INTRODUCTION
The first repair of superior labrum anterior posterior (SLAP) lesion was performed by Andrews and Gidumal [1]
using arthroscopic debridement. This type of labral injury was thought to be a deceleration injury that occurs in the followthrough phase of a throwing motion. It was found that traction and overloading of the long head of biceps tendon was the cause of the tear. The term, SLAP lesion, was initially given by Snyder et al. [2], who also classified the lesions into four classes; type I, II, III, and IV. Later, the classification system brought up to five classes, with an additional type X class, by Maffet et al. [3] and Powell et al. [4]. At the time, a positive correlation between SLAP lesions and overhead athletes were not made [5]. Type II SLAP is the most commonly occurring class in overhead
athletes, in which mobility of shoulder joints is impaired and pain is induced [6].
ANATOMY
Glenoid labrum is composed of fibrocartilage and primarily surrounds the glenohumeral joint. The glenoid labrum allows the glenoid fossa to be extended deeply, thereby limiting the translation of the humeral head. This structural feature enhances the concavitycompression mechanism of the labrum. Part of this mechanism is the long head biceps complex, where the superior glenoid labrum acts as the root. Unlike the inferior glenoid labrum that is sturdily attached to the glenoid, around 60% is flexibly attached, giving an appearance of a ‘meniscuslike labrum’ [7]. The precise mechanistic role of the long head Superior labrum anterior posterior lesion is a major cause of shoulder pain and dysfunction in throwing athletes.
Several theories explain the possible pathogenesis of superior labrum anterior posterior lesions. The current modalities of clinical examination that diagnose lesions of superior labrumbiceps tendon complex have a high selectivity but a low specificity, which limits their usefulness. Thus, magnetic resonance arthrography is needed to diagnose lesions of superior labrumbiceps tendon complex and to rule out normal variants. A combined physical examination and radiologic evaluation is important to identify symptomatic lesions. Repair of superior labrum anterior posterior tears in throwing athletes should take into account the biomechanics of the superior labrumbiceps tendon complex as well as concepts of kinetic chain, in case of symptomatic lesions. When an operative treatment is considered for throwing athletes, especially of elite baseball players, surgeons should inform patients of the low rate of return to preinjury level after the superior labrum anterior posterior repair.
Keywords: Glenoid labrum; Superior labrum anterior posterior; Throwing athletes; Scapular dyskinesis; Shoulder
Current concepts of type II superior labrum anterior posterior lesion management in throwing athletes
Jin-Young Park
1, Jin-Young Bang
21Department of Orthopaedic Surgery, Shoulder, Elbow Joint Center, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul; 2Department of Orthopaedic Surgery, Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea
Copyright © 2014 Korean Arthroscopy Society and Korean Orthopedic Society for Sports Medicine. All rights reserved.
CC This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/3.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received January 9, 2014; Revised March 10, 2014; Accepted March 21, 2014
Correspondence to: Jin-Young Bang, Department of Orthopaedic Surgery, Haeundae Paik Hospital, Inje University College of Medicine, 875 Haeun-daero, Haeundae-gu, Busan 612-896, Korea. Tel: +82-51-2030-7793, Fax: +82-51-797-0991, E-mail: allthatineed@
hanmail.net Arthroscopy and
Orthopedic Sports Medicine
AOSM
biceps tendonsuperior glenoid labrum complex is not yet known, but it has been implicated in the stability of the body below the shoulders during any elevation exercise.
Further, the long head biceps tendon has been shown to increase the resistance against the torsion force of the shoulders upon abduction and external rotation (ABER) thereby maintaining the anterior stability of glenohumeral joints and preventing superior migration of the humeral head.
PATHOPHYSIOLOGY
Overhead throwing is essentially a repetition of hyper
abduction and external rotation resulting in excessive stress on the shoulder joint by persistently exerting of shearing and compression forces on the glenohumeral joint, rotator cuff, and capsulolabral complex [8]. Here we introduce possible theories of the pathogenesis of superior labral tears in throwing athletes.
Internal impingement
Walch et al. [9] described an intraarticular impingement that occurred during an abducted external rotated position of the thrower’s arm as an internal impingement.
In an internal impingement, the undersurface of the posterosuperior rotator cuff is in contact with posterosuperior glenoid labrum and is squeezed between the labrum and the greater tuberosity, at abduction 90o-external rotation 90o position. Jobe [10] showed this phenomenon in throwing athletes and not only that this occurred in rotator cuff, but also in the glenoid labrum and the bone. Furthermore, repetitive stretching can lead to combined anterior microinstability and an exacerbated internal impingement, where reconstruction of the anterior capsulolabral may be required. However, some authors have suggested that an internal impingement is simply a rare natural occurrence [11].
