접수일: 2011년 6월 9일 수정일: 2011년 12월 7일 게재승인일: 2011년 12월 16일
교신저자: 김의종, 110-744 서울시 종로구 대학로 101 서울대학교병원 진단검사의학과
Tel: 02-2072-3500, Fax: 02-764-6542 E-mail: [email protected]
*이 연구는 2010년 질병관리본부의 학술연구용역사업인 ‘전국 병원감염감시체계구축: 중소병원(연구비 번호 2010E4400700)’
의 지원을 받아 수행되었음.
중소병원의 의료관련감염 감시
박은숙1ㆍ진혜영2ㆍ정선영3ㆍ권오미1ㆍ유소연4ㆍ박신영5ㆍ김성란6ㆍ홍혜경7ㆍ김옥선8
김경미9ㆍ윤성원10ㆍ정재심11ㆍ용동은12ㆍ김명수13ㆍ박대원14ㆍ조용균15ㆍ오향순16ㆍ염준섭17ㆍ김의종18
세브란스병원 감염관리실1, 아주대병원 감염관리실2, 이대 목동병원 감염관리실3, 가톨릭대학교 성빈센트병원 감염관리실4, 가천의대 길병원 적정진료관리실5, 고려대학교 구로병원 감염관리실6, 관동대학교 의과대학 명지병원 적정진료관리실7,
영동대학교 간호학과8, 세명대학교 간호학과9, 삼성서울병원 감염관리실10, 울산대학교 임상전문간호학11, 연세의대 진단검사의학과12, 광명성애병원 내과13, 고려의대 감염내과14, 가천의대 감염내과15, 서울대학교병원
감염관리실16, 강북삼성병원 감염내과17, 서울의대 진단검사의학과18
Healthcare-Associated Infection Surveillance in Small and Medium Sized Hospitals
Eun Suk Park
1, Hye Young Jin
2, Sun Young Jeong
3, Oh Mee Kweon
1, So-Yeon Yoo
4,
Shin Yong Park
5, Sung Ran Kim
6, Hae Kyung Hong
7, Og Sun Kim
8, Kyung Mi Kim
9, Sung Won Yoon
10, Jae Sim Jeong
11, Dongeun Yong
12, Muyng Soo Kim
13, Dae-Won Park
14, Yong Kyun Cho
15,
Hyang Soon Oh
16, Joon-Sup Yeom
17, and Eui-Chong Kim
18Infection Control Office, Severance Hospital
1, Ajou University Hospital
2, Ewha Womans University Mokdong Hospital
3, The Catholic University of Korea, St. Vincent’s Hospital
4, Department of Quality Improvement, Gachon University Gil Hospital
5, Infection Control Office, Korea University Guro Hospital
6, Office of Infection Control, Gwandong University College of Medicine Myongji Hospital
7, Department of Nursing, Youngdong University
8, Department of Nursing, Semyung University
9, Infection Control Office, Samsung Medical Center
10, School of Clinical Nursing, University of Ulsan
11, Department of Laboratory Medicine, Yonsei University, College of Medicine
12, Department of Internal Medicine, Gwangmyung Sungae Hospital
13, Devision of Infectious Disease, Korea University College of Medicinel
14, Devision of Infectious Disease, Gachon University pf Medicine and Science
15, Infection Control Office, Seoul National University
Hospital
16, Department of Internal Medicine, Kangbuk Samsung Hospital
17, Department of Laboratory Medicine, Seoul National University College of Medicine
18, Korea
Background: The purpose of this study is to know the healthcare-associated infection (HAI)s in small and medium sized hospitals, less than 400 beds.
Methods: We had web based surveillance for HAIs in 27 hospitals from August to October 2010. The surveillance performed in 1-2 ICUs and 1 general ward in each hospitals by CDC definition. And for the multi-drug resistant organisms (MDROs), we reviewed all of blood culture results.
Results: We identified 319 HAIs among 269,436 patients days. The HAIs rate was 1.18 (CI 1.05-1.32)/1,000 patient-
days. Urinary tract infection was the most common HAI (52.4%) in this study followed by pneumonia (18.9%), blood-
stream infections (14.2%), surgical site infection (7.9%), and others (6.6%). There were 76.5% of device associated
infections in UTI, 46.7% in BSI, and 18.3% in pneumonia. The rate of HAIs in ICU was higher than that of in general
ward (4.6 vs 0.9/1,000 patient-days). However, the indwelling catheter associated urinary tract infection rate was lower
in ICU (2.6 vs 4.4/1,000 device days). There were no significant differences in central line-associated blood stream
infection rate (1.5 vs 1.8) and ventilator-associated pneumonia rate (3.0 vs 0.0). The common microorganisms found in HAIs were Escherichia coli (19.8%), Staphylococcus aureus (13.1%), and Pseudomonas aeruginosa (12.7%). Moreover, 90.9% of S. aureus were resistant to methicillin, and 38.2% of P. aeruginosa and 44.4% of Acinetobacter baumannii were resistant to imipenem. Total of 66 MDROs were isolated from blood culture and the result shows that the MRSA was 84.6% (56 case), carbapenmen-resistant Acinetobacter spp. was 10.6% (7 case), and vancomycin-resistant entero- cocci was 4.6% (3 case).
