Korean J Fam Pract. 2013;3:77-80
Vol. 3, No. 1 Mar 2013
| 77
가정의학
말기 암 환자에서 항암치료 종료 후 호스피스 입실까지의 기간이 여명에 미치는 영향
Brief Communication
이정욱, 반가형, 최환석, 이용주
1, 라정란
2, 박명희
2, 성지민
2, 김철민*
가톨릭대학교 의과대학 가정의학교실, 1가톨릭대학교 서울성모병원 완화의학과, 2가톨릭대학교 서울성모병원 간호부
The Effect of a Period of Hospice Admission after Quitting Chemotherapy on the Duration of Life for Terminal Cancer Patients
Jung-Wook Lee, Ga-Hyung Ban, Hwan-Seok Choi, Yong-Joo Lee
1, Jeong-Lan Ra
2, Myung-Hee Park
2, Ji-Min Seong
2, Cheol-Min Kim*
Department of Family Medicine, The Catholic University College of Medicine; 1Department of Hospice, Seoul St. Mary’s Hospital, The Catholic University College of Medicine; 2Department of Nursing, Seoul St. Mary’s Hospital, The Catholic University of Korea College of Nursing, Seoul, Korea
Background: Recently, there has been a rising interest in hospice therapy for terminal cancer patients for improving their quality of life, and managing their pain and symptoms. The aim of this study is to verify the correlation between the timing of the hospice consultation and the duration of life of the patients.
Methods: We investigated 155 patients’ medical records retrospectively who had died from January 2011 to December 2011 after they had been treated at the hospice center in the Catholic Medical Center. We investigated the last date of chemotherapy, the admission date at the hospice center, and the date of death of the patients. With these dates, we calculated the period between the date of quitting chemotherapy and the admission date at the hospice center, and between the fi rst day of hospice care and the date of death.
Results: The median duration of life of group 1 (less than 15 days between the date of quitting chemotherapy and the admission date at the hospice center), 26 months, was longer than that of group 2 (more than 15 days between the date of quitting chemotherapy and the admission date at the hospice center), which was 10 months (P=0.035).
Conclusion: This study showed that rapid admission to hospice care had a positive impact on the duration of life of terminal cancer patients.
Keywords: Hospice; Cancer Terminal Stage; Survival Rate; Chemotherapy
서론
최근 말기 암 환자에 있어서의 높은 질의 삶 및 통증, 증상 조절의 중요성에 대해서 관심이 높아지고 있다.1-3) 호스피스 완화의료는 말기 암 환자의 총체적인 돌봄(holistic care)이며, 환자의 증상조절 및 정신적 지지를 통해 삶의 질을 높이며 무 의미한 의료서비스의 사용을 줄이는 방향으로 환자를 이끈 다.4,5) 호스피스완화의료의 대상자는 임종이 6개월 이내로 예 Received: August 29, 2012, Accepted: March 4, 2013
*Corresponding Author: Cheol-Min Kim
Tel: 02-2258-1914, Fax: 02-2258-1916 E-mail: [email protected]
Korean Journal of Family Practice
Copyright © 2013 by The Korean Academy of Family Medicine
Jung-Wook Lee, et al: Effect of Survival Rate: Perioid from Last Chemotherapy to Hospice Care
78 |
Vol. 3, No. 1 Mar 2013 Korean J Fam Pract견되는 환자이나 전통적으로 질병 경과상 늦은 시기에 타과 로부터 의뢰되어왔다.6,7) 의미 있는 완화의료를 위해서는 질병 경과상 이른 시기에 제공돼야 하며 이른 완화의료 치료를 받 은 경우 기존 항암치료를 받은 경우보다 삶의 질, 우울증상에 나은 결과를 가져왔다.8) 그러므로 적절한 시기의 호스피스 의 뢰는 말기 암 환자의 삶의 질에 지대한 영향을 미칠 것으로 생 각된다. 이번 연구에서는 암 환자의 주치의가 치료를 위한 마 지막 항암요법을 마친 후에, 호스피스완화의료에 자신의 환 자를 의뢰하는 시점과 환자가 의뢰된 이후 호스피스 입실까 지의 기간, 호스피스 입실부터 사망에 이르는 기간과의 상관 관계를 알아봄으로써 말기 암 환자에 대한 주치의의 호스피 스 인식도 제고에 필요한 정보를 제공할 것으로 생각한다.
방법
1. 연구대상 및 기간
서울성모병원 호스피스센터에서 2011년 1월 1일부터 2011년 12월 31일 사이에 입원한 말기 암 환자 중 155명을 대상 으로 연구를 진행하였다.
