대한골절학회지 제18권, 제2호, 2005년 4월 Journal of the Korean Fracture Society
Vol. 18, No. 2, April, 2005
압박 고나사를 이용한 대퇴골 전자간부 골절 치료의 방사선학적 결과
- 외측 피질골 침범 여부를 중심으로 -
이석하·이성태·오광준·김영배
*·이우승
*·전지성·유인록·금정섭
건국대학교 의과대학 건국대학교병원 정형외과학교실, 서울 보훈병원 정형외과학교실*
목 적: 압박 고나사를 이용하여 외측 피질골을 침범한 대퇴골 전자간 골절의 치료결과를 방사선학적으로 분석하여 불안정성 대퇴 전자간 골 절의 의미를 알아보고자 하였다.
대상 및 방법: 1999년 1월부터 2002년 6월까지 본원에서 대퇴골 전자간 골절로 압박 고나사를 이용하여 수술 받은 환자 중 지연 나사의 대퇴 골두 내에서의 위치, Tip-Apex distance (TAD), 그리고 Singh의 골다공증 수치 등이 통계적으로 차이가 없는 24례를 대상으로 하였다. 결과 분석은 외측 피질골을 침범하지 않은 골절군 (group A: 16례)과 외측 피질골을 침범한 골절군 (group B: 8례)으로 구분하여 최종 추시 시 방 사선학적 평가에서의 전위 정도, 경간각의 내반 및 외반 변화, 지연 나사의 활강 정도, 그리고 경간각의 변화 등을 통계적으로 분석하였다.
결 과: 최종 추시 시 지연 나사의 활강 정도는 외측 피질골을 침범한 골절군 (group B)에서는 평균 14.8±9.3 mm였고, 외측 피질골을 침범 하지 않은 골절군 (group A)에서는 6.7±3.6 mm로 통계학적으로 의미 있는 차이가 없었으며 (p value>0.05), 내반 각변형은 외측 피질골을 침범한 골절군 (group B)에서는 평균 8.00±8.12도였고, 외측 피질골을 침범하지 않은 골절군 (group A)에서는 2.75±2.63도로 통계학적으로 의미 있는 차이가 있었다 (p value<0.05). 전위 정도에서는 외측 피질골을 침범한 골절군 (group B)에서는 7.60±2.61 mm였고, 외측 피질골 을 침범하지 않은 골절군 (group A)에서는 0.5±1.80 mm로 통계학적으로 의미 있는 차이가 있었다 (p value<0.05).
결 론: 외측 피질골을 침범한 대퇴 전자간 골절은 수술 후 해부학적 정복을 얻었다 하더라도 전위가 발생할 수 있는 불안정성 대퇴 전자간 골절로 간주하여 치료방침을 결정하는 것이 바람직하다 하겠다.
색인 단어: 불안정성 전자간 골절, 압박 고나사, 외측 피질골
Radiologic Result of Treatment of Intertrochanteric Fracture Using Compression Hip Screw - Involvement of Lateral Cortex -
Suk-Ha Lee, M.D., Sung-Tae Lee, M.D., Kwang-Jun Oh, M.D., Yong-Bae Kim
*, M.D., Woo-Seung Lee
*, M.D., Ji-Sung Jun, M.D., In-Rok Yoo, M.D., Jung-Sup Keum, M.D.
Department of Orthopedic Surgery, KonKuk University Hospital, College of Medicine, KonKuk University, Seoul, Korea Department of Orthopedic Surgery, Seoul Veterans Hospital, Seoul, Korea
*Purpose: To assess the meaning of the unstable intertrochanteric fracture of femur with involvement of lateral cortex by analysing the radiologic result of the surgical treatment using a compression hip screw.