Conclusion: The characteristics of HAIs in small and medium sized hospitals will be contributed to the decision making of governance policy for infection control and to provide comparable data for these hospitals.
Keywords: Small hospital, Healthcare-associated infection, ICU, Multidrug resistant organisms
서 론
국내 의료관련감염에 대한 연구 및 정책들은 대부분 400병상 이상 대형병원들을 중심으로 진 행되어 왔으나[1-3], 300병상 미만의 종합병원까 지 의료기관평가가 확대되면서 중소병원에서의 감염관리 필요성이 확대되고 있다[4]. 감염의 위 험요인은 의료기관의 특성에 따라 달라지므로 감염관리 역시 기관의 특성을 고려하여 진행되 어야 한다. 중소병원에 대한 일부 정책연구들을 통해 중소병원들은 감염관리 인력 및 지식의 부 족, 진단검사체계의 미흡, 경영자의 인식부족 등 으로 감염관리 뿐만 아니라 기본적인 감염감시 진행이 쉽지 않은 것으로 알려져 있다[5,6]. 이러 한 여러 가지 제약들로 인해 중소병원에서의 의 료관련 감염의 발생실태는 확인되지 못하고 있 다. 이에 중소병원에서의 여러 가지 제한점에도 불구하고 실무자들이 쉽게 접근할 수 있는 감시 체계의 개발과 이를 통한 중소병원에서의 의료 관련감염의 실태를 파악할 필요성이 대두되었다.
본 연구의 목적은 중소병원에서의 의료관련 감 염현황을 파악하는 것이며, 이를 위하여 중소병 원의 참여가 가능한 감염감시체계를 구축하였다.
대상 및 방법
감염감시체계 개발과 개발된 감시체계를 통한 감염감시조사의 2단계로 이루어졌으며 총 연구 기간은 2010년 5월부터 2010년 12월까지 총 8개 월이었다. 5월부터 7월까지 3개월간의 웹기반 감 시체계를 개발하였으며 감시는 8월부터 10월까
지 3개월간 진행되었다.
웹기반 감시체계는 문헌고찰 및 초점그룹 인 터뷰를 통해 중소병원의 특성과 요구를 반영하 여 개발하였다. 기존 Korean nosocomial infection surveillance (KONIS) 시스템을 기반으로 신뢰도 와 실무 적용성을 증가시키는 것에 중점을 두어 1) 세부 감염진단에 따른 주요 증상 입력과 기준 에 부합되지 않는 경우 경고 메시지 활성화, 2) 감시 단위(병동 및 중환자실)별 특성에 따른 비 교, 3) 균주 분포, 4) 그래프 및 도표 제공이 가능 하도록 하였다.
참여병원은 400병상 미만 중소병원으로 대한 병원감염관리학회와 대한감염관리간호사회의 홈 페이지를 통해 공모하였다.
의료관련감염의 정의는 미국 질병관리본부와 전국의료안전네트워크(National healthcare safety network, NHSN)의 정의[7]를 사용하였으며 감염 감시에 대한 신뢰도 및 타당도를 위하여 참여병 원의 감염감시 실무자들에 대한 교육, 매뉴얼 및 진단기준 핸드북의 제작 및 배포, 홈페이지를 통 한 사례검토 등을 진행하였다.
감시부위는 중소병원에서 발생하는 감염의 특
성을 분석하기 위하여 모든 부위의 의료관련 감
염을 조사하였으며, 임상적 패혈증 및 기타부위
요로감염을 포함하였다. 대상부서는 중환자실과
일반병동을 포함하였으며, 참여병원당 중환자실
과 일반병동 1개 이상씩 진행하였다. 다제내성균
주의 현황파악을 위하여 검사실 기준으로 혈액을
대상으로 조사하였다. 감염이나 의료기관과의 연
관성과 상관없이 분리된 다제내성균주 모두 조
사하였으며, Methicillin-resistant S. aureus (MRSA)
Table 1. Healthcare-associated infection rate by nursing ward type and hospital size, August through October 2010 Total infections Patient-days Pooled mean 95% CI P value 10‰ 25‰ 50‰ 75‰ 90‰
Total HAI 317 269,436 1.18 1.05-1.31 0.33 0.56 1.34 3.43 7.03
Gen Ward 228 250,226 0.91 0.8-1.04 0.000 0.28 0.44 0.69 1.4 2.25
ICU 89 19,210 4.63 3.76-5.7 2.29 2.76 3.93 6.99 9.41
≥200 bed 278 226,726 1.23 1.09-1.38 0.094 0.3 0.56 1.43 3.43 7.52
<200 bed 39 42,710 0.91 0.67-1.25 0.41 0.61 1.02 3.41 4.22
Abbreviation: HAI, Healthcare-associated infection.
