Abstract : In many clinical cases such as emergency bronchial asthma attack, methylxanthine bronchodilator, aminophylline may have a beneficial role in the management of asthma. However, aminophylline has a narrow therapeutic index. Also individual variability in the rates of metabo- lism or total clearance has marked an influence on the serum level of the drug.
Generally, the overall liver function declines with age, probably as a result of reduced hepatic mass and blood flow. Therefore, we should carefully monitor mode of action and adverse effect of the drug. At present, we don't have a standard guideline for patients on maintenance dose of aminophylline. In practice, initial dose is decided by the clinical experience and maintenance dose is determined from each patient's hepatic clearance. Consequently, in the study, we aimed to ana- lyze the factors of influencing aminophylline maintenance dose in Korean respiratory lung disease patients.
From April 2004 to September 2005, the initial treatment of the patients had included constant intravenous aminophylline therapy in Seoul National University Bundang Hospital. Subjects were the adult of over 18 years old and had measured serum level in steady state. Also exclusion were made for patients with altered theophylline metabolism (e.g., smoking), drug interactions (e.g., ciprofloxacin), and concomitant disease states (e.g., congestive heart failure, liver cirrhosis).
The subtherapeutic range group had smaller maintenance dose (mg/kg/hr) than the therapeutic
회원학술보고
Aminophylline 클리어런스 및 유지 용량에 영향을 미치는 요인 분석
노주현, 정영미, 남궁형욱, 이병구 분당서울대학교병원 약제부
Analysis of the Factors of Influencing the Clearance of Aminophylline and Maintenance Dose
J.H Rho, Y.M Jeong, H.Y Namgung, B.K Lee
Department of Pharmacy, Seoul National University Bundang Hospital
range group (0.24 ± 0.06 vs 0.33 ± 0.12, t-test, p 0.05). Mean serum level and maintenance dose of aminophylline in therapeutic range were not influenced by sex and obesity but these were high in young subjects (less than 65 year old). No significant difference between young subjects and geriatric subjects (greater than 65yr) was detected in theophylline clearance. Also, it was found that the clearance of theophylline in obese subjects was similar to that of non-obese sub- jects. From this study, it is concluded that obesity (actual body weight/ideal body weight) has to be considered as the factor which affect to the clearance. Maintenance dose of the patient group reached therapeutic range was 0.33 ± 0.12 mg/kg/hr, hence dosage guideline can be set by this result.
[Key words]Aminophylline, Elderly people, Steady state, Clearance, Maintenance dose
연구 배경
Xanthine계 기관지 확장제인 aminophylline은 응급시 천식 치료 약물로 유용하게 사용되며 미숙아 의 무호흡증에도 쓰인다.1~4) 항염증, 면역조절 효과 를 가질 뿐 만 아니라 횡격막의 수축력 증가, 횡격막 의 피로도를 감소시키는 효과를 가진다.5,6) 그러나 aminophylline은 유효 혈중 농도가 5~15 μg/ml로 타 약물에 비해 좁고 약효 및 독성 발현이 혈중 theophylline농도와 상관관계를 가질 뿐만 아니라 약동학적 파라미터의 개인차가 크므로 therapeutic 혈중 농도 모니터링이 필요한 약물이다.3,7)특히 연령 이 증가할수록 hepatic mass 및 blood flow의 감 소로 인해 간 대사의 활성이 낮아질 뿐만 아니라 기 저 질환과 병용 약물이 증가하므로 반응과 부작용을 주의깊게 관찰하여야 한다.3,6)현재 aminophylline 을 주사 투여할 때 표준화된 가이드라인이 없는 실정 이며, 실제 임상에서는 초기 용량을 경험적으로 결정 하여 투여한 후 혈중 농도가 치료 영역 이하이거나 이상일 경우 용량 조절을 하여 유지 용량을 설정한 다. 이에, 이번 연구에서는 실제 임상 환경에서 호흡 기 질환을 가진 환자를 대상으로 theophylline의 clearance 및 aminophylline의 유지 용량을 구하 고 이에 영향을 주는 요인을 분석하고자 하였다.