Glenohumeral internal rotation deficit and posterior capsular tightness
Wilk et al. [12] found that shoulder injuries occur more often in throwers with concomitant glenohumeral internal rotation deficit (GIRD). The authors found that throwers with GIRD were twice as more likely to endure shoulder injuries than those without GIRD. Furthermore, the authors found that although a maximal hyperexternal rotation helps acceleration of a throwing ball during a late cocking phase, the changes in shoulder motion arc
can lead to damage in the labrum, long head of biceps tendon, and the rotator cuffs. A viscous cycle forms when posterior capsular tightness, induced by the shoulder damage aggravates GIRD.
Peel back mechanism
Burkhart and Morgan [13] proposed a “peel back” mec
ha nism. When the humeral head translates into the posterosuperior position, the cam effect decreases, which in turn causes the anterosuperior capsular structure to become lax. When the arm extends into an abduction and hyperexternal rotation position, torsional force on the biceps and labrum induces the biceps from a horizontal to a more vertical position. Such changes cause a twist in the base of the biceps, and the energy is transmitted to the posterosuperior labrum ultimately leading to a
“peel back”. Although a peel back mechanism is a normal activity of the superior labrum, if associated excessively with SLAP may lead to symptoms of tear.
Kinetic chain
A throwing action is an amalgamation of energy from a series of events that begin from the lower and translate to the upper extremity [14]. Greiwe and Ahmad [8] called this movement of energy from the lower extremity, waist, scapular, shoulder, to the arm as a “kinetic chain”.
Further, they found that muscle imbalance, especially of the scapular region, within this kinetic chain, is a major cause of shoulder impingement, rotator cuff tears, and instability. Jobe and Pink [15] reported that kinetic chain abnormality occurs when hyperabduction and external rotation is out of its normal range.
Scapular malposition, inferiormedial border prominence, coracoids pain and malposition, and dyskinesis of scapular movement
Scapular malposition, inferiormedial border prominence, coracoids pain and malposition, and dyskinesis of scapular movement (SICK) is an extension of the kinetic chain. Changes in scapular mechanics lead to abnormal shoulder kinematics, thereby leading to shoulder pain and dysfunction. Scapular movement allows integrity of the glenohumeral articulation and maintains rotator cuff musculature [16]. These intrinsic muscle activity supports glenohumeral stability through a concavity
compression mechanism. Scapular composes of an important part of the kinetic chain in a throwing shoulder.
A malpositioned scapular impairs shoulder function, and
this impairment is called “scapularthoracic dyskinesis”. A reduced scapular retraction during cocking phase or an excessive scapular protraction during acceleration phase lead to a defect in concavitycompression, and thereby scapular impingement through either a downward or a forward scapular rotation [16]. Burkhart et al. [17] applied the term SICK to a disabled throwing shoulder. Of in
terest, they described a SICK scapular, with a deficit in internal rotation, in patients where repetitive throwing motions had led to increased torsional load on the inferior glenohumeral ligament and increased strain on the posterosuperior rotator cuff during late cocking phase, ultimately aggravating an internal impingement and peel back mechanism [17].
PHYSICAL EXAMINATION
Clinically evaluating SLAP lesion has shown to be in
effective, as subsequent radiological examinations have confirmed many false positive results diagnosed by clinical examination, and no physical examination that specifically diagnoses SLAP lesions exist. Typical symptoms of SLAP lesion in throwing athletes is a gradual loss in athletic performance and throwing speed.
Mechanical symptoms such as clicking during late cocking phase are also possible [18]. Further, in cases where partialthickness rotator cuff tear of the articular surface, capsulobabral injury, biceps tendinitis, and internal impingement occur together, these symptoms may come associated with nocturnal pain and instability [19]. Physical examination of the shoulder joints in these throwing athletes should be made from the glenohumeral joint to the scapulothoracic motion. First, range of motion and muscle strength should be assessed, especially at 90o abduction. Further, external and internal rotation should be measured and compared to the contralateral side. Reinold et al. [20] suggested that a possible patho
physiology of SLAP lesions is the decrease in internal rotation which leads to an eccentric force that gradually promotes the development of the external rotators (infraspinatus and teres minor). This development of the external rotators contribute to the eccentric contracture of the posterior glenohumeral muscles and cause muscular microinjury and acute decrease in angular kinematics.
