Received September 4, 2014, Revised September 22, 2014, Accepted September 22, 2014 Corresponding author: Hi-Joon Park
Department of Meridian and Acupoint, College of Korean Medicine, Kyung Hee University, 26 Kyungheedae-ro, Dongdaemun-gu, Seoul 130-701, Korea Tel: +82-2-961-9435, Fax: +82-2-963-2175, E-mail: [email protected]
This research was supported by Basic Science Research Program through the National Research Foundation of Korea(NRF) funded by the Ministry of Education, Science and Technology(No. 2005-0049404) and a grant of the Korean Health Technology R&D Project, Ministry of Health and Welfare, Republic of Korea(HI13C0540).
CCThis is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/ by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Different Responses to Acupuncture in
Electroencephalogram according to Stress Level:
A Randomized, Placebo-Controlled, Cross-Over Trial
Song-Yi Kim1,2,3, Sang-Woo Kim3, Hi-Joon Park1,2,3
1Acupuncture and Meridian Science Research Center(AMSRC),
2Korean Medicine Convergence Research Information Center(KMCRIC),
3Department of Meridian and Acupoint, College of Korean Medicine, Kyung Hee University
스트레스 정도에 따라 침 치료가 뇌파(EEG)에 미치는 영향:
무작위배정 플라시보 대조군 교차연구
김송이1,2,3ㆍ김상우3ㆍ박히준1,2,3
1경희대학교 침구경락과학연구센터, 2경희대학교 한의약융합연구정보센터, 3경희대학교 한의과대학 경혈학교실
Objectives : The purpose of this randomized, placebo-controlled, cross-over trial was to examine how acupuncture treatment at Shinmun(HT7) affects the brain activity and the autonomic nervous system(ANS), using electroencephalograms(EEG) and heart rate variability(HRV). Methods : Eighteen healthy volunteers participated in two separate experiments: in each experiment, either real acupuncture(RA) or non-penetrating sham acupuncture(SA) was applied at HT7 in random sequences to each person. The EEG and HRV measurements were conducted simultaneously before and during the acupuncture stimulation for 5 minutes, respectively. Resulting EEG and HRV parameters were compared between RA and SA groups. To assess differences according to the stress levels for participants, subgroup analysis was performed based on the results of the stress response index questionnaire.
Results : In the results, acupuncture stimulation at HT7 increased α band in EEG. In the HRV analysis, heart rate was decreased significantly but HF and RMS-SD were increased in the RA group, compared with those of the SA group. In the subgroup analysis by stress level, participants in the RA group with high stress exhibited an increased in α band in their EEG while the low stress participants showed decrease or little increase in the band. For the SA group, α band reported relatively moderate changes in all channels. Conclusions : Our results showed that acupuncture induces changes in brain activation and the ANS. Acupuncture was related to the activation of the parasympathetic nervous system. The brain activities of the participants were different depending on the stress level.
Key words : acupuncture, ANS, brain activity, EEG, HRV
Introduction
Acupuncture follows the paradigm of traditional East Asian medicine, in which insertions of needles at specific points called acupuncture points on the meridian regulate and treat symptoms of illnesses1). Current research explores the use of acupuncture to reduce chronic pain as well as cancer and mental illnesses2). A variety of mechanisms within acupunc- ture have been developed: immunological and hormonal approaches3-5); physical approaches in connective tissue6); neurological approaches such as release of specific neuro- peptides in the central nervous system7); fMRI for neuro- imaging8,9). Especially with fMRI, SPECT, PET and other imaging techniques, acupuncture researchers are stimulating different functional aspects of the brain during the structural mapping process. Among them, electroencephalogram(EEG) transmits electrical impulses from the nerves in the brain non-invasively to measure the activity and state of the brain.
The frequency ranges of EEG include θ, β, α: normal α activity represents slower frequency activity in the brain, such as when the brain is relaxed and stable while the low amplitude, high Hz waveforms like β activity signify an in- crease of arousal and stress10). In addition, Yu et al.’s11) research show that by inducing stress artificially by assigning a mental arithmetic task, there was a reduction in the power components of the α band and a marked linear increase in the β band of the parietal and occipital regions.
Previous studies reported that acupuncture stimulation at an acupuncture point on the right trapezius muscle increased α and θ activity12), and another study showed that power band below 13 Hz was increased after scalp and auricular acupuncture13). Acupuncture at PC6 elicited an increased in all the frequency bands14). On the other hand, Streitberger et al.15) observed an increased in the α1 band(1.25∼4.50 Hz) when comparing LI4 acupuncture stimulation and sham acupuncture, but did not observe any changes in the remaining δ, β, α2 band(9.75∼12.50 Hz). There are se- veral factors in the actual acupuncture procedure that affect EEG results. Chen et al.16) found that in the case of elec- troacupuncture, the activity of the different powers de-
pended on the frequency level of electroacupuncture(200 Hz or 2 Hz). Another finding showed significant changes of α, β, or θ band power in relation to the acupuncture sensation17).
