trough levels and acute rejection rates in renal transplant patients: a systematic review and meta-analysis. Pharmacogenet. Genomics. 22, 642 (2012).
28) Borobia, A. M., Romero, I., Jimenez, C., Gil, F., Ramirez, E., De Gracia, R., Escuin, F., Gonzalez, E. and Sansuán, A. J.: Trough tacrolimus concentrations in the first week after kidney transplantation are related to acute rejection. Ther. Drug Monit. 31, 436 (2009).
29) Ihara, H., Shinkuma, D., Ichikawa, Y., Nojima, M., Nagano, S.
and Ikoma F.: Intra- and interindividual variation in the pharmacokinetics of tacrolimus (FK506) in kidney transplant recipients--importance of trough level as a practical indicator.
Int. J. Urol. 2, 151 (1995).
30) Hu, R. H., Lee, P. H. and Tsai, M. K.: Clinical influencing factors for daily dose, trough level, and relative clearance of tacrolimus in renal transplant recipients. Transplant Proc. 32, 1689 (2000).
31) Wells, G. A., Shea, B., O'Connell, D., Peterson, J., Welch, V., Losos, M. and Tugwell, P. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta- analyses. Available at http://konos.go.kr/konosis/common/
bizlogic.jsp.: Accessed 17 May 2018.
32) Zheng, J. S., Hu, X. J., Zhao, Y. M., Yang, J. and Li, D.: Intake of fish and marine n-3 polyunsaturated fatty acids and risk of breast cancer: meta-analysis of data from 21 independent prospective cohort studies. BMJ. 346, f3706 (2013).
33) Xuan, C., Zhang, B. B., Li, M., Deng, K. F., Yang, T. and Zhang, X. E.: No association between APOE ε 4 allele and multiple sclerosis susceptibility: a meta-analysis from 5472 cases and 4727 controls. J. Neurol. Sci. 308, 110 (2011).
34) Zhang, B. B., Xuan, C., Deng, K. F., Wu, N. and Lun, L. M.:
Association between the MDR1 gene variant C3435T and risk of leukaemia: a meta-analysis. Eur. J. Cancer Care (Engl). 22, 617 (2013).
35) Anglicheau, D., Verstuyft, C., Laurent-Puig, P., Becquemont, L., Schlageter, M. H., Cassinat, B., Beaune, P., Legendre, C.
and Thervet E.: Association of the multidrug resistance-1 gene single-nucleotide polymorphisms with the tacrolimus dose requirements in renal transplant recipients. J. Am. Soc.
Nephrol. 14, 1889 (2003).
36) Zhang, X., Liu, Z. H., Zheng, J. M., Chen, Z. H., Tang, Z., Chen, J. S. and Li, L. S.: Influence of CYP3A5 and MDR1 polymorphisms on tacrolimus concentration in the early stage after renal transplantation. Clin. Transplant. 19, 638 (2005).
37) Turolo, S., Tirelli, A. S., Ferraresso, M., Ghio, L., Belingheri, M., Groppali, E., Torresani, E. and Edefonti, A.: Frequencies and roles of CYP3A5, CYP3A4 and ABCB1 single nucleotide polymorphisms in Italian teenagers after kidney transplantation.
Pharmacol. Rep. 62, 1159 (2010).
38) Provenzani, A., Notarbartolo, M., Labbozzetta, M., Poma, P., Vizzini, G., Salis, P., Caccamo, C., Bertani, T., Palazzo, U., Polidori, P., Gridelli, B. and D'Alessandro, N.: Influence of CYP3A5 and ABCB1 gene polymorphisms and other factors on tacrolimus dosing in Caucasian liver and kidney transplant patients. Int. J. Mol. Med. 28, 1093 (2011).
39) Wang, W., Zhang, X. D., Ma, L. L., Lü, Y. P., Hu, X. P., Zhang, P., Wang, Y. and Guan, D. L.: [Relationship between MDR1 gene polymorphism and blood concentration of tacrolimus in renal transplant patients]. Natl. Med. J. China. 85, 3277 (2005).