Tests on stability should also be made. Tests to indicate anterior capsulolabral injury are load shift test and apprehension relocation test, whereas tests to indicate inferior instability and posterior instability are the sulcus
test and jerk test, respectively [21].
A range of tests can detect superior labral injury, such as Crank test, active compression test, biceps load test I, II, pain provocation test, resisted supination external rotation test, compression rotation test, and forced abduction test [22]. Most of these tests are known to have a high sensitivity for SLAP lesions, but have low specificity. A metaanalysis by Meserve et al. [23] evaluated the relative sensitivity and specificity of these tests and showed that that active compression test, crank test, and Speed test had in order of the most to the least diagnostic accuracy.
Conversely, Cook et al. [24] looked at the diagnostic accuracy of O’Brien active compression test, Speed test, biceps load II test, O’Driscoll, dynamic labral shear test, and the labral tension test and found that multiple diagnoses using multiple tests over a single diagnosis increases the diagnostic power. A systematic review by Jones and Galluch [25] has also usefully summarized the selectivity/specificity of the various diagnostic tests.
Scapular dyskinesis can induce SLAP lesions and thus it is important to assess scapular motion. To assess scapular motion, asymmetry between the dominant and the nondominant shoulder is marked during forward elevation. If scapular depression, anterior tilting, and/or protraction exist, a presence of a lesion in the throwing shoulder that shows pain should be considered. To assess scapular dyskinesis, the scapular assistance test (SAT) and the scapular retraction test (SRT) are used. During SAT, the patient stabilized the upper scapular with his/her hands, then, the inferiomedial border is rotated to assist an upward rotation movement of the scapular. During this movement, if impingement, clicking, or weakness in the rotator cuff is felt, scapular dyskinesis should be diagnosed. During SRT, the patient stabilizes the scapular medial border by with his/her hands, then, the arm is elevated and similar nature of discomfort is noted for as the SAT [26].
IMAGE
AP, stryker notch, axillary view radiographs are helpful. The posterior and posteroinferior glenoid can be examined by stryker and/or axillary views. Bennett lesions, glenoid erosion, outlet impingement, and acromioclavicular joint lesions can also be seen. Detecting SLAP lesions by radiographical means such as magnetic resonance imaging is known to be accurate, and of them, magnetic resonance arthrogrhaphy (MRA) has proved to be most
effective. Normal variation should not be mistaken for lesions.
TREATMENT
When considering the choice of treatment for athletes, it is important to consult not only the athletes themselves but also their family, team coach etc., as a successful return to sports is a major issue for these patients. Therefore, a direct and accurate conveyance of the prognostic outlook and period of rehabilitation for these athletes is of high priority [27].
Nonsurgical treatment
Shoulder injuries in throwing athletes can occur from alteration in the kinetic chain that is comprised of the hip, trunk, scapulothoracic complex, and posterior capsule. For example, a change in scapulothoracic position increases degree of fatigue, which may cause internal impingement or weaken the rotator cuff. As such, nonsurgical treatment concentrates on strengthening of the rotator cuffs, improving scapular motion through periscapular exercise, and posterior capsule stretching etc [17,22].
Surgical treatment
Surgical treatment is employed for symptomatic SLAP lesions and for patients unresponsive to nonsurgical treatment. Fixation methods of treatment include transosseous suture, screws, staples, and bioabsorbable suture. The use of metallic anchors during fixation methods have largely been replaced by bioabsorbable suture anchors as it lessens complications of implant loosening, migration, and chondral injury. However, despite the safety and efficacy of bioabsorbable anchors, implant breakageinduced failure and premature degradation is seen when these anchors are used [28].
Anchorrelated complication cause pain and stiffness in patients, and if the patients shows an unexpected out come or delay in recovery of surgery, a possible anchorrelated complication should be ruled out. Glenohumeral synovitis, glenoid osteolysis, loose bodies, and chondral injuries are complications that have been reported so far. In an attempt to decrease complications, polyetheretherketone (PEEK) and other composites has been included as a composition of bioabsorbable anchors in place of polyglycolic acid (PGA) and polyLlactic Acid (PLLA), the novel bio
absorbable anchors have shown promising outcomes [29].