In addition, neural mechanisms in the autonomic nervous system(ANS) have been proposed18-20). These studies explored the use of HRV as a tool to measure the activity and response of sympathetic and parasympathetic nerves in the regulation of cardiovascular activity. Until recently, research has shown that, in normal subjects, acupuncture has a tendency to cause the acceleration of the parasympathetic nervous system. In addition, stimulating different acupuncture points caused opposing results. For subjects under experimentally-stressed conditions, their imbalanced ANS were able to recover through acupuncture treatment, and their excited sympa- thetic nerves tended to return to normalcy21).
Although two reviews21,22) concluded that the relationship between acupuncture and ANS response results is uncertain, there are two controversial issues to be considered about acupuncture research. First, most of the included studies used penetrated, minimal acupuncture stimulation for the control groups instead of non-invasive sham/placebo acupuncture. In these ways, a similar level of physiological changes for the control and experimental groups may be induced. Secondly, acupuncture is normally administered to patients as treatment for an illness, and not to healthy individuals for observation;
therefore, a healthy group as control subjects may be un- suitable. The second set of factor that requires consideration is the status of subjects.
The objective of our research was to examine how the acupuncture treatment at Shinmun(HT7), believed to reduce stress levels and control psychological stability, affects the brain activity and the sympathetic nervous system using EEG and HRV. Using a cross-over design, this study considered the effects of the abovementioned limiting factors and the decrease of individual’s physiology when given sham acu- puncture. Because we used healthy individuals for our study, we measured the stress level of each using a sensitivity analysis to see if there were any changes in stress levels throughout the trials.
Fig. 1. Protocol of experiment.
aA needle manipulation involving twirling the needle to produce the desired effect. EEG : electroencephalogram, HRV : Heart rate variability;
min, minutes; sec, seconds.
Materials and Methods
1. Study design
The research was conducted using a cross-over design in which each participant received RA and SA in two sessions in a randomized order. Each participant made two visits: in the first, they were administered RA or SA, and asked to come in 1∼3 days later for the alternate treatment. If, for any reason, participants omitted a visit to the treatment or obtained data has problems with analysis, they were excluded from the study.
2. Participants
The study recruited eighteen healthy 20∼30 year-old male volunteers who had no history of neurological illnesses.
Individuals with history of cardiac and vascular disorders such as hypertension, arrhythmia, conduction disorder, is- chemic heart disease, diabetes, thyroid illness, and endocrine problems were excluded from the experiment. Cases in which individuals were taking medicine or under the in- fluence of substances were also excluded. Participants were required to refrain from consuming caffeinated or alcoholic beverages and from smoking for the 12 hours preceding experiment. All participants were briefed on the experi- mental procedure and asked to sign an agreement to volun- teer prior to participation. All procedures were in compliance with the Declaration of Helsinki for human subjects.
3. Intervention
An experienced Korean Medicine Doctor inserted a needle at the acupuncture point HT723) bilaterally, which is located on the tendon of flexor carpi ulnaris located above the palmar wrist crease on the anterior region of the wrist. For
the RA group, a standard 0.20×40 mm needle(DongBang Acupuncture Inc., Korea) was inserted perpendicularly 5 mm deep. The twirling method was used for thirty seconds during which the needle was twisted every second followed by needle retention for five minutes to prolong the effect. The same technique at the HT7 was applied to the SA group without penetration of skin using a Park Sham needle. After acupuncture stimulation, all participants were wiped with rubbing alcohol, and bandaged to maintain the blinding. The Acupuncture Sensation Questionnaire(ASQ)24) was admini- stered to measure the experience of deqi in addition to the visual analogue scale(VAS) to measure the pain and stress caused by acupuncture treatment.
4. Outcome measures and statistical analysis Participants were asked to complete a basic questionnaire which recorded the demographics, physical condition and Stress Response Inventory(SRI: 39-question self-reported mea- surement) in their first visit. The participants were allowed to rest for ten minutes before treatment. Their EEG and HRV were measured before and during the administration of acupuncture a total of two times for five minutes each(Fig.
1). During the measurements, they were seated on a chair with a back and foot stool, asked not to move and to focus their eyes straight ahead.
We used a 32-channel digital electroencephalogram sys- tem(Neuonics32, Intermed Co., Seoul, Korea)25) to record the EEG signals. An EEG recording cap with 32 Ag/AgCl elec- trodes was placed on the subjects’ heads to allow for fast and exact placement of the electrodes in a 10∼20 system.