대상 환자 및 연구 방법
2004년 4월 1일부터 2005년 9월 30일까지 분당 서울대학교병원에서 aminophylline을 등속 점적정 맥 주입하고 steady-state에서 혈중 농도를 측정한 18세 이 상 의 성 인 중 theophylline TDM (Therapeutic Drug Monitoring)을 의뢰한 환자를 대상으로 전자의무기록(Electronic Medical Record) 자료를 바탕으로 후향적으로 조사하였다.
Non-steady state에서 채혈한 경우, 울혈성 심부 전, 간경화 등 theophylline clearance에 영향을 미치는 질환이 있는 경우, 흡연 환자, hemody- namic state가 불안정할 것으로 추정되는 중환자, 투여 방법의 오류도 제외하였다. 또한 theophylline 과 약물 상호작용이 있는 것으로 알려진 ciproflox- acin, propafenone, cimetidine, erythromycin, rifampicin, phenytoin 등의 약물을 병용한 경우도 대상환자에서 제외하였다. Aminophylline을 infusion pump로 점적 정맥 투여하였고 steady state에서 채혈한 검체는 Abbott AxSym 기기를 통해 혈중 농도가 측정되었다. 실제 대상 환자의 clearance는 infusion rate (K)와 steady state에 서의 혈중 농도(Cp)로부터 계산하였다. 이 때 적정 치료 혈중 농도 범위는 5~15 μg/ml으로 설정하였으 며 환자의 체중은 ideal body weight을 사용하였 다. 단 actual body weight가 ideal body weight
보다 작은 경우에는 actual body weight을 사용하 였다.
통계학적 분석 방법은 연령, 성별, 비만도와 clearance와의 관계를 구하고 연령, 성별, 비만도와 유지 용량 간의 관계를 구하였다. 분석 방법은 SPSS ver 12.0을 이용하였고 p값이 0.05이하일 경우 유 의성이 있다고 정의하였다.
결과
1. 환자 특징
연구기간 내에 aminophylline 투여 중 혈중 농도 를 측정한 성인 환자 143명 중 연구 대상 환자는 총 78명이었다. 평균 혈중 농도는 8.16 ± 3.61 μg/ml이 며 투여 용량은 0.32 ± 3.61 mg/kg/hr이었다. 적응 증은 asthma, COPD가 대부분을 차지하였다(Table 1). 제외 대상 환자는 non-steady state에서 채혈한 경우(30명), 울혈성 심부전, 간경화 등 theophylline clearance에 영향을 미치는 질환이 있는 경우(9명),
흡연 환자(9명), hemodynamic state가 불안정할 것으로 추정되는 중환자실 환자(11명), 사망 환자(2 명), 투여 방법의 오류(3건)도 제외하였다. 또한 theophylline의 대사에 영향을 미치는 약물을 병용 한 경우(3명)도 대상 환자에서 제외하였다.
2. 혈중 농도 분포
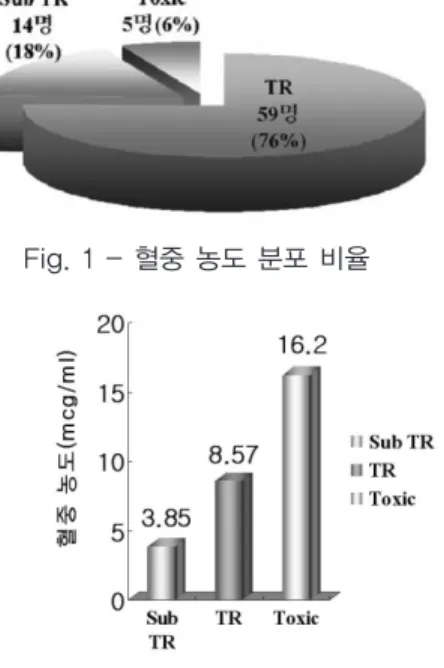
대상 환자 78명 중 therapeutic range군은 59명 (76%)으로 가장 많았고 subtherapeutic range군 은 14명(18%)이었으며 toxic range군은 5명(6%)이 었다(Fig. 1). 각 군의 평균 혈중 농도는 subthera- peutic range군이 3.85 ± 0.77 μg/ml, thera- peutic range군은 8.57 ± 2.57 μg/ml이며 toxic range군은 16.2 ± 1.89 μg/ml이었다(Fig. 2).