40) Akbas, S. H., Bilgen, T., Keser, I., Tuncer, M., Yucetin, L., Tosun, O., Gultekin, M. and Luleci, G.: The effect of MDR1 (ABCB1) polymorphism on the pharmacokinetic of tacrolimus in Turkish renal transplant recipients. Transplant Proc. 38, 1290 (2006).
41) Jun, K. R., Lee, W., Jang, M. S., Chun, S., Song, G. W., Park, K.
T., Lee, S. G., Han, D. J., Kang, C., Cho, D. Y., Kim, J. Q. and Min, W. K.: Tacrolimus concentrations in relation to CYP3A and ABCB1 polymorphisms among solid organ transplant recipients in Korea. Transplantation. 87, 1225 (2009).
42) Singh, R., Srivastava, A., Kapoor, R. and Mittal, R. D.: Do drug transporter (ABCB1) SNPs influence cyclosporine and tacrolimus dose requirements and renal allograft outcome in the posttransplantation period? J. Clin. Pharmacol. 51, 603 (2011).
43) Kim, I. W., Moon, Y. J., Ji, E., Kim, K. I., Han, N., Kim, S. J, Shin, W. G., Ha, J., Yoon, J. H., Lee, H. S. and Oh, J. M.: Clinical and genetic factors affecting tacrolimus trough levels and drug- related outcomes in Korean kidney transplant recipients. Eur.
J. Clin. Pharmacol. 68, 657 (2012).
44) Shilbayeh, S., Zmeili, R. and Almardini, R. I.: The impact of CYP3A5 and MDR1 polymorphisms on tacrolimus dosage requirements and trough concentrations in pediatric renal transplant recipients. Saudi. J. Kidney Dis. Transpl. 24, 1125 (2013).
45) Ciftci, H. S., Ayna, T. K., Caliskan, Y. K., Guney, I., Bakkaloglu, H., Nane, I., Aydin, A. E., Turkmen, A. and Gurtekin, M.:
Effect of MDR1 polymorphisms on the blood concentrations of tacrolimus in Turkish renal transplant patients. Transplant Proc. 45, 895 (2013).
46) Wan, X., Wang, W., Liu, J. and Tong, T.: Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 19, 135 (2014).
47) Shou, W., Wang, D., Zhang, K., Wang, B., Wang, Z., Shi, J. and Huang, W.: Gene-wide characterization of common quantitative trait loci for ABCB1 mRNA expression in normal liver tissues in the Chinese population. PLoS One. 7, e46295 (2012).
48) Ciftci, H. S., Ayna, T. K., Caliskan, Y. K., Guney, I., Bakkaloglu, H., Nane, I., Aydin, A. E., Turkmen, A. and Gurtekin, M.:
Effect of MDR1 polymorphisms on the blood concentrations of tacrolimus in Turkish renal transplant patients. Transplant Proc. 45, 895 (2013).
49) Birdwell, K. A., Decker, B., Barbarino, J. M., Peterson, J. F., Stein, C. M., Sadee, W., Wang, D., Vinks, A. A., He, Y., Swen, J. J., Leeder, J. S., van Schaik, R., Thummel, K. E., Klein, T. E., Caudle, K. E. and MacPhee, IA.: Clinical pharmacogenetics implementation consortium (CPIC) guidelines for CYP3A5 genotype and tacrolimus dosing. Clin. Pharmacol. Ther. 98, 19 (2015).
50) MacPhee, I. A., Fredericks, S., Tai, T., Syrris, P., Carter, N. D., Johnston, A., Goldberg, L. and Holt, D. W.: The influence of pharmacogenetics on the time to achieve target tacrolimus concentrations after kidney transplantation. Am. J. Transplant.
4, 914 (2004).
51) Anglicheau, D., Flamant, M., Schlageter, M. H., Martinez, F., Cassinat, B., Beaune, P., Legendre, C. and Thervet E.:
Pharmacokinetic interaction between corticosteroids and tacrolimus after renal transplantation. Nephrol. Dial. Transplant.
18, 2409 (2003).