Skin impedance was usually kept lower than 5 kV for each session, and the measurements were taken for 5 minutes at a sampling rate of 256 Hz. The earlobe served as the
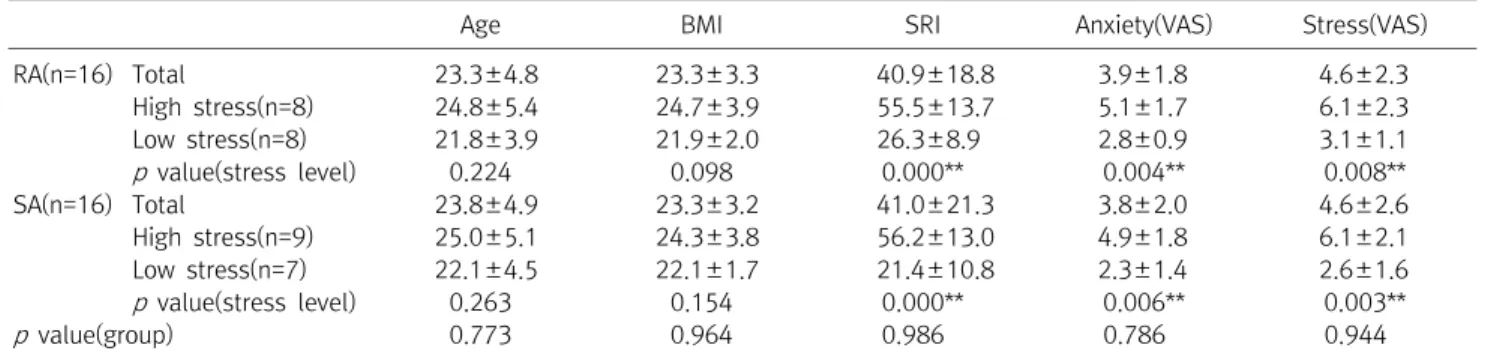
Age BMI SRI Anxiety(VAS) Stress(VAS)
RA(n=16) Total 23.3±4.8 23.3±3.3 40.9±18.8 3.9±1.8 4.6±2.3
High stress(n=8) 24.8±5.4 24.7±3.9 55.5±13.7 5.1±1.7 6.1±2.3
Low stress(n=8) 21.8±3.9 21.9±2.0 26.3±8.9 2.8±0.9 3.1±1.1
p value(stress level) 0.224 0.098 0.000** 0.004** 0.008**
SA(n=16) Total 23.8±4.9 23.3±3.2 41.0±21.3 3.8±2.0 4.6±2.6
High stress(n=9) 25.0±5.1 24.3±3.8 56.2±13.0 4.9±1.8 6.1±2.1
Low stress(n=7) 22.1±4.5 22.1±1.7 21.4±10.8 2.3±1.4 2.6±1.6
p value(stress level) 0.263 0.154 0.000** 0.006** 0.003**
p value(group) 0.773 0.964 0.986** 0.786** 0.944**
BMI : Body mass index (kg/m2), RA : Real acupuncture, SA : Sham acupuncture, SRI : Stress response inventory, VAS : Visual analogue scale.
Data was reported by Mean±SD. **p<0.001.
Table 1. Baseline Characteristics
reference, and the frontal lobe served as the ground. EEG signals were filtered and artifacts were reduced using Neuonics32, Intermed Co.’s neural network, digitally. The EEG data were exported and processed after extraction of α and β band intensities using fast Fourier transformation process. Our analyzed bands were divided into following spectral ranges: α, β set at 8∼12, and 13∼30 Hz, res- pectively.
HRV was measured using an electrocardiogram ampli- fier(Heart Rhythm Scanner; Biocom Technologies, USA). In order to record HRV, electrodes were placed on the chest at 256 samples/sec and the rates of extraction for each individual was recorded. The gathered information was analyzed under time-domain and frequency-domain as a low-frequency band(LF component; 0.04∼0.15 Hz) and a high-frequency band(HF component; 0.15∼0.40 Hz), which reflected the sympathovagal balance. From the relative con- tribution of the LF and HF components(LF/HF ratio), heart rate, total power, standard deviation of NN interval(SDNN), very-low-frequency(VLF) component, and square root of the mean squared differences of successive normal to normal interval(RMS-SD) were calculated.
The EEG and HRV were the main outcome measures for any changes between real and sham acupuncture treatments.
In addition, the changes after treatments were compared in accordance to stress level by the median of the SRI scores.
Our data were statistically analyzed using SPSS. All results were recorded as mean±standard deviation, and pre/post-
treatment t-tests were assayed with p<0.05. An acupuncture sensation correlation was analyzed using the Spearman correlation test.
Results
1. Baseline characteristics and Stress Response Inventory(SRI) data
In total, 18 participants were recruited, but among them, four or three participants were excluded from EEG or HRV analysis of present study due to absences or data error. This was the case for 2 participants in the RA and 2 for the SA leaving a total of 16 in the RA and 16 in the SA group for EEG analysis. In the HRV analysis, 16 participants remained in RA and 17 in the SA group. The demographic data for the 16 participants based on the EEG analysis are provided on Table 1. There were no significant differences in the baseline characteristics between the two groups. Analysis of the SRI results showed that the participants’ median SRI data was 43.