Not only are the arthroscopic portals, anterosuperior and anterorinferior portals, used to treat SLAP lesions, the transrotator cuff portal approach has also been used. However, the gold standard configuration for SLAP repair is yet under dispute. A few examples of configurations used in SLAP repair are; 1) repair after inserting two anchors anterior and posterior relative to the biceps tendon insertion, 2) horizontal mattress suture after inserting an anchor at the biceps tendon insertion, and 3) repair after insertion of at least one anchor at the posterior biceps tendon to neutralize the torsional peel back mechanism (Figs. 1, 2). Another configuration suggested when repairing SLAP in overhead athletes is to insert the anchor anterior to the biceps root as opposed to the posterior side. This is because positioning the anchor at the posterior side of the biceps may lead to tethering of the biceps, which would limit the postoperative range of motion (especially the external rotation) [27].
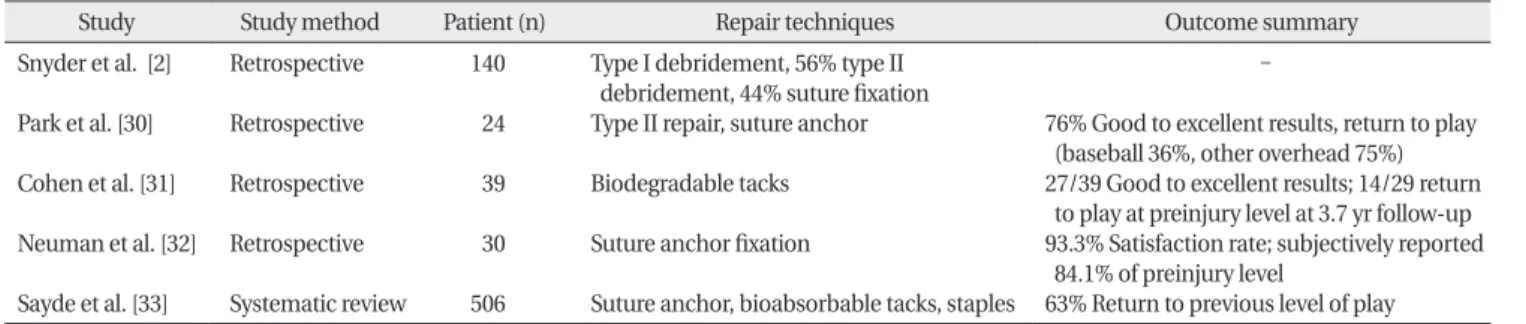
OUTCOMES
Several studies report the clinical outcomes of SLAP lesion repair (Table 1) [2,3033]. Surgical intervention of type II SLAP lesions show in general a positive outcome in normal patients (40%-94%), but this is by no means to say that elite athletes with type II SLAP lesions can return to sports with the same shoulder joint condition as before [30,34-37]. In addition, the rate of return to sports after repair differs between the kind of sports that athlete plays.
Park et al. [30] found a 38% rate of return to sports after arthroscopic repair of type II SLAP lesions in 24 overhead baseball athletes at 45.8 month followup, whereas the rate of return to sports was 76% for athletes of all other sports. Brockmeier et al. [38] found a similar result where the rate of return to sports in baseball athletes (64%) was lower than that of overhead athletes of other sports (76%) after SLAP lesion repair. Cohen et al. [31] used bio
absorbable tack on 39 type II SLAP lesion patients, and of these, only 14 (48%) could return to sports at the level of preinjury, and only 3 of the 8 throwers could return to sports at all (Table 1). On the other hand, if SLAP lesions came in combination with another lesion, such as a rotator cuff tear, in the middle aged group the SLAP underperformed after repair, opposed to when the lesion was isolated, when there was no glenohumeral arthritis, or when the patient was highly active [39].
Fig. 1. (A) Arthroscopic view of a type 2 superior labralanterior to posterior (SLAP) tear from the posterior portal. (B) Superior glenoid after preparation. (C) Suture passing procedure using a shuttle relay technique. (D) SLAP lesion repaired with suture anchors.
Fig. 2. (A) Arthroscopic view of a type 2 superior labral anterior to posterior (SLAP) tear from the posterior portal.
(B) Excessive peel back phenomenon in abduction and external rotation (ABER).
(C) View after SLAP repair. (D) It is not observed peel back phenomenon in ABER position after SLAP repair using horizontal matress suture.
CONCLUSION
Repetitive posture in overhead athlete can lead to micro
damage and lesion of the bicepssuperior labrum complex.