Materials & Methods: Classifing patients (who has taken the surgical treatment for intertrochanteric fracture of femur using compression hip screw from January 1999 to June 2002) in our hospital with 24 patients who had not much difference statistically in the compression screw located within the femur, Tip-Apex distance (TAD) the Singh Numerical Value of osteoporosis. The results were divided into two groups, group A (without fracture extends through lateral cortex of femur: 16 cases) and B (fracture extends through lateral cortex of femur: 8 cases), when analyzing it. And then analyzed the final examination in the evaluation of electrical potential level by radiology, change of the inside and outside of neck-shaft angle, descent level of the screw and the change of the neck-shaft angle.
Result: In the latest follow up, the sliding amount of the screw in group B, the average was 14.9±9.3 mm, and 6.7±3.6 mm in group A. There was no difference statistically (p value>0.05). In the varus change in group B, the average was 8.00±8.12° and in group A it ws 2.75±2.63°
There was statistical difference(p value<0.05). In displacement after operation, it was 7.60±2.61 mm in group B and 0.5±1.80 mm in group A.
There was statistical difference (p value<0.05).
Conclusion: The intertrochanteric fracture with involvement of lateral cortex of femur have to be considered as unstable fracture having tendency of displacement.
Key Words: Intertrochanteric fracture, Compression hip screw, Involvement of lateral cortex of femur
115 통신저자 : 이 성 태
서울특별시 광진구 화양동 1번지 건국대학교병원 정형외과학교실 Tel : 82-2-450-9685·Fax : 82-2-458-1134 E-mail : damioh@yahoo.co.kr
*본 논문의 요지는 2003년도 제 29차 대한골절학회 춘계학술대회에서 구연하였음.
Address reprint requests to : Sung Tae Lee, M.D.
Department of Orthopaedic Surgery, Konkuk University Seoul Hospital, Hwayang-dong, Kwangjin-gu, Seoul 143-701, Korea
Tel : 82-2-450-9685·Fax : 82-2-458-1134 E-mail : damioh@yahoo.co.kr
서 론
대퇴 전자간 골절은 고령의 연령층에서 빈발하나 근래 교 통수단 및 산업재해의 증가로 큰 외상 및 외력에 노출되기 쉬운 장년층에서도 그 빈도가 증가하고 있다. 이러한 골절의 수술적 치료 시 정확한 해부학적 정복 및 견고한 내고정을 위하여 여러 가지 기구들이 고안되어 왔으며, 그 중 특히 압 박 고나사를 이용한 고정 방법이 선호되고 있다5,15). 압박 고 나사의 원리는 골절부위로 압박을 주어 골유합을 촉진시키 고 지연 나사의 활강을 통하여 내고정 기구로의 부하와 골두 천공의 위험을 줄이는 것으로, 이러한 압박 고나사의 대표적 적응증이 대퇴전자를 통한 골절, 또는 대퇴 전자간 골절이다.
그러나, 대퇴골 전자간 골절의 수술은 활강 압박 고나사를 사용하였을 때 5~23% 정도의 실패를 야기한다고 알려져 있
다2~4,6,19). 고정실패에 영향을 미치는 요인으로는 불안정성
골절, 정복의 방법, 내고정물의 종류와 위치, 골밀도 등이 있고9), 특히 불안정성 골절양상을 파악하는 것이 적절한 내고정물을 선택하여 고정실패를 예방하는데 중요한 수술적 지침이 된다.
이에 저자는 압박 고나사를 내고정물로써 사용한 예 중
지연 나사의 위치, 골밀도 등이 동일한 조건의 환자를 대상 으로 방사선학적 평가를 시행하여 불안정성 골절의 의미에 대하여 고찰하고자 하였다.
대상 및 방법
1999년 1월부터 2002년 3월까지 대퇴골 전자간 골절에 대 해 압박 고나사를 이용하여 치료받은 환자 중 9개월 이상 추 시가 가능했던 24례를 대상으로 후향적 평가를 실시하였다.