This data was used to divide the participants into high and low stress groups(RA/high stress: n=8; RA/low stress: n=8;
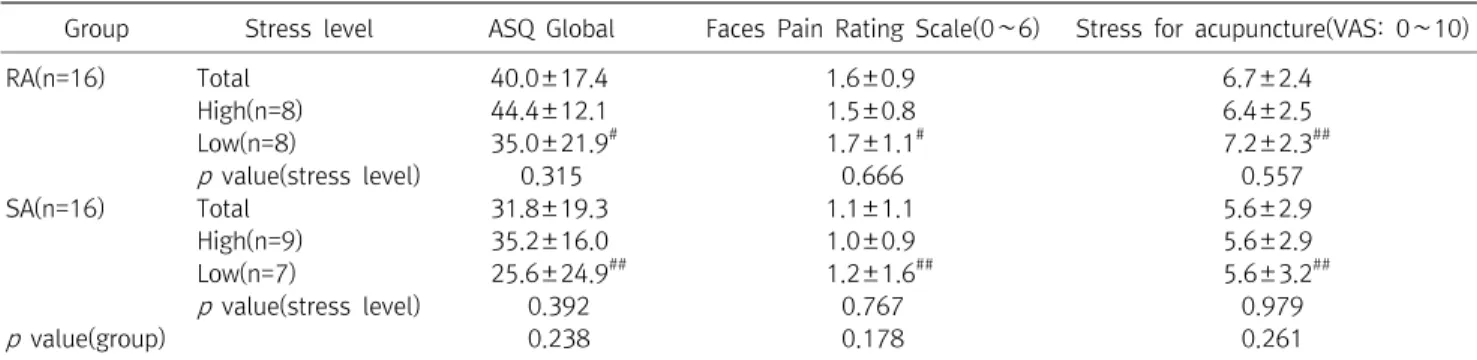
SA/high stress: n=9; SA/low stress: n=7). The acupuncture sensation(deqi experience) as well as the pain and stress for acupuncture were not statistically different in either the RA or SA groups. This pattern is the same in the different participant’s stress level(Table 2).
Group Stress level ASQ Global Faces Pain Rating Scale(0∼6) Stress for acupuncture(VAS: 0∼10)
RA(n=16) Total 40.0±17.4 1.6±0.9 6.7±2.4
High(n=8) 44.4±12.1 1.5±0.8 6.4±2.5
Low(n=8) 35.0±21.9# 1.7±1.1# 7.2±2.3##
p value(stress level) 0.315 0.666 0.557
SA(n=16) Total 31.8±19.3 1.1±1.1 5.6±2.9
High(n=9) 35.2±16.0 1.0±0.9 5.6±2.9
Low(n=7) 25.6±24.9## 1.2±1.6## 5.6±3.2##
p value(stress level) 00.392 0.767 0.979
p value(group) 00.238 0.178 0.261
ASQ : Acupuncture sensation questionnaire, RA : Real acupuncture, SA : Sham acupuncture, VAS : Visual analogue scale.
#One participant did not answer, ##Two participants did not answer.
Table 2. Comparisons of Acupuncture Sensation(Deqi)
Fig. 2. Change rates of EEG values during acupuncture.
(A) Alpha band, (B) Beta band. There were no statistical diffe- rences between groups by independent t-test.
Fig. 3. Change rates of HRV parameters during acupuncture.
HRT : Heart rate, SDNN : Standard deviation of all R-R intervals, LF/HF : Low frequency/high frequency ratio, VLF : Very low fre- quency, LF: Low frequency, HF : High frequency, RMS-SD : Root mean square successive difference. *p<0.05; **p<0.005 by independent t-test.
2. Change in EEG induced by acupuncture
Before acupuncture stimulation, there were no differences in α and β band of EEG between two groups(p>0.05). In general, α and β bands for RA and SA group in all channels of brain increased during the administration of acupuncture, but the changes were not statistically significant(Fig. 2). The α band on most channels, excluding T7 and TP7, showed a more increase in the RA group compared with those of the SA group. On the contrary, there was a trend of greater increase in the β band for the SA group compared with RA group.
3. Change in autonomic functions using HRV data analysis
The HRV data for both RA and SA groups were similar before acupuncture administration(p>0.05). The change in rates of HRV parameters after acupuncture, specifically the mean heart rate(HRT), HF, and RMS-SD, were statistically different between groups(Fig. 3). The HRT was -3.4±2.7% for the RA group, and -1.0±1.9% for the SA group. The HF in the RA was 43.9±64.6% but in the SA was 2.9±46.5%. The RMS-SD in the RA group showed a change of 20.3±19.7%, but the sham group, 5.6±10.4%. Each of the changes showed that administration of acupuncture decreases heart rate, and accelerates the parasympathetic nervous system.
A
B
Fig. 4. Change rates of EEG data (alpha and beta band) based on different stress levels.