Resulting GIRD, internal impingement, posterior capsular tightness, and scapular dyskinesis may be the cause of pain in patients with SLAP lesions. These symptoms prevent proper functioning of the rotator cuff and agg
ravate dynamic microinstability, decreasing the athletic performance of the patient. GIRD and scapular dyskinesis may be managed by nonsurgical treatment. If nonsurgical treatment is ineffective, surgical treatment is considered taking into account the patient’s age and level of activity.
Further, a low rate of return to sports for professional athletes, especially for baseball players, therefore, discussing the prognostic factors with the patients and the concerned team is an important process prior to any intervention. Lastly, a better understanding of the precise pathogenesis of SLAP lesions that correlate with symptoms, physical examination and imaging results is required to effectively diagnose them.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
1. Andrews JR, Gidumal RH. Shoulder arthroscopy in the throwing athlete: perspectives and prognosis. Clin Sports Med 1987;6:
565-71.
2. Snyder SJ, Karzel RP, Del Pizzo W, Ferkel RD, Friedman MJ. SLAP lesions of the shoulder. Arthroscopy 1990;6:274-9.
3. Maffet MW, Gartsman GM, Moseley B. Superior labrum-biceps tendon complex lesions of the shoulder. Am J Sports Med 1995;23:93-8.
4. Powell SE, Nord KD, Ryu RKN. The diagnosis, classification, and treatment of SLAP lesions. Op Tech Sports Med 2004;12:99- 110.
5. Burkhart SS, Morgan C. SLAP lesions in the overhead athlete.
Orthop Clin North Am 2001;32:431-41, viii.
6. Cho HL, Lee CK, Hwang TH, Suh KT, Park JW. Arthroscopic repair of combined Bankart and SLAP lesions: operative techniques and clinical results. Clin Orthop Surg 2010;2:39-46.
7. Cooper DE, Arnoczky SP, O’Brien SJ, Warren RF, DiCarlo E, Allen AA. Anatomy, histology, and vascularity of the glenoid labrum. An anatomical study. J Bone Joint Surg Am 1992;74:46-52.
8. Greiwe RM, Ahmad CS. Management of the throwing shoulder:
cuff, labrum and internal impingement. Orthop Clin North Am 2010;41:309-23.
9. Walch G, Boileau P, Noel E, Donell ST. Impingement of the deep
surface of the supraspinatus tendon on the posterosuperior glenoid rim: an arthroscopic study. J Shoulder Elbow Surg 1992;
1:238-45.
10. Jobe CM. Posterior superior glenoid impingement: expanded spectrum. Arthroscopy 1995;11:530-6.
11. Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology part I: pathoanatomy and biomechanics. Arthroscopy 2003;19:404-20.
12. Wilk KE, Macrina LC, Fleisig GS, et al. Correlation of glenohu- meral internal rotation deficit and total rotational motion to shoulder injuries in professional baseball pitchers. Am J Sports Med 2011;39:329-35.
13. Burkhart SS, Morgan CD. The peel-back mechanism: its role in producing and extending posterior type II SLAP lesions and its effect on SLAP repair rehabilitation. Arthroscopy 1998;14:637- 40.
14. Kibler WB. The role of the scapula in athletic shoulder function.
Am J Sports Med 1998;26:325-37.
15. Jobe FW, Pink MM. Operative techniques in upper extremity sports injuries. St. Louis, MO: Mosby; 1996.
16. Kibler WB. Scapular involvement in impingement: signs and symptoms. Instr Course Lect 2006;55:35-43.
17. Burkhart SS, Morgan CD, Kibler WB. The disabled throwing
REFERENCES
Table 1. Outcomes after SLAP repair
Study Study method Patient (n) Repair techniques Outcome summary
Snyder et al. [2]
Park et al. [30]
Cohen et al. [31]
Neuman et al. [32]
Sayde et al. [33]
Retrospective Retrospective Retrospective Retrospective Systematic review
140 24 39 30 506
Type I debridement, 56% type II debridement, 44% suture fixation Type II repair, suture anchor Biodegradable tacks Suture anchor fixation
Suture anchor, bioabsorbable tacks, staples
-
76% Good to excellent results, return to play (baseball 36%, other overhead 75%) 27/39 Good to excellent results; 14/29 return to play at preinjury level at 3.7 yr followup 93.3% Satisfaction rate; subjectively reported 84.1% of preinjury level
63% Return to previous level of play SLAP, superior labrum anterior posterior.
shoulder: spectrum of pathology part III: the SICK scapula, scapular dyskinesis, the kinetic chain, and rehabilitation.
Arthroscopy 2003;19:641-61.