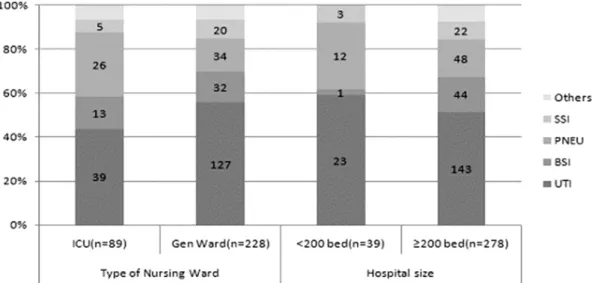
Fig. 1. Distribution of site specific HAI by type of nursing ward and hospital size, August through October 2010. Abbreviations: UTI, urinary tract infection; BSI, bloodstream infection; PEN, pneumonia; SSI, surgical site infection.
와 vancomycin-resistant enterococci (VRE), carbepe- nem-resistant Acinetobacter spp., carbepenem-resis- tant Klebsiella spp., carbepenem-resistant Pseudomo-
nas spp.를 대상으로 하였다.분석은 SPSS for Windows ver. 12.0 (SPSS Inc., Chicago, IL, USA)프로그램을 이용하여 실수와 백 분율, χ
2-test, ANOVA로 분석하였다.
결 과
1. 참여병원 특성
총 27개 병원이 참여하였다. 일반병동 감시에 25 개 병원 52개 병동이 참여하였고, 중환자실 감시 에는 22개 병원 23개 중환자실, 혈액내 다제내성 균 감시에는 25개 병원이 참여하였다. 중환자실은 여러 임상과가 혼재된 통합중환자실이 90.9% (20 개)로 가장 많았으며, 일반병동은 통합병동 56.9%, 외과계 병동 23.5%, 내과계 병동 19.6%였다.
병상규모는 200-300병상 규모가 48.1% (13개) 로 가장 많았으며, 지역별 분포는 서울/경기에 집 중되는 경향(63.0%, 17개)을 보였으며, 전라도 (14.8%, 4개), 경상도(11.1%, 3개), 제주도(2개), 충 청도(1개)까지 분포하였다. 병원특성은 대부분이 종합병원(88.5%, 24개)이었으며, 여성전문병원, 외 과전문병원, 노인이나 산재 및 만성환자 중심의 병원처럼 특성화된 경우가 37.0% (10개)였다. 인 턴, 인턴 및 전공의 수련병원이 48.1% (13개)였으 며 간호등급은 3등급 44.4% (12개), 4-5등급 33.3%
(9개), 6등급 이하 22.2% (6개)였다. 평균재원일은 17±19.6일, 평균병상 이용률은 79±20.3%였다.
감염관리간호사는 전임인 곳이 48.1% (13개), 감염관리 업무를 연간 지속적으로 진행하는 경 우는 66.7% (18개)였다. 감염관리 경력이 3년 이 상 되는 곳은 44.4% (12개)였으며 최근 3년 이내 1회 이상 전담자가 교체된 곳이 19.6% (8개)였다.