(A) Alpha band of real acupuncture, (B) Alpha band of sham acupuncture, (C) Beta band of real acupuncture, (D) Beta band of sham acupuncture. *p<0.05 by independent t-test.
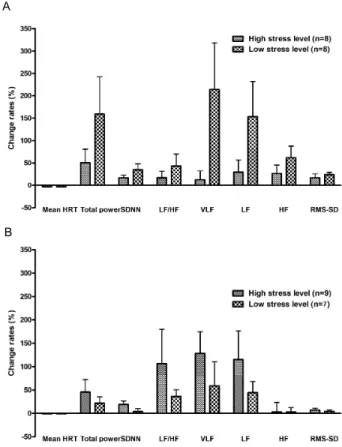
Fig. 5. Change rates of HRV data based on different stress levels.
(A) Real acupuncture, (B) Sham acupuncture. There were no sta- tistical differences between groups by independent t-test.
4. Relationships between changes in EEGs and HRV data and stress level
EEG results indicate a marked difference in α band of the high and low stress groups that received RA. The high stress group exhibited a marked change in all channels after acupuncture stimulation. The strong tendency to increase indicated in the C3(independent-sample t-test, p=0.043), OZ(0.041), and O2(0.049) channels. But the low stress groups exhibited decrease or little increase after acupuncture
administration(Fig. 4A). On the contrary to RA, after SA stimulation, α band reported relatively moderate changes in all channels(Fig. 4C). In case of β band, RA did not lead to significant changes of β band in both stress level(Fig. 4B).
But SA group showed more increased β band changes, but it was not significant(Fig. 4D).
Fig. 5 indicated the change rates of HRV data based on different stress levels after acupuncture stimulation. The results were diverse according to stress level and type of acupuncture. For example, RA generated more increases of HRV related factors in low stress group, but SA produced in high stress level, although they were not statistically signi- ficant.
There was no correlation between deqi sensation and the EEG or HRV results.
A
B
C
D
A
B
Discussions
In the present study, acupuncture stimulation at HT7 increased band intensities of α frequency in EEG. In the HRV analysis, heart rate was decreased significantly but HF and RMS-SD were increased in the RA group compared with those of the SA group. These results show that acupuncture stimulation at HT7 stabilizes changes in brain activation and that through the regulation of the ANS, the parasympathetic nervous system can be activated. These results were espec- ially notable in the subgroup analysis by stress level. In the RA group, participants with high stress exhibited an increased in α band in their EEG patterns while the low stress participants showed decrease or little increase in the band. For the SA group, α band reported relatively moderate changes in all channels, and low stress individuals showed little change or a decrease while the high stress participants increased. Acupuncture at HT7 affects the brain activity of the participants differently depending on the stress level, which shows each individual’s reaction tends to rely on his or her current condition.
The HT7 which was employed in this study has been used for neurological or psychiatric disorder, clinically. Acupun- cture treatment at HT7 activates parasympathetic nerve26); works on stress levels with decreasing tachycardia induced by stress27); decrease the resting heart rate28); improve insomnia29); effective for depression induced maternal se- paration in animal study30,31) and for anxiety-like behavior following nicotine withdrawal32). Therefore, we hypothe- sized that stimulations of HT7, which is used on the psy- chological and nerve problems would have an effect on the stress levels of participants.
Although there are existing studies that observe the effects of treatment on the different acupuncture points or compare the types of treatments used, there are few that look at the individual differences. Several research findings showed that there was a correlation between the individual’s heat and cold tendency and the change in HRV’s LF33) as well as brain activity34). These results were attempts to show that there were different physiological responses induced by individual
variations. The individual variations might be due to the un- balanced yin-yang in the individuals, which can be reba- lanced by readjusting the participant’s qi.
In our study, we have designed a protocol to observe the individual variations for mild case of symptoms such as stress.
Stress, often used as a psychological term, influences both the emotional and physical health of an individual. Stress can be a cause, while a stressor induced physiological and behavioral responses35), and it can be defined as a kind of maladjustment to one’s environment. From our study that depicted an inverse relationship between perceived stress and the HF component of HRV, it was observed experimentally that stress influences the cardiac-vagal modulation of the indi- vidual36). Stress induces negative symptoms from headaches to an increase in heart rate and may even develop into risk factor for an illness. Also, this risk factor for illness has sometimes been interpreted as relationship between action of stress in the brain and related hormone such as glu- cocorticoid, epinephrine, cortisol35,37). Our study applied st- ress level to establish unbalanced condition, instead of pain model, which had been used in previous acupuncture studies.
In spite of this encouraging new approach, the current stan- dard of measuring stress levels is controversial. It was too ambiguous thing to measure and divide stress level although we made every effort to use validate questionnaire. The SRI questionnaire’s validity test showed the scores for healthy subjects as 68.5±23.4, and patients with anxiety disorders 87.1±31.6, depressive disorder 109.2±34.8, somatoform disorder 94.1±32.5, and psychosomatic disorder(82.0±27.3)38). In comparison, the average SRI score for subjects in our study was 39.9(SD 20.5), which is very low. The exception was 1 out of the 18 participants, who received a score of 87.