이 중, 남자가 8례, 여자가 16례였고, 평균 연령은 67.3세였 다. 수상 원인은 실족이 18례 (75%)로 가장 많았고, 낙상이 5례 (21%), 교통사고가 1례 (4%)순이었다. 이를 외측 피질골 을 침범한 골절군 (B군)과 외측 피질골을 침범하지 않은 골 절군 (A군)으로 나누었으며 A 군은 16례, B군은 8례였다.
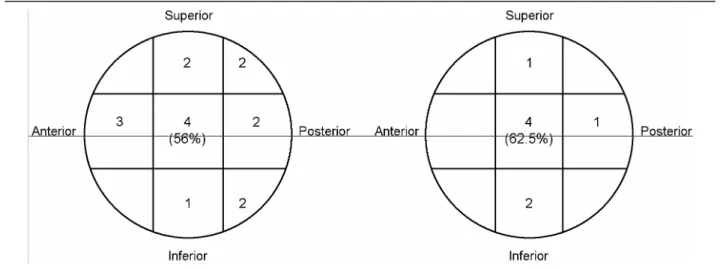
두 군은 지연 나사의 골두 내 위치, Singh의 골다공증 수 치16), TAD (Tip-Apex distance)가 동일한 조건으로, 지연 나 사의 골두 내 위치는 양측 모두 중앙으로 위치된 경우가 많 아 A군은 56%, B군은 62.5%였다 (Table 1). Singh의 골다공 증 수치의 분포는 A군에서는 grade 3가 5례, grade 4가 8례, grade 5가 3례였고, B군에서는 grade 3가 3례, grade 4가 4례, grade 5가 1례로 두군 사이에 통계적으로 유의한 차이는 없
Table 1. Placement of lag screw
Table 2. Singh Index
Singh Index Group A (cases) Group B (cases)
Grade 3 5 3
Grade 4 8 4
Grade 5 3 1
Total (cases) 16 8
p>0.05
Table 3. Tip-Apex distance (TAD) Group Number of
patients (cases)
Average (mm)
Standard deviation (±)
Group A 16 22.14 3.58
Group B
(Transverse) 8 24.00 5.08 p>0.05
었다 (Table 2). TAD는 A군에서는 평균 22.14 mm, B군에서 는 24 mm로 통계적으로 유의한 차이는 없었다 (Table 3).
수술 후 처치는 수술 다음날 sitting position을 시켰으며 walker를 이용한 체중부하는 수술 후 약 6주부터 허용하였으 나 환자 상태, 방사선 추시 관찰을 통한 골절부위의 안정성 에 따라 그 시기를 적절히 조정하였다.
고정실패의 정의는 10도 이상의 내반 및 외반 변형, 지연 나사못의 골두 천공, 지연 나사못의 활강 정도가 15 mm 이 상 되어 동통 및 하지단축으로 인한 증상이 있는 경우, 그리 고 금속판의 고정소실 등으로 정의하였다12,15,18).
지연 나사못의 활강 정도는 술 후 전후방 사진과 추시 전 후방 사진에서의 활강 정도의 차이를 측정하였고, 추시 사 진에서 대퇴 경간각을 측정하여 술 후 사진과의 각변형의 차이를 측정하였다. 또한 골절의 전위 정도도 수술직후와 추
시 사진에서 전위된 골절선의 양 끝에 평행한 선을 전후면 사진에서는 수직으로, 측면 사진에서는 수평으로 그어 측정 하였다. 통계는 SAS와 dBSTAT을 이용하여 t-test 및 nonpa- rameter Wilcoxon Rank Sums test를 사용하였으며 통계적 유 의성은 p-value가 0.05보다 작은 경우로 하였다.
결 과
고정실패의 결과를 보면 B군에서 10도 이상의 내반 변형 이 1례 있었으며, TAD 35 mm 이상이었던 B군의 1례에서 골 두 천공이 1례 있었고, 15 mm 이상의 지연 나사못의 활강 은 A군에서 2례, B군에서 2례 있었다.