자체 미생물검사실을 운영하는 경우가 70.4% (19
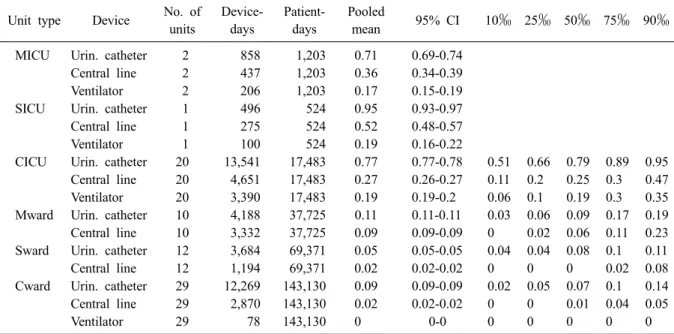
Table 3. Pooled means and percentiles of the distribution of device-utilization rations, by type of ICU and Ward. August through October 2010
Unit type Device No. of units
Device- days
Patient- days
Pooled
mean 95% CI 10‰ 25‰ 50‰ 75‰ 90‰
MICU Urin. catheter 2 858 1,203 0.71 0.69-0.74 Central line 2 437 1,203 0.36 0.34-0.39
Ventilator 2 206 1,203 0.17 0.15-0.19
SICU Urin. catheter 1 496 524 0.95 0.93-0.97 Central line 1 275 524 0.52 0.48-0.57
Ventilator 1 100 524 0.19 0.16-0.22
CICU Urin. catheter 20 13,541 17,483 0.77 0.77-0.78 0.51 0.66 0.79 0.89 0.95 Central line 20 4,651 17,483 0.27 0.26-0.27 0.11 0.2 0.25 0.3 0.47 Ventilator 20 3,390 17,483 0.19 0.19-0.2 0.06 0.1 0.19 0.3 0.35 Mward Urin. catheter 10 4,188 37,725 0.11 0.11-0.11 0.03 0.06 0.09 0.17 0.19 Central line 10 3,332 37,725 0.09 0.09-0.09 0 0.02 0.06 0.11 0.23 Sward Urin. catheter 12 3,684 69,371 0.05 0.05-0.05 0.04 0.04 0.08 0.1 0.11
Central line 12 1,194 69,371 0.02 0.02-0.02 0 0 0 0.02 0.08
Cward Urin. catheter 29 12,269 143,130 0.09 0.09-0.09 0.02 0.05 0.07 0.1 0.14 Central line 29 2,870 143,130 0.02 0.02-0.02 0 0 0.01 0.04 0.05
Ventilator 29 78 143,130 0 0-0 0 0 0 0 0
Abbreviations: MICU, medical ICU; SICU, surgical ICU; CICU, complex ICU; Mward, medical ward; Sward, surgical ward; Cward, complex ward.
Table 2. Device-associated infection rates by type of nursing ward
Place type of infection
General ward ICU
P value No. of
infections
Device
days Rate No. of
infections
Device
days Rate
Catheter associated UTI 88 20,141 4.37 39 14,895 2.62 0.002
Central line associated BSI 13 7,359 1.77 8 5,363 1.49 0.467
Ventilator associated pneumonia 0 78 0.00 11 3,696 2.98 0.578
Abbreviations: UTI, urinary tract infection; BSI, bloodstream infection; PNEU, pneumonia.
개)였으며, 그람 염색만 진행하는 경우가 11.6%
(3개)였다.
2. 의료관련 감염률
전체 52개 일반병동과 23개 중환자실에서 3개 월간 총 269,436 환자일수 동안 319건의 의료관 련감염이 발생하여 환자일수 1,000일당 1.18건의 감염률을 보였다. 중환자실에서 일반병동보다 유 의하게 발생률이 높았으며, 200병상을 중심으로 병상규모에 따른 감염률의 차이는 유의하지 않 았다(Table 1).
부위별감염의 분포는 요로감염이 52.4% (166건) 로 가장 많았으며 폐렴 18.9%, 혈류감염 14.2%, 수술부위감염 7.9%, 기타 6.6%의 순이었으며 기 타로는 위장관감염, 눈/코/귀 감염, 피부 및 연조
직 감염, 중추신경계감염 등이었다. 중환자실이 일반 병동보다 폐렴의 분포가 많았으며, 200병상 이상에서 혈류감염의 분포가 많았다(Fig. 1). 요 로감염의 76.5%, 혈류감염의 46.7%, 폐렴의 18.3%
가 삽입기구사용과 관련성이 있었다.