Therefore, definition of the word “high stress subjects” did not equate with the clinical level of abnormal status.
Generally, well-executed acupuncture stimulation induces
“deqi” sensation for therapeutic effect39,40). “Deqi” is one of the most important factors of acupuncture, and because of this, it is recommended that clinical research document deqi sensation41). However, many studies that use of sham or minimal acupuncture as the control exclude deqi sensation.
Unfortunately, our findings showed that there was almost no difference in the deqi sensation experienced by the two groups. The lack of difference may be attributed to the fact that there was some needle stimulation in the SA groups (although the needle was blunt) or may be due to the weak stimulation of acupuncture in the RA group. In our study, both groups showed low pain according to the VAS, thus the latter has a large potential to explain the results. Other types of acupuncture sensation, for example sharp pain and deqi sensation stimulate the brain in different ways42), as well as other types of acupuncture such as electroacupuncture or manual acupuncture does43). The HT7 acupuncture point’s anatomical position is known for the likelihood of inducing less deqi sensation compared with other points such as LI4 and ST36 which widely used in deqi studies. Although, Park et al.’s study40) included the acupuncture point HT7 among a number of acupuncture points on different meridians to develop the ASQ, but each sensation of each acupuncture point was mixed in the final output. Another study which compared the deqi sensation using HT7 and S16 showed that both have deqi sensation, that the brain responses were different for each44). Direction of further studies could be to compare and further elucidate deqi sensation for the different acupoints instead of grouping them together.
Several studies explored the relationship between EEG and HRV data: Sakai et al.’s study12) demonstrated a positive correlation between the γ, α, and θ bands of the EEG and total power(VLF+LF+HF) of HR and parasympathetic activity, and a negative correlation between the θ, α, β, and γ bands and sympathetic activity. Also, Streitberger et al.15) showed that θ and α1 of EEGs and HF and LF of HRV parameter are negatively correlated, and that these results were related with deqi sensation.
Hsu et al.13) measured the EEGs and HRV’s after stimu- lating an auricular acupuncture point(shinmun) at ear on the same name as HT7(shinmun) and several other scalp acu- puncture points were used, and found that the parasy- mpathetic nerves were activated while the sympathetic ner- ves were suppressed.
Our findings showed that acupuncture affects one’s au-
tonomic nervous system functions and brain activity in specific ways, and that participants’ EEG and HRV results are different in the RA and SA groups depending on their level of stress. But we were unable to show the precise rela- tionship or reason for EEG changes in the autonomic nervous function. To conclude the results precisely, further large scale and long-term research including detailed study design and statistical considering such as multiple correction with sta- tistical consideration are warranted.
In conclusion, our results indicated that acupuncture sti- mulation at HT7 induces changes in brain activation and the ANS. These patterns are different according to the parti- cipant’s stress level. Acupuncture is a means to control ba- lance of the human body, and therefore, treatment of symp- toms depends greatly on the individual patient’s physiology and condition. To elucidate and ensure the consistency of our results, further studies are still necessary.
Acknowledgements
This research was supported by Basic Science Research Program through the National Research Foundation of Korea(NRF) funded by the Ministry of Education, Science and Technology(No. 2005-0049404) and a grant of the Korean Health Technology R&D Project, Ministry of Health and Welfare, Republic of Korea(HI13C0540).
References
1. WHO. World Health Organization(WHO) International Stan- dard Terminologies on Traditional Medicine in the Western Pacific Region. Manila : WHO Regional Office for the Western Pacific. 2007.
2. Park J, Linde K, Manheimer E, Molsberger A, Sherman K, Smith C, et al. The status and future of acupuncture clinical research.
J Altern Complement Med. 2008 ; 14 : 871-81.
3. Cabioglu MT, Cetin BE. Acupuncture and immunomodulation.
Am J Chin Med. 2008 ; 36 : 25-36.
4. Lin JG, Chen WL. Acupuncture analgesia : a review of its mech- anisms of actions. Am J Chin Med. 2008 ; 36 : 635-45.
5. Ulett GA, Han S, Han JS. Electroacupuncture : mechanisms and clinical application. Biol Psychiatry. 1998 ; 44 : 129-38.
6. Langevin HM, Yandow JA. Relationship of acupuncture points and meridians to connective tissue planes. Anat Rec. 2002 ; 269 : 257-65.
7. Han JS. Acupuncture : neuropeptide release produced by elec- trical stimulation of different frequencies. Trends Neurosci.
2003 ; 26 : 17-22.
8. Hui KK, Liu J, Makris N, Gollub RL, Chen AJ, Moore CI et al.
Acupuncture modulates the limbic system and subcortical gray structures of the human brain : evidence from fMRI studies in normal subjects. Hum Brain Mapp. 2000 ; 9 : 13-25.
