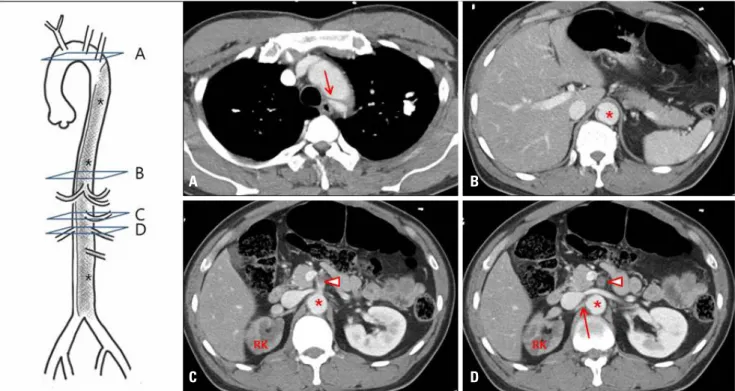
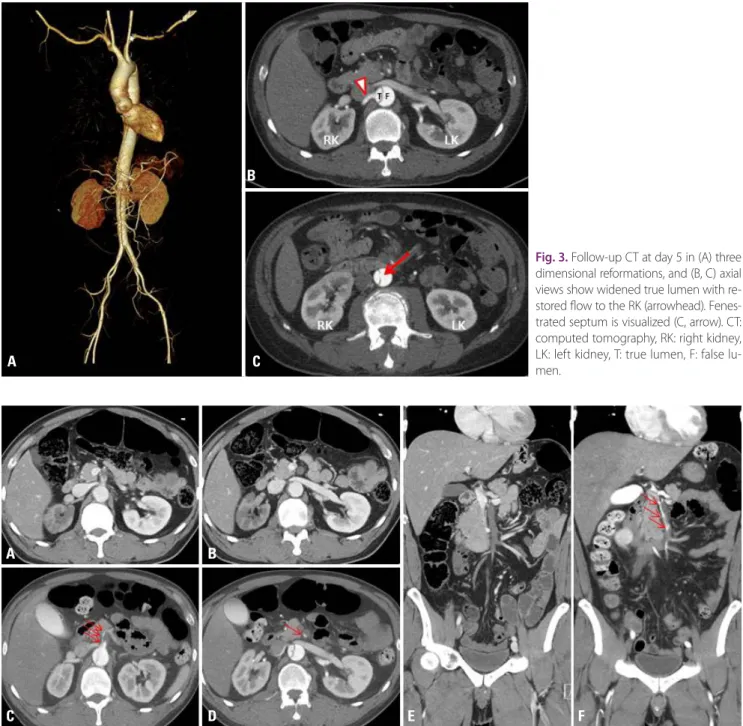
Type B Aortic Dissection with Visceral Artery Involvement Following Blunt Trauma: A Case Report
6
0
0
전체 글
(2)
(3)
(5)
수치

관련 문서
been largely tried and accepted in hemodynamically stable patients.(2,3) We report a case of hepatic duct confluence injury after blunt abdominal trauma successfully
We report the case of a 43-year- old male patient who experienced an aortic injury caused by the sharp edge of a fractured rib after multiple rib frac- tures due to
Despite the frequent use of CT for the evaluation of chest injury after blunt trauma, di- agnosis of tracheobronchial rupture by CT scan has rarely been reported: to our knowledge,
Acute myocardial infarction (AMI) is a rare complication that can occur after blunt chest trauma. 1)2) Blunt chest trau- ma can lead to various cardiac complications ranging from
A CASE OF RETROPERITONEAL HEMATOMA CAUSED BY LEFT OVARIAN ARTERY RUPTURE FOLLOWING MILD BLUNT TRAUMA
We report a case of retroperitoneal hematoma caused by rupture of left ovarian artery occurred after abdominal blunt trauma including brief review of the literatures.. Keywords:
Acute complicated type B aortic dissection (TBAD) is a potentially catastrophic, life-threatening condition. Several risk factors have been associated with acute