삽입기구관련 감염은 유치도뇨관 관련 요로감
염은 중환자실에서 오히려 일반병동보다 유의하
게 낮았으며, 중심정맥관 관련 혈류감염이나 인
공호흡기관련 폐렴은 유의한 차이가 없었다(Table
2). 중환자실은 종류가 다양하지 못해 환자 특성
에 따른 비교를 하지 못하였으나 일반병동은 병
동 특성에 따라 차이가 있었다. 내과계병동에서
유치도뇨관이나 중심정맥관 사용비가 높았으며
(Table 3), 유치도뇨관 관련 요로감염은 내과계병
동과 외과계병동에서 통합병동보다 유의하게 높
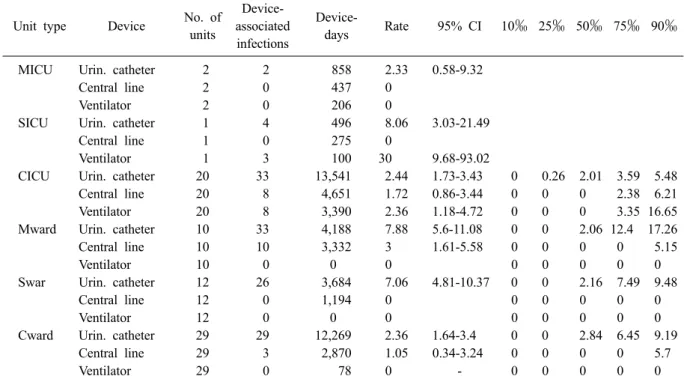
Table 4. Pooled means and percentiles of the distribution of device associated infection rates, by type of ICU and Ward, August through October 2010
Unit type Device No. of
units
Device- associated
infections
Device-
days Rate 95% CI 10‰ 25‰ 50‰ 75‰ 90‰
MICU Urin. catheter 2 2 858 2.33 0.58-9.32
Central line 2 0 437 0
Ventilator 2 0 206 0
SICU Urin. catheter 1 4 496 8.06 3.03-21.49
Central line 1 0 275 0
Ventilator 1 3 100 30 9.68-93.02
CICU Urin. catheter 20 33 13,541 2.44 1.73-3.43 0 0.26 2.01 3.59 5.48
Central line 20 8 4,651 1.72 0.86-3.44 0 0 0 2.38 6.21
Ventilator 20 8 3,390 2.36 1.18-4.72 0 0 0 3.35 16.65
Mward Urin. catheter 10 33 4,188 7.88 5.6-11.08 0 0 2.06 12.4 17.26
Central line 10 10 3,332 3 1.61-5.58 0 0 0 0 5.15
Ventilator 10 0 0 0 0 0 0 0 0
Swar Urin. catheter 12 26 3,684 7.06 4.81-10.37 0 0 2.16 7.49 9.48
Central line 12 0 1,194 0 0 0 0 0 0
Ventilator 12 0 0 0 0 0 0 0 0
Cward Urin. catheter 29 29 12,269 2.36 1.64-3.4 0 0 2.84 6.45 9.19
Central line 29 3 2,870 1.05 0.34-3.24 0 0 0 0 5.7
Ventilator 29 0 78 0 - 0 0 0 0 0
Abbreviations: MICU, medical ICU; SICU, surgical ICU; CICU, complex ICU; Mward, medical ward; Sward, surgical ward; Cward, complex ward.
았다(Table 4).
의료관련감염의 원인균 분포는 요로감염에서는
Escherichia coli, 폐렴에서는 Pseudomonas aerugi- nosa나 Acinetobacter baumannii와 같은 그람음성균주의 분포가 많았고, 혈류감염이나 수술부위감 염에서는
S. aureus나 coagulase-negative staphylo-cocci와 같은 그람양성 균주가 많았다(Table 5). 분 리된 균주의 항생제 내성은
S. aureus의 90.9%가methicillin 내성이었으며, P. aeruginosa의 38.2%,
A. baumannii의 44.4%가 imipenem에 대한 내성을보였다. Enterococcus faecium과 Enterococcus faeca-
lis의 경우 vancomycin에 대한 내성은 각각 8.3%였다. E. coli의 경우 cefotaxime과 ciprofloxacin에 대한 내성은 각각 34.0%와 18.9%였으며. K. pneu-
moniae는 cefotaxime에 37.5%, ciprofloxacin에 20.8%의 내성을 보였다. 중환자실에서는 다소 내성률 이 낮은 경향을 보였으나 분리건수 자체가 많지 않아 정확한 분석은 하지 못했다.
3. 혈액 내 다제내성균주 분리현황
25개 병원에서 3개월간 환자일수 556,642일 동
안 혈액에서 분리된 다제내성균주는 총 66건으로 환자일수 1,000일당 0.12건의 발생률을 보였다. 다 제내성균주의 84.6% (56건)은 MRSA였으며, car- bapenem-resistant Acinetobacter spp. (CRA) 10.6%
(7건), VRE 4.6% (3건)의 순으로 분리되었고 car- bapenem-resistant Klebsiella spp.나 Pseudomonas spp.의 발생은 없었다. Enterococcus faecium은 모두 quinupristin-dalfopristin에 감수성을 보였다. CRA 7건 중 6건은 A. baumannii였으며 이중 2건은 β- lactam, carbapenem, aminoglycoside, fluoroquino- lone에 모두 내성을 보였다.
VRE와 carbapenem-resistant Acinetobacter spp.는 모두 200병상 이상 규모의 병원에서만 보고되었다.