9. Kong J, Gollub RL, Rosman IS, Webb JM, Vangel MG, Kirsch I et al. Brain activity associated with expectancy-enhanced place- bo analgesia as measured by functional magnetic resonance imaging. J Neurosci. 2006 ; 26 : 381-8.
10. Bonnet MH, Arand DL. Impact of activity and arousal upon spectral EEG parameters. Physiol Behav. 2001 ; 74 : 291-8.
11. Yu X, Zhang J, Xie D, Wang J, Zhang C. Relationship between scalp potential and autonomic nervous activity during a mental arithmetic task. Auton Neurosci. 2009 ; 146 : 81-6.
12. Sakai S, Hori E, Umeno K, Kitabayashi N, Ono T, Nishijo H.
Specific acupuncture sensation correlates with EEGs and auto- nomic changes in human subjects. Auton Neurosci. 2007 ; 133 : 158-69.
13. Hsu CC, Weng CS, Sun MF, Shyu LY, Hu WC, Chang YH.
Evaluation of scalp and auricular acupuncture on EEG, HRV, and PRV. Am J Chin Med. 2007 ; 35 : 219-30.
14. Kim MS, Kim HD, Seo HD, Sawada K, Ishida M. The effect of acupuncture at PC-6 on the electroencephalogram and electrocardiogram. Am J Chin Med. 2008 ; 36 : 481-91.
15. Streitberger K, Steppan J, Maier C, Hill H, Backs J, Plaschke K.
Effects of verum acupuncture compared to placebo acu- puncture on quantitative EEG and heart rate variability in healthy volunteers. J Altern Complement Med. 2008 ; 14 : 505-13.
16. Chen AC, Liu FJ, Wang L, Arendt-Nielsen L. Mode and site of acupuncture modulation in the human brain : 3D (124-ch) EEG
power spectrum mapping and source imaging. Neuroimage.
2006 ; 29 : 1080-91.
17. Yin CS, Park HJ, Kim SY, Lee JM, Hong MS, Chung JH et al.
Electroencephalogram changes according to the subjective acupuncture sensation. Neurol Res. 32 Suppl 1 : 31-6.
18. Knardahl S, Elam M, Olausson B, Wallin BG. Sympathetic nerve activity after acupuncture in humans. Pain. 1998 ; 75 : 19-25.
19. Li Z, Wang C, Mak AF, Chow DH. Effects of acupuncture on heart rate variability in normal subjects under fatigue and non-fatigue state. Eur J Appl Physiol. 2005 ; 94 : 633-40.
20. Haker E, Egekvist H, Bjerring P. Effect of sensory stimulation (acupuncture) on sympathetic and parasympathetic activities in healthy subjects. J Auton Nerv Syst. 2000 ; 79 : 52-9.
21. Chae Y-B, Park H-J, Koo S-T, Lee H-J. Review on acupuncture and autonomic nervous system : Heart rate variability analysis in humans. Journal of Meridian & Acupoint. 2007 ; 24 : 25-36.
22. Lee S, Lee MS, Choi JY, Lee SW, Jeong SY, Ernst E. Acupuncture and heart rate variability : A systematic review. Auton Neurosci.
23. WHO. WHO standard acupuncture point locations in the Western Pacific Region. Manila : World Health Organization.
2008.
24. Kim Y, Park J, Lee H, Bang H, Park HJ. Content validity of an acu- puncture sensation questionnaire. J Altern Complement Med.
2008 ; 14 : 957-63.
25. Min SK, Jon D-I, Lee SH, Ahn CB, Yoo SK. Clinical validity of the domestic EEG and EP mapping system (Neuronics). Sleep Med Psychophysiol. 1997 ; 4 : 96-106.
26. Shinohara M. Decreasing heart rate and shortening of the arte- rial pulse propagation time by acupuncture in the spectral analyses. Masui. 1997 ; 46 : 213-21.
27. Chan J, Briscomb D, Waterhouse E, Cannaby AM. An uncon- trolled pilot study of HT7 for 'stress'. Acupunct Med. 2002 ; 20 : 74-7.
28. Lin JG, Ho SJ, Lin JC. Effect of acupuncture on cardiopulmonary function. Chin Med J (Engl). 1996 ; 109 : 482-5.
29. Nordio M, Romanelli F. Efficacy of wrists overnight com- pression (HT 7 point) on insomniacs : possible role of melato- nin? Minerva Med. 2008 ; 99 : 539-47.
30. Lim S, Ryu YH, Kim ST, Hong MS, Park HJ. Acupuncture in- creases neuropeptide Y expression in hippocampus of mater-
nally-separated rats. Neurosci Lett. 2003 ; 343 : 49-52.
31. Park HJ, Lim S, Lee HS, Lee HJ, Yoo YM, Kim SA et al.
Acupuncture enhances cell proliferation in dentate gyrus of maternally-separated rats. Neurosci Lett. 2002 ; 319 : 153-6.