18. Reinold MM, Gill TJ. Current concepts in the evaluation and treatment of the shoulder in overhead-throwing athletes, part 1:
physical characteristics and clinical examination. Sports Health 2010;2:39-50.
19. Powers R. SLAP lesions: how to recognize and treat this debili- tating shoulder injury. JAAPA 2011;24:32, 5-6, 8 passim.
20. Reinold MM, Wilk KE, Macrina LC, et al. Changes in shoulder and elbow passive range of motion after pitching in professional baseball players. Am J Sports Med 2008;36:523-7.
21. Kemp K, Sheps DM. Clinical tests to identify SLAP lesions: a meta-analysis. Clin J Sport Med 2009;19:339-40.
22. Knesek M, Skendzel JG, Dines JS, Altchek DW, Allen AA, Bedi A.
Diagnosis and management of superior labral anterior posterior tears in throwing athletes. Am J Sports Med 2013;41:444-60.
23. Meserve BB, Cleland JA, Boucher TR. A meta-analysis examining clinical test utility for assessing superior labral anterior posterior lesions. Am J Sports Med 2009;37:2252-8.
24. Cook C, Beaty S, Kissenberth MJ, Siffri P, Pill SG, Hawkins RJ.
Diagnostic accuracy of five orthopedic clinical tests for diagnosis of superior labrum anterior posterior (SLAP) lesions. J Shoulder Elbow Surg 2012;21:13-22.
25. Jones GL, Galluch DB. Clinical assessment of superior glenoid labral lesions: a systematic review. Clin Orthop Relat Res.
2007;455:45-51.
26. Park JY, Lhee SH, Oh JH, Kim HK. Scapular dyskinesis. J Korean Shoulder Elbow Soc 2009;12:271-7.
27. Lintner DM. Superior labrum anterior to posterior tears in throwing athletes. Instr Course Lect 2013;62:491-500.
28. Dhawan A, Ghodadra N, Karas V, Salata MJ, Cole BJ. Compli- cations of bioabsorbable suture anchors in the shoulder. Am J Sports Med 2012;40:1424-30.
29. Nho SJ, Provencher MT, Seroyer ST, Romeo AA. Bioabsorbable
anchors in glenohumeral shoulder surgery. Arthroscopy 2009;25:788-93.
30. Park JY, Chung SW, Jeon SH, Lee JG, Oh KS. Clinical and radiolo- gical outcomes of type 2 superior labral anterior posterior repairs in elite overhead athletes. Am J Sports Med 2013;41:1372-9.
31. Cohen DB, Coleman S, Drakos MC, et al. Outcomes of isolated type II SLAP lesions treated with arthroscopic fixation using a bioabsorbable tack. Arthroscopy 2006;22:136-42.
32. Neuman BJ, Boisvert CB, Reiter B, Lawson K, Ciccotti MG, Cohen SB. Results of arthroscopic repair of type II superior labral anterior posterior lesions in overhead athletes: assessment of return to preinjury playing level and satisfaction. Am J Sports Med 2011;39:1883-8.
33. Sayde WM, Cohen SB, Ciccotti MG, Dodson CC. Return to play after type II superior labral anterior-posterior lesion repairs in athletes: a systematic review. Clin Orthop Relat Res 2012;470:1595-600.
34. Denard PJ, Lädermann A, Burkhart SS. Long-term outcome after arthroscopic repair of type II SLAP lesions: results according to age and workers’ compensation status. Arthroscopy 2012;28:
451-7.
35. Gorantla K, Gill C, Wright RW. The outcome of type II SLAP repair:
a systematic review. Arthroscopy 2010;26:537-45.
36. Katz LM, Hsu S, Miller SL, et al. Poor outcomes after SLAP repair:
descriptive analysis and prognosis. Arthroscopy 2009;25:849- 55.
37. Oh JH, Lee HK, Kim JY, Kim SH, Gong HS. Clinical and radiologic outcomes of arthroscopic glenoid labrum repair with the Bio- Knotless suture anchor. Am J Sports Med 2009;37:2340-8.
38. Brockmeier SF, Voos JE, Williams RJ 3rd, et al. Outcomes after arthroscopic repair of type-II SLAP lesions. J Bone Joint Surg Am 2009;91:1595-603.
39. Oh JH, Kim SH, Kwak SH, Oh CH, Gong HS. Results of concomitant rotator cuff and SLAP repair are not affected by unhealed SLAP lesion. J Shoulder Elbow Surg 2011;20:138-45.