분리장소는 병동 71.2% (47건), 중환자실 22.7%
(15건)이었으며, 응급실과 혈액투석실에서 각각
3건, 1건 분리되었다. 다제내성균주가 분리되기
전까지 재원기간은 평균 32일, 중앙값 14일이었
다. 입원 3일 이내에 발생한 경우는 19.7% (13건)
였으며, 이 중 3개월 이내에 의료기관 입원력이
있었던 경우는 61.5% (8건)였다. 다제내성균주의
분리 전 평균 재원기간은 MRSA 33.5±61.0일(0-
Table 6. Comparison of device use and rate of device-associated infection in the ICU among in small hospital and other networks
Device utilization ratio Device associated infection rate
Small hospital KONIS 2009 (400-700)
NHSN
2006-2008 Small hospital KONIS 2009 (400-700)
NHSN (2006-2008) ICAUTI 0.78* (0.77-0.78) 0.78 (0.78-0.79) 0.64 (0.53-0.80 2.62
†(1.91-3.58) 5.92 (5.40-6.49) 3.4 (0.0-4.3) CLABSI 0.28*
†(0.27-0.29) 0.43 (0.43-0.43) 0.39 (0.20-0.50) 1.49
†(0.75-2.98) 3.55 (3.02-4.17) 1.5 (0.0-1.8) VAP 0.19*
†(0.19-0.20) 0.36 (0.36-0.36) 0.29 (0.13-0.38) 2.98 (1.65-5.37) 2.22 (1.78-2.77) 2.2 (0.0-3.0)
*P value<0.05 compared NHSN;
†P value<0.05 compared KONIS.
Abbreviations: KONIS, Korean nosocomial infection surveillance; NHSN, National safety network all others ICU ≤15 beds.
Table 5. Number (%) of microorganisms isolated from clinical specimens of patients with healthcare associated in- fections August through October 2010
Microorganisms No. of isolates (%)
UTI BSI PNEU SSI Others All
Gram-positive cocci (%) 30 (18.6) 23 (57.5) 12 (28.6) 11 (57.9) 3 (75.0) 79 (29.7)
Staphylococcus aureus 4 13 10 4 2 33 (12.4)
Staphylococci, coagulase-negative 2 8 6 1 17 (6.4)
Enterococcus faecalis 11 1 12 (4.5)
Enterococcus faecium 11 1 12 (4.5)
Corynebacterium species 1 1 (0.4)
Others 2 2 4 (1.5)
Gram-negative bacilli (%) 116 (72.0) 17 (42.5) 30 (71.4) 8 (42.1) 171 (64.3)
Acinetobacter baumannii 4 7 6 1 18 (6.8)
Enterobacter cloacae 2 1 1 2 6 (2.3)
Escherichia coli 52 1 53 (19.9)
Klebsiella pneumoniae 17 3 4 24 (9.0)
Proteus mirabilis 7 1 8 (3.0)
Pseudomonas aeruginosa 23 2 9 34 (12.8)
Serratia marcescens 2 2 4 8 (3.0)
Stenotrophomonas maltophilia 1 4 5 (1.9)
Others 8 3 3 1 15 (5.6)
Anaerobes (%) 1 (25.0) 1 (0.4)
Clostridium difficile 1 1 (0.4)
Fungi (%) 15 (9.3) 15 (5.6)
Candida albicans 4 4 (1.5)
Candida species 9 9 (3.4)
Others 2 2 (0.8)
Total 161 (100) 40 (100) 42 (100) 19 (100) 4 (100) 266 (100)
Abbreviations: UTI, urinary tract infection; BSI, bloodstream infection; PNEU, pneumonia; SSI, surgical site infection.
384일), CRA 11.8±10.3일(3-33일), VRE 48.7±36.0 일(13-85일)이었으나 통계적 유의성은 없었다.
VRE는 E. faecalis 1건, E. faecium이 2건 있었다.
고 찰
국내 중소병원에서의 의료관련 감염률의 발생
률을 기존 국내외 감염률에 대한 연구들과 직접
비교하기에는 감시방법이나 대상의 차이가 있었
다. 중환자실 또는 삽입기구관련 감염 등 부분적
인 비교만이 가능하였다. 중환자실에서의 삽입기
구 감염률을 국내 KONIS 시스템[2]의 400-700병
상규모 중환자실과 미국의 NHSN [8]의 비교육병
원의 15병상 미만 중환자실과 비교하여 보았다.