32. Chae Y, Yeom M, Han JH, Park HJ, Hahm DH, Shim I et al. Effect of acupuncture on anxiety-like behavior during nicotine with- drawal and relevant mechanisms. Neurosci Lett. 2008 ; 430 : 98-102.
33. Kim DH, Yang DH, Kim EJ, Nam DW, Park YC, Park YJ et al. A Study on the Effect of Interaction between Acupuncture at Shinmun (HT7) and Subject`s Cold or Heat Tendency on Heart Rate Variability. Journal of Korean Acupuncture and Moxibu- stion. 2006 ; 23 : 25-38.
34. Kim DH, Kim JD, Jung. KE, Kim KT, Rhu SR, Jung JC et al. A Study on the Effect of Moxibustion at Shinmun(H7) according to Cold or Heat Tendency. Journal of Korean Acupuncture and Moxibustion. 2004 ; 21 : 135-47.
35. de Kloet ER, Joels M, Holsboer F. Stress and the brain : from adaptation to disease. Nat Rev Neurosci. 2005 ; 6 : 463-75.
36. Dishman RK, Nakamura Y, Garcia ME, Thompson RW, Dunn AL, Blair SN. Heart rate variability, trait anxiety, and perceived stress among physically fit men and women. Int J Psycho- physiol. 2000 ; 37 : 121-33.
37. Annie CL, Groer M. Childbirth stress. An immunologic study. J Obstet Gynecol Neonatal Nurs. 1991 ; 20 : 391-7.
38. Koh KB, Park JK, Kim CH, Cho S. Development of the stress re- sponse inventory and its application in clinical practice.
Psychosom Med. 2001 ; 63 : 668-78.
39. Kong J, Gollub R, Huang T, Polich G, Napadow V, Hui K et al.
Acupuncture de qi, from qualitative history to quantitative measurement. J Altern Complement Med. 2007 ; 13 : 1059-70.
40. Park H, Park J, Lee H. Does Deqi (needle sensation) exist? Am J Chin Med. 2002 ; 30 : 45-50.
41. MacPherson H, White A, Cummings M, Jobst K, Rose K, Niemtzow R. Standards for reporting interventions in con- trolled trials of acupuncture : the STRICTA recommendations.
Complement Ther Med. 2001 ; 9 : 246-9.
42. Hui KK, Liu J, Marina O, Napadow V, Haselgrove C, Kwong KK et al. The integrated response of the human cerebro-cerebellar and limbic systems to acupuncture stimulation at ST 36 as evi- denced by fMRI. Neuroimage. 2005 ; 27 : 479-96.
43. Napadow V, Makris N, Liu J, Kettner NW, Kwong KK, Hui KK.
Effects of electroacupuncture versus manual acupuncture on the human brain as measured by fMRI. Hum Brain Mapp. 2005
; 24 : 193-205.
44. Chen SJ, Liu B, Fu WB, Wu SS, Chen J, Ran PC. [A fMRI ob- servation on different cererbral regions activated by acu- puncture of Shenmen (HT 7) and Yanglao (SI 6)]. Zhen Ci Yan Jiu.
2008 ; 33 : 267-71.
국문초록
목적 : 본 무작위배정 플라시보 대조군 교차연구는 신문혈의 침 치료가 뇌 활성도와 자율신경계에 어떠한 영향을 미치는지 뇌파(EEG)와 심박
변이도(HRV)를 통해 알아보고자 한 연구이다. 방법 : 18명의 건강인 피험자가 참여하여 1-3일의 간격을 두고 무작위배정 순서에 따라 신문혈
에 진짜침과 가짜침으로 시술받았고, 치료 전, 후에 각각 뇌파와 심박변이도를 측정하였다. 피험자의 스트레스 정도에 따른 반응의 차이를 살
펴보기 위하여 스트레스설문지를 이용하여 서브그룹분석을 시행하였다. 결과 : 그 결과, 침 치시술은 뇌파 중 α밴드 값의 증가를 나타냈으며,
진짜침 그룹의 경우 심박변이도의 결과값 중 HF와 RMS-SD의 증가가 대조군에 비해 유의하게 높았다. 스트레스 정도에 따른 서브그룹 분석에 서는 진짜침 그룹 중 스트레스 정도가 높은 피험자는 α밴드 값이 증가한 반면, 스트레스 정도가 낮은 피험자는 감소하거나 증가의 폭이 낮은
것을 알 수 있었으며, 거짓침 그룹에서는 비교적 적은 변화를 나타내었다. 결론 : 본 연구 결과를 통해 침이 뇌 활성도 및 자율신경계에 영향을
미치며, 이는 부교감신경계통과 관련이 있음을 알 수 있었다. 또한 이러한 결과는 환자의 스트레스 정도에 따라 다른 반응을 나타냄을 보여주 었다.