양측 군에서의 지연 나사못의 활강은 두군 각각 평균이 A군은 6.7±3.6 mm, B군은 14.8±9.3 mm으로 통계적으로 유 의한 차이는 없었다 (p>0.05) (Table 4). 수술 후 각변형의 비 교에서는 A군은 평균 2.75±2.63도, B군은 8±8.12도로 통계 적으로 유의한 차이가 있는 것으로 나타났다 (p<0.05) (Table 5). 수술 후 전위 정도의 비교에서도 A군은 평균 0.5±1.80 mm, B군은 평균 7.6±2.61 mm로 통계적으로 유의한 차이가 있는 것으로 나타났다 (p<0.05) (Table 6).
지연 나사의 위치, Singh의 골다공증 수치, TAD가 통계적 으로 차이가 없는 총 24례만을 대상으로 외측 피질골의 골
Table 5. Angulation change (varus) Group Number of
patients (cases)
Average (degrees)
Standard deviation (±)
Group A 16 2.75 2.63
Group B
(Transverse) 8 8.00 8.12
p<0.05
Table 6. Displacement Group Number of
patients (cases)
Average (mm)
Standard deviation (±)
Group A 16
0.5
1.80Group B
(Transverse) 8
7.60
2.61p<0.05 Table 4. Amount of Lag screw sliding
Group Number of patients (cases)
Average (mm)
Standard deviation (±)
Group A 16 6.7 3.6
Group B
(Transverse) 8 14.8 9.3 p>0.05
A B C
Fig. 1. (A) Preoperative radiographs show Evans type 1, AO type C3.2 fracture on the anteroposterior and lateral views.
(B) Postoperative radiographs show a good antomical reduction with TAD: 20 mm, neck-shaft angle 140 degrees.
(C) At follow up, through the transverse fracture line, 16 mm displacement was occured and 5 degree varus deformity, 7 mm sliding was accompanied.
절선이 있는 군과 없는 군으로 나누어 분석한 결과, Fig. 1, Fig. 2와 같이 외측 피질골의 골절선을 가진 대퇴전자간 골 절은 압박 고나사를 이용하여 해부학적 정복을 얻었다 하더 라도 지연 나사의 활강을 통한 감입과 더불어 전위가 발생할 수 있기 때문에 그 안정성을 유지할 수 없었다.
고 찰
대퇴골 전자간 골절의 수술적 치료에는 95도 angled de- vice, 골수강내 금속정, 압박 고나사 등 다양한 기구들이 사 용되고 있으며 1941년 Lorenz가 lag screw 개념을 도입한 이 후 1950년대에 Pugh16)가 sliding nail plate를 고안하였고 이후 Massie13)와 Richard에 의해 압박 고나사 (compression hip screw)가 개발되어 현재까지 대퇴골 전자부 골절 치료 시 금 속 내고정물로 가장 많이 사용되고 있다. 이러한 압박 고나 사의 원리는 지연 나사의 활강을 통하여 골절부위로 압박을 주어 골유합을 촉진시키는 것으로, 역동적 내고정물에 해당 한다. 따라서 안정성 골절인 경우 유용한 내고정물로써 장점 을 가지고 있으나, 불안정성 골절인 경우 골절면의 내측 감 입의 결과로 경간각의 감소가 유발되고 고정의 이완 및 지 연 나사의 활강과 더불어 전이가 발생할 수 있기 때문에 골 절면의 정확한 해부학적 정복을 얻었다 하더라도 고정실패 의 가능성은 오히려 증가할 수 있다.
불안정성 골절에 대한 기술로는 Evans에 의한 분류와 AO 분류가 있으며, Evans는 분쇄 골절양상을 보이거나 해부학 적 정복 후에도 후내측 피질골이 정복되지 않거나 역사위 골 절선을 가지면 불안정성 골절로 정의한 반면, AO에서는 분 쇄 골절이고 정복이 어려운 경우를 불안정성 골절로 구분하 였다. 이처럼 Evans에 의한 분류는 외측 피질골 골절에서 역 사위 골절선 만을 강조한 반면, AO에서는 외측 지지대의 중 요성을 인지하고 외측 피질골의 개념을 도입하여 A3 group 중 단순 역사위 골절선이 있는 경우를 A3.1로, 횡형 골절선
이 있는 경우를 A3.2로 따로 구분하여 이를 더 세분, 대퇴 전자간 불안정성 골절에 대한 개념을 좀더 명확히 하였다.