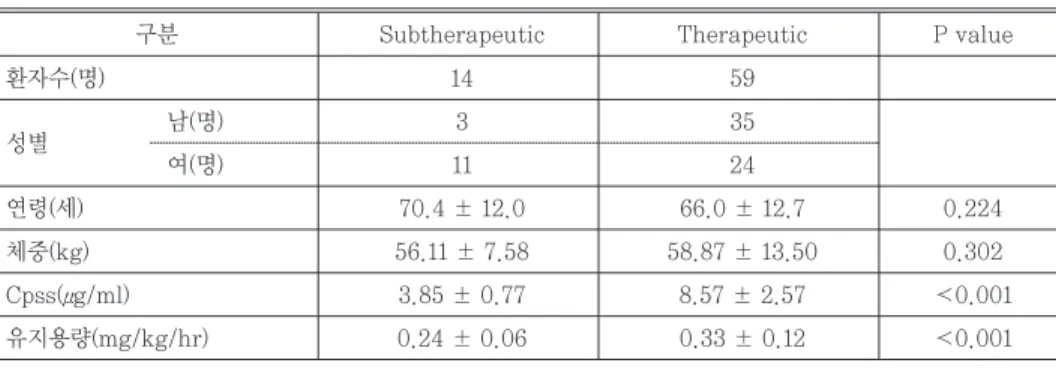
Table 2는 혈중 농도의 분포에 따른 환자 특성을 나타낸 것이다. Therapeutic range군의 혈중 농도가 subtherapeutic range군보다 유의하게 높았으며 thera- peutic range군의 유지용량이 subther- apeutic range군보다 유의하게 컸다.
Therapeutic range 군에 비해 subther- apeutic range군의 연령이 높았다.
CL: clearance (ml/kg/hr) K0: infusion rate (mg/kg/hr)
Cpss: steady state에서의 혈중 농도(μg/ml) CL= K0×0.8
Cpss
Table 1. 환자 특징
구분 명(%) 평균(mean SD)
환자수(명) 78
연령(세) 67.0 ± 12.6
남 41(53)
여 37(47)
체중(kg) 54.4 ± 7.4
Cpss(μg/ml) 8.16 ± 3.61
유지용량(mg/kg/hr) 0.32 ± 0.13
적응증
Asthma 40(52)
COPD 26(33)
기타 12(15)
SD: Standard Deviation
Fig. 1 - 혈중 농도 분포 비율
Fig. 2 - 각 군의 혈중 농도 성별(명)
Table 2. 혈중 농도 분포
구분 Subtherapeutic Therapeutic P value
환자수(명) 14 59
성별 남(명) 3 35
여(명) 11 24
연령(세) 70.4 ± 12.0 66.0 ± 12.7 0.224
체중(kg) 56.11 ± 7.58 58.87 ± 13.50 0.302
Cpss(μg/ml) 3.85 ± 0.77 8.57 ± 2.57 0.001
유지용량(mg/kg/hr) 0.24 ± 0.06 0.33 ± 0.12 0.001
(mean ± SD)
구분 65세 미만 65세 이상
환자수, 명(%) 22(37) 37(63)
성별, 명(%) 남 10(17) 25(43)
여 12(20) 12(20)
연령(세) 52.4 ± 2.4 73.7 ± 0.9
체중(kg) 54.6 ± 1.7 55.1 ± 1.3
Table 3. 치료 혈중 농도 범위의 환자 특성 3. 치료 혈중 농도 범위의 환자 특성
Therapeutic range에 속한 환자 59명에서 65세 미만과 65세 이상으로 구분해 보았다. 평균 연령은
65세 이상군이 73.7세이고 65세 미만군이 52.4세이 었으며 두 군 간의 체중에는 큰 차이가 없었다 (Table 3).