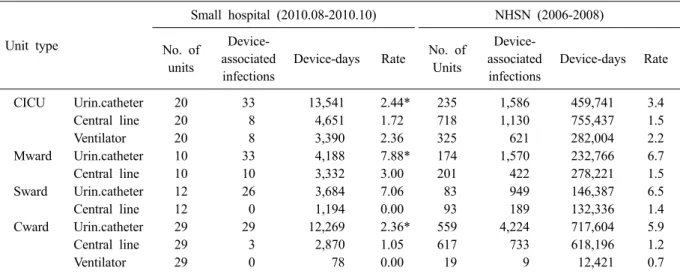
Table 7. Comparison of device-associated infection rate in ICU and general ward amongin small hospital and NHSN
Unit type
Small hospital (2010.08-2010.10) NHSN (2006-2008)
No. of units
Device- associated infections
Device-days Rate No. of Units
Device- associated infections
Device-days Rate
CICU Urin.catheter 20 33 13,541 2.44* 235 1,586 459,741 3.4
Central line 20 8 4,651 1.72 718 1,130 755,437 1.5
Ventilator 20 8 3,390 2.36 325 621 282,004 2.2
Mward Urin.catheter 10 33 4,188 7.88* 174 1,570 232,766 6.7
Central line 10 10 3,332 3.00 201 422 278,221 1.5
Sward Urin.catheter 12 26 3,684 7.06 83 949 146,387 6.5
Central line 12 0 1,194 0.00 93 189 132,336 1.4
Cward Urin.catheter 29 29 12,269 2.36* 559 4,224 717,604 5.9
Central line 29 3 2,870 1.05 617 733 618,196 1.2
Ventilator 29 0 78 0.00 19 9 12,421 0.7
*P value<0.05 compared NHSN.
Abbreviation: NHSN, National Health care Safety Network; CICU, Complex ICU; Mward, Medical ward; Sward, Surgi- cal ward; Cward, Complex ward.
상대적으로 병상규모가 큰 국내의 KONIS 시스 템과 비교 시 중심정맥관 관련 혈류감염률은 사 용비(0.28 vs. 0.43)나 감염률(1.49 vs. 3.55) 모두 유의하게 낮았으며, 유치도뇨관의 사용비는 유의 한 차이가 없었음에도 불구하고 유치도뇨관 관 련 요로감염발생은 낮았다(2.62 vs. 5.92). 반면 인 공호흡기의 사용비는 유의하게 낮았음(0.19 vs.
0.36)에도 불구하고 인공호흡기 관련 감염률의 차이는 없었다. 미국 NHSN과 비교 시 유치도뇨 관의 사용비는 본 연구에 참여한 중소병원 중환 자실이 유의하게 높았고 중심정맥관이나 인공호 흡기 사용비는 유의하게 낮았지만 삽입기구 감 염률에서 유의한 차이는 없었다(Table 6). 간호단 위의 특성을 고려하여 미국 NHSN과 비교하였을 때 유치도뇨관 관련 요로감염에서 유의한 차이 를 보였지만 복합 중환자실과 복합 병동은 낮은 반면, 내과병동은 높았다(Table 7).
대형병원들에 비해 상대적으로 감염관리체계 가 미약한 중소병원 중환자실의 감염률이 기존 KONIS시스템보다 낮았던 것은 의료관련감염의 가장 중요한 위험요인인 유치도뇨관, 중심정맥 관, 인공호흡기와 같은 삽입기구의 사용비가 낮 은 것을 고려할 수 있으나[2,8], 기구사용비와 기 구관련감염률이 일관성 있게 나타나지 않은 것 은(Table 6), 중소병원의 다양한 환자 특성과 짧 은 감시기간의 영향을 배제할 수 없었다.
부위별 병원감염의 분포는 환자군의 특성에 따라 다르다. 요양병원과 같은 재원일수가 긴 병 원들은 상대적으로 요로감염이나, 피부 및 연조 직감염, 혹은 위장관 감염과 같은 기타감염의 분 포가 많아[9-11] 주요 감시대상과 관리대책을 차 별화하여 접근하게 된다. 그러나 본 연구결과에 서는 기타감염의 분포가 적었다. 본 연구의 참여 병원에 요양병원이나 노인병원의 분포가 적었던 것을 고려하여 국내 중소병원의 특징을 대변한 다고 하기에는 무리가 있지만 주요병원감염 중 심으로 감염감시나 감염관리활동을 지속하는 것 이 필요한 것으로 보인다.
의료관련감염의 대부분은 요로감염, 폐렴, 수
술부위감염, 혈류감염[1]이며 이들 감염의 대부
분은 삽입기구와 관련되어 있어 상대적으로 삽
입기구사용비가 높은 중환자실에서 삽입기구관
련 감염이 감염관리의 우선순위가 되어 왔다
[2,8]. 그러나 중소병원의 일반병동은 유치도뇨관
사용비가 중환자실보다 낮음에도 불구하고 유치
도뇨관 관련 요로감염이 높았던 점이나 인공호
흡기 사용이 없는 폐렴의 발생이 일반병동에서
많았던 부분은 중환자실 뿐만 아니라 일반병동
에서도 삽입기구관련감염 감시가 필요함을 제시
하고 있었다. 감염관리 측면에서 볼 때 유치도뇨
관 삽입환자에 대한 감염관리 대상을 중환자실
뿐만 아니라 일반병동까지 확대하는 것이 필요
하며, 폐렴은 인공호흡기 외에도 흡인과 같은 다 른 폐렴의 위험요인이 있는지 확인하여 폐렴예 방을 위한 중재방안[12]의 적용을 고려해야 한다 는 것을 보여주는 결과였다.