또한, 고도의 불안정성 다분절 골절 (A2.3, A3)에는 압박 고 나사가 적절치 않다고 하였다. 본 연구에서도 Singh의 골다 공증 수치, TAD, 지연 나사의 골두내 위치 등이 같은 조건인 예를 대상으로 한 방사선학적 평가 상 수술 후 각변형과 전 위 정도가 외측 피질골을 침범한 대퇴 전자간 골절군에서 통계적으로 의미있게 높았으며 이는 수술 직후 해부학적 정 복을 유지할 수 없음을 의미한다. 이러한 불안정성 전자간 골절시 과거에는 내측 전위 절골술1)을 골절유합을 촉진시키 기 위해 권장되어 왔으나 최근엔 압박 고나사와 더불어 과금 속판 (Trochanteric Stabilizing Plate)을 추가하거나, 근위 대퇴 골수정, fixed angled blade 금속판을 사용하여 좋은 결과를 보고하고 있다. Robert Buciuto 등은 불안정성 대퇴 전자간 골 절에서 angled blade 금속판이 특히 술 후 해부학적 정복의 유지에 압박 고나사에 비하여 좋은 결과를 보인다고 하였으 며17), George J Haidukewych 등은 외측 피질골을 침범한 대퇴 전자간 골절에서 압박 고나사에 비해 근위 대퇴 골수정은 골 절부 감입 및 단축이 적다는 점에서, 95도 angled blade 금속 판은 골절면의 회전 변형과 외측 전위를 막아준다는 점에서 더 우수하다고 하였다7).
하지만 본 연구에서는 불안정성 대퇴 전자간 골절의 의미 를 알아보고자 하는 압박 고나사를 사용한 증례만을 조사하 여 제한점이 있으며 향후 다른 내고정 기구를 사용한 경우와 비교하는 것이 필요하다.
결 론
외측 피질골을 침범한 대퇴 전자간 골절을 압박 고나사를 사용하여 해부학적 정복을 얻었다 하더라도 지연 나사의 활 강을 통한 전이가 발생할 수 있으므로 불안정성 골절로 간주 하여 치료 방침을 결정해야 할 것으로 사료된다.
Fig. 2. (A) Preoperative radiographs show Evans type 1, AO type C3.2 fracture on the anteroposterior and lateral views. The radiographs show a involvement of lateral cortex of proximal femur
(B) Postoperative radiograph
(C) At follow up, through the transverse fracture line, 8 mm displacement was occured, and 13 mm sliding was accompanied.
A B C
참 고 문 헌
1) Baumgaertner MR, Curtin SL, Lindskog DM and Keiggi JM: The value of the tip-apex distance in predicting failure of fixation of pertrochanteric fractures of the hip. J Bone Joint Surg, 77-A: 1058-1064, 1995.
2) Bridle SH, Patel AD, Bircher M and Calvert PT: Fixation of intertrochanteric fractures of the femur. A randomised pro- spective comparison of the Gamma nail and dynamic hip screw. J Bone Joint Surg, 73-B: 330-334, 1991.
3) Min BW, Kang CS and Kang CH: Fixation failure in pa- tients with proximal fractures of the femur treated with a compression hip screw. J Korean Hip Soc, 10(2): 37-41, 1998.
4) Davis TRC, Sher JL, Horsman A, Simpson M, Porter BB and Checketts RG: Intertrochanteric femoral fractures. Me- chanical failure after internal fixation. J Bone Joint Surg, 72-B: 26-31, 1990.