65세 미만 군의 클리어런스는 33.41 ± 8.28 ml/kg/hr으로 65세 이상 군 보다 다소 높게 나왔으 나 유의한 차이는 없었으며 성별에 따른 클리어런스 에도 유의한 차이는 없었다. Actual body weight 과 ideal body weight의 비가 1.2 이상인 과체중군 의 클리어런스는 1.2 미만인 정상체중군에 비해 다 소 높았으며 유의성이 경계 수준에 있었다. 65세 이
상 군에 비해 65세 미만 군에서 더 큰 유지 용량이 투여되고 더 높은 혈중 농도가 측정되었다. 성별에 따른 유지 용량에는 유의한 차이가 없었다. 과체중군 이 0.34±0.08 mg/kg/hr로 더 큰 유지 용량으로 투여되고 더 높은 혈중 농도가 측정되었으나 유의한 차이는 없었다(Table 4).
4. 부작용
Aminophylline을 지속적으로 투여한 환자 중에서 aminophylline으로 인한 심각한 부작용을 호소하 는 환자는 없었으며 투여 후 headache를 호소하는 환자가 toxic range 군에서 1명 있었다.
고찰
지금까지의 theophylline의 약물 동력학적 연구는 경구 투여 시에 이루어졌다. 그러나 실제로는 입원환 자에게 천식이나 COPD의 급격한 증상 악화를 완화 시킬 목적으로 aminophylline IV를 투여하였으며 입원 환자의 경우 증상이 호전되면 경구로 전환하게 된다. 특히, 연령에 증가함에 따라 glomerular fil- tration rate, hepatic enzyme activity, serum albumin, protein binding 등과 같은 약물동력학 적 인자가 변한다. 이와 같이 노인환자의 경우 앞서 말한 여러 인자 변화와 다중약물요법으로 인해 theophylline의 약물 동태학적 변화를 예측하기가 어렵다.9) 또한 aminophylline의 IV 투여는 Neilsen-Kudsk 등8)에서 Vd의 감소로 인해 독성이 더 증가한다고 보고하였으며 aminophylline IV 투 여를 유지하는 경우 환자의 임상학적 상태가 불안정 한 경우가 많으므로 유지 용량을 설정하는 가이드라
인이 필요한 실정이다.
연령에 따른 theophylline 클리어런스의 연구 중 Bauer 등,10)Y. Horai 등11)은 연령에 따른 클리어런 스에 유의한 차이가 없다고 발표하였다. Akihiro 등,3) Muhlberg W 등12)의 연구에서는 정상 성인에 비해 노인 환자의 클리어런스가 감소되었다는 다른 결론을 내리고 있다. 본 연구에서는 연령에 따른 클 리어런스에 유의한 차이가 없었으나 실제 65세 이상 노인 환자의 aminophylline 유지 용량이 65세 미만 의 환자보다 적게 유지되고 있었으며 혈중 농도도 노 인 환자에게서 낮게 유지되고 있었다. 이는 amino- phylline을 노인 환자의 경우 각 환자의 임상적 상 태나 drug elimination activity를 고려하지 않고 연령을 주로 고려하여 용량을 줄이려는 방향으로만 전개된 것으로 사료된다.
또한 성별에 따른 theophylline 클리어런스의 연 구 중 Jennings 등13)은 성별에 따라 theophylline metabolism, clearance에 유의한 차이가 있다고 발 표한 반면에 Y. Horai 등11)은 성별과 클리어런스 간 에 유의한 관계가 없다고 하였다. 본 연구에서는 성 별이 클리어런스 변화와 상관관계를 가지지 않았다.
Zahorska-Markiewicz B 등14)은 16명의 비만 환 자에게서 weight reducing treatment를 시행하면 서 theophylline의 pharmacokinetics을 조사한 Table 4. 치료 혈중 농도 범위의 혈중 농도, 클리어런스, 유지 용량
구분 Cpss(μg/ml) Clthe(ml/kg/hr) 유지 용량(mg/kg/hr)
연령
65세 미만 9.87 ± 0.46 33.41 ± 8.28 0.41 ± 0.13
65세 이상 7.81 ± 0.42 30.76 ± 11.62 0.29 ± 0.10
P value 0.002* 0.327 0.013*
성별
남 9.21 ± 2.85 31.32 ± 7.26 0.36 ± 0.13
여 8.01 ± 2.29 29.69 ± 8.90 0.31 ± 0.11
P value 0.328 0.364 0.108
비만도(ABW/IBW)
1.2 8.10 ± 2.45 29.69 ± 8.50 0.29 ± 0.89
≥1.2 10.22 ± 2.35 36.40 ± 13.96 0.34 ± 0.08
P value 0.453 0.053 0.794
(mean ± SD)
결과 clearance는 감소하고 반감기는 증가하므로 비만 환자는 aminophylline 용량 설정 시 ideal body weight을 이용해야 한다고 발표하였다.