의료관련감염에서 분리된 미생물의 내성률이 나 혈액에서 분리된 내성균 감시에서 S. aureus의 methicillin 내성률은 기존 KONIS 시스템이나 대 형병원들과 비슷하였다[1,2]. 그러나 혈액내 내성 균분리환자의 19.3%는 입원 3일 이내에 발생되 어 과거 입원 혹은 타병원과의 관련성을 제기하 고 있었으며, 중소병원의 의료관련감염에서 분리 된 P. aeruginosa와 A. baumannii의 imipenem 내성 률이 낮지만은 않았다. 이러한 결과는 대부분의 국내 병원들이 항생제내성 균주의 관리체계가 부족한 현실[13]을 고려할 때 정부의 적극적 대 책이 필요함을 시사하고 있었다.
27개 병원에서 3개월간 진행한 감염감시로 중 소병원의 의료관련감염 실태를 파악하기에는 제 한점이 있었지만 국내 대형병원에서 진행한 감 시결과와의 차이를 보여주고 있어 중소병원들의 비교분석을 위한 참고자료가 확보되었다는데 의 의를 둘 수 있다.
그러나 중소병원의 다양성과 지원체계의 부족 을 고려할 때 참여병원 및 조사기간의 확대, 참 여병원의 특성을 고려한 비교 프로그램의 개발 이 요구된다. 또한 중소병원의 감염관리에 대한 부족한 기반체계를 고려할 때 인력, 조사체계에 대한 지원방안이 필요하다.
요 약
배경: 본 연구의 목적은 400병상 미만 규모의 중소병원에서의 의료관련감염 현황을 파악하기 위함이다.
방법: 2010년 8월부터 10월까지 27개 병원에 서 웹기반 감시를 진행하였다. 의료관련감염 감 시는 각 병원에서 1-2개의 중환자실과 일반병동 에서 미국 CDC 정의에 의하여 진행하였으며, 다 제내성균주는 모든 혈액배양결과를 조사하였다.
결과: 총 269,436 환자일수 동안 319건의 의료 관련감염이 발생하여 환자일수 1,000일당 1.18건 (CI 1.05-1.32)의 감염률을 보였다. 부위별감염의
분포는 요로감염이 52.4%로 가장 많았으며 폐렴 18.9%, 혈류감염 14.2%, 수술부위감염 7.9%, 기 타 6.6%의 순이었다. 요로감염의 76.5%, 혈류감 염의 46.7%, 폐렴의 18.3%는 삽입기구와 연관성 이 있었다. 전체 감염률은 중환자실에서 일반병 동보다 유의하게 발생률이 높았으나(4.6 vs 0.9), 유치도뇨관 관련 요로감염은 중환자실이 유의하 게 낮았다(2.6 vs 4.4). 중심정맥관(1.5 vs 1.8)이나 인공호흡기관련 폐렴(3.0 vs 0.0)은 중환자실과 일반병동 간에 유의한 차이가 없었다. 원인균주 의 분포는 E. coli 19.8%, S. aureus 13.1%, P. aeru-
ginosa 12.7%의 순이었다. S. aureus의 90.9%가methicillin 내성이었고 P. aeruginosa의 38.2%와 A.
baumannii의 44.4%가 imipenem내성이었다. 혈액
에서 분리된 다제내성균주는 총 66건이었으며, MRSA 84.6% (56주), carbepenem-resistant Acinetob-
acter spp. 10.6% (7주), VRE 4.6% (3주)였다.결론: 본 연구로 파악한 중소병원에서의 의료 관련감염의 특성은 정부의 감염관리 관련 정책 결정시 필요한 기초자료가 되고 참여병원들 간 에 상호비교할 수 있는 감염률 자료를 제공할 수 있을 것이다.
감사의 글
이 연구는 2010년 질병관리본부 학술연구용역 사업인 ‘전국 병원감염감시체계구축: 중소병원’
결과입니다. 참여하여 주신 27개 병원의 모든 연 구자들과 좋은 웹 보고체계를 개발해주신 질병 관리본부장을 비롯한 관계자 여러분께 감사를 드립니다.
참 고 문 헌