5) Hwang DS, Kwak SG, Kim YM, Nam DC and Hong UP:
Fixation Failure of Compression Hip Screw in Unstable Inter- trochanteric Fracture of Femur. J Korean Fracture Soc, 16:
600-605, 2003.
6) Dimon JH and Hughston JC: Unstable intertrochanteric fractures of the hip. J Bone Joint Surg, 49-A: 440-450, 1967.
7) Flores LA, Harrinhton IJ and Martin H: The stability of intertrochanteric fractures treated with a sliding screw plate. J Bone Joint Surg, 72-B: 37-40, 1990.
8) George J Haidukewych, T Andrew Israel, Daniel J Berry:
Reverse obliquity fractures of the intertrochanteric region of the femur. J Bone Joint Surg, 83: 643-649, 2001
9) Jensen JS, Tondevoid E and Mossing N: Unstable trochan- teric fractures treated with the sliding-plate system: a biome- chanical study of unstable trochanteric fracture III. Acta Orthop Scand, 49: 392-397, 1978.
10) Lee JH, Kang SB, Park JS and Moon SH: Fixation Fai- lure after Internal Fixation In Intertrochanteric Fractures. J Korean Orthop Soc, 32(7): 41-48, 1997.
11) Roh KJ, Kim JO and Kim HH: Problems of compression hip screw for the treatment of intertrochanteric fracture in
eldely patients. J Korean Fracture Soc, 12: 502-508, 1999.
12) Laros GS and Moore JF: Complications of fixation in in- tertrochanteric fractures. Clin Orthop, 101: 110-119, 1974.
13) Madsen JE, Naess L, Aune AK, Alho A, Ekeland A and Stromsoe K: Dynamic hip screw with trochanteric stabilizing plate in the treatment of unstable proximal femoral fractures.
A comparative study with the Gamma nail and compression hip screw. J Orthop Trauma, 12(4): 241-248, 1998.
14) Madson JE, Naess L, Aune AK, Alho A, Ekeland A and Stromsoe K: Dynamic hip screw with trochanteric stabilizing plate in the treatment of unstable proximal femoral fractures.
A comparative study with the Gamma nail and compression hip screw. J Orthop Trauma, 12(4): 241-248, 1998.
15) Massie WKK: Fractures of the hip. J Bone Joint Surg, 46-A:
658-690, 1964.
16) Pugh WLK: A self-adjusting ail plate for fractures about the hip joint. J Bone Joint Surg, 37-A: 1085-1093, 1955.
17) Rha JD, Kim YH, Yoon SI, Park TS and Lee MH: Factors affecting sliding of the lag screw in intertrochanteric fractures.
International Orthop, 17: 320-324, 1993.
18) Robert Buciuto and Richard Hammer: RAB-plate versus sliding hip screw for unstable trochanteric hip fractures. J Trauma, 50(3): 545-550, 2001.
19) Singh M, Nagraph AR and Maini PS: Changes in trabe- cular pattern of the femur as an index of osteoporosis. J Bone Joint Surg, 52-A: 457-467, 1970.
20) Thomas AP: Dynamic hip screws that fail. Injury, 22(1):
45-46, 1991.
21) Wolfgang GL, Bryant MH and ONeill JP: Treatment of intertrochanteric fracture of the femur using sliding screw plate fixation. Clin Orthop, 163: 148-158, 1982.
22) Choy WS, Ahn JH, Kim BS, Lee KW, Kim WJ and Keum TS: Analysis of Prognostic Factors for Intertrochanteric Frac- ture of Femur Treated with the Compression Hip Screw. J Korean Hip Soc, 13: 221-228, 2001.
23) Zuckerman JD, Skovron ML, Koval KJ, Aharonoff G and Frankel VH: Postoperative complications and mortality asso- ciated with operative delay in older patient who have a frac- ture of the hip. J Bone Joint Surg, 77-A: 1551-1556, 1995.