Anon 등15)은 theophylline이 fat-free tissue에 분포되므로 ideal body weight을 사용해야 한다고 결론을 내렸다. 그러나 본 연구에서는 과체중군의 클 리어런스가 정상 체중군에 비해 유의하게 높지 않았 으나 p값이 경계 수준에 있었다.
본 연구에는 몇 가지 제한점을 지적할 수 있는데 첫 째로 적은 환자 수로 인하여 연령, 성별, 비만도 등 여러 인자의 통계학적 유의성을 확인하기가 어려웠 다. 두 번째로 aminophylline IV 투여는 천식이나 COPD의 증상이 악화된 환자가 대부분이므로 환자 의 내인성 클리어런스 변화에 따른 편차가 크므로 한 번의 혈중 농도 측정으로는 정확한 theophylline clearance를 산출하는데 제한이 따른다.
결론
Therapeutic range에 도달한 환자 군의 유지 용 량은 본 연구에서 0.33 ± 0.12 mg/kg/hr로 측정 되었다. 이를 토대로 aminophylline의 초기 용량 가이드라인 설정이 가능하지만 노인 환자의 적절한 aminophylline 용량 결정을 위해서 추가적인 TDM 이 권장된다. 그 외에 clearance에 영향을 미치는 인자로 비만도를 고려할 필요가 있을 것으로 사료된 다. 또한 유지 용량의 확실한 가이드라인을 마련하기 위해서는 후속적인 연구가 필요할 것이다.
참고 문헌
1. Aminophylline for the prevention of apnea during prostaglandin E1 infusion.
Pediatrics. 2003;112:e27~29
2. Treatment of apnea of prematurity.
Pediatr Drugs.2003;5(3):195~210
3. Differential pharmacokinetics of theo- phylline in elderly patients. Drugs Aging.
2003; 20: 71~84
4. Should aminophylline be abandoned in the treatment of acute asthma in adults?
Q J Med 2000;93:761~765
5. Therapeutic responses in asthma and COPD: Bronchodilators. Chest. 2004; 126:
125S~137S
6. Drug therapy: Theophylline in asthma.
1996; 334(21): 1380~1388
7. Apparent decrease in population clear- ance of theophylline: Implications for dosage Clin Pharmacol Ther.
1997;62(5):483~489
8. Pharmacokinetics of theophylline on ten elderly patients. Acta Pharmacol Toxicol.
1978; 42: 226~234
9. Theophylline pharmacokinetics in normal elderly subjects. Clin Pharmacol Ther.
1988; 44:522~30
10. Influence of age on theophylline clear- ance in patients with chronic obstructive pulmonary disease. Clin Pharmaco- kinet. 1981; 5: 469~474
11. Individualized aminophylline therapy in patients with obstructive airway disease:
Oral dosage prediction froom an intra- venous test dose. Eur. J. Clin Pharmcol.
1982; 23: 111~121
12. Pharmacokinetics and pharmacodynamics of theophylline in geriatric patients with multiple diseases. Klin Wochenschr.
1987;65(12):551~7
13. Gender differences in hepatic induction and inhibition of theophylline pharma- cokinetics and metabolism. J Lab Clin Med. 1993; 122(2):208~16
14. Pharmacokinetics of theophylline in obesity.
Int J Clin Pharmacol Ther. 1996;34(9):393~5 15. Theophylline intravenous labeling guidelines, Memorandum from the Department of Health and Human Services, Washington, DC, 1995a.
16. Theophylline kinetics in a geriatric
group. Clin. Pharmacol. Ther. 1983;
34(1): 61~67
17. Theophylline kinetics in relation to age:
the importance of smoking. Br. J. clin.
Pharmc.1980; 10: 109~114
18. Theophylline의 malabsorption. 병원약사회 지.1995;12(3):216~220