2. 연구방법
후향적 조사연구이며 의무기록에서 인구통계학적, 임상 적 자료를 수집한 후 최종 항암제 투여일과 호스피스 병동 입 실일, 호스피스 병동 입실 이후 사망한 날짜를 통해 최종 항 암제 투여 후 입원까지의 기간 및 입원 후 사망까지의 기간 을 산출하였다. 대상 환자의 통증점수는 지난 24시간 동안의 통증을 통증자(ruler)를 이용하여 0에서 10까지 점수를 측정 하는 Numeric rating scale (NRS)를 사용하였으며 기능상태는 Anderson에 의해 1996년 처음 개발된 완화수행지수인 palliative performance scale을 이용하였다.9)
3. 통계분석
Mann-Whitney U-test, Fisher’s exact test를 이용하였으며 두 방법 모두 multivariate analysis는 적용하지 않았다.
결과
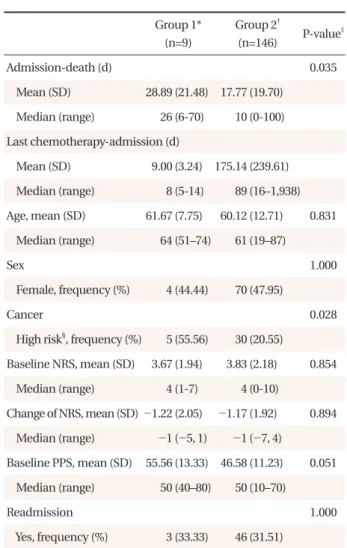
연구대상 환자 155명 중 최종 group 1(최종 항암제 투여 후 입원까지 15일 이하)은 9명(5.8%), group 2(최종 항암제 투 여 후 입원까지 15일 초과)는 146명(94.2%)이었다. 두 그룹에 서 연령, 성별, palliative performance scale 그리고 numeric rating scale (NRS)는 통계적으로 유의한 차이가 없었으며 group 1에
서 고위험 암(간담췌, 식도)의 비율이 통계적으로 유의하게 더 높은 비율로 관찰되었다. Group 1과 group 2의 입원 후 사망 까지의 기간은 group 1에서 중간값 26일로 group 2의 10일에 비 해 생존기간이 유의하게 더 길게 나왔다(P=0.035) (Table 1).
고찰
본 연구의 결과 group 1(최종 항암제 투여 후 입원까지 15 일 이하)에서 입원 후 사망까지의 기간이 중간값 26일로 group 2(최종 항암제 투여 후 입원까지 15일 초과)의 10일에 비해 더 길게 측정되었다.
Table 1. General characteristics of the study subjects
Group 1*
(n=9)
Group 2†
(n=146) P-value‡
Admission-death (d) 0.035
Mean (SD) 28.89 (21.48) 17.77 (19.70) Median (range) 26 (6-70) 10 (0-100) Last chemotherapy-admission (d)
Mean (SD) 9.00 (3.24) 175.14 (239.61) Median (range) 8 (5-14) 89 (16–1,938) Age, mean (SD) 61.67 (7.75) 60.12 (12.71) 0.831 Median (range) 64 (51–74) 61 (19–87)
Sex 1.000
Female, frequency (%) 4 (44.44) 70 (47.95)
Cancer 0.028
High risk§, frequency (%) 5 (55.56) 30 (20.55)
Baseline NRS, mean (SD) 3.67 (1.94) 3.83 (2.18) 0.854 Median (range) 4 (1-7) 4 (0-10)
Change of NRS, mean (SD) -1.22 (2.05) -1.17 (1.92) 0.894 Median (range) -1 (-5, 1) -1 (-7, 4)
Baseline PPS, mean (SD) 55.56 (13.33) 46.58 (11.23) 0.051 Median (range) 50 (40–80) 50 (10–70)
Readmission 1.000
Yes, frequency (%) 3 (33.33) 46 (31.51) NRS: numeric rating scale, PPS: palliative performance scale.
*Less than or equal to 15 days between the date of quitting chemotherapy and the admission date of hospice center. †More than 15 days between the date of quitting chemotherapy and the admission date of hospice center. ‡Mann-Whitney U-test for continuos data, Fisher’s exact test for categorical data. §Hepatobiliary, pancreas, esophagus.
이정욱 외 : 항암종료후 호스피스 입실이 여명에 미치는 영향
Vol. 3, No. 1 Mar 2013
| 79
가정의학
이전 연구들에서 호스피스로의 늦은 의뢰가 암 환자에게 부적절한 의료의 질을 제공한다는 결과가 나왔듯이 말기 암 치료는 높은 삶의 질 유지를 위해 질병의 경과상 이른 시기에 완화의료, 호스피스에 의뢰돼야 한다.10) 본 연구는 호스피스 로의 이른 의뢰를 통해 환자가 효과적인 증상조절을 받게 됨 으로써 그들의 삶의 질을 증진시켜 전체적인 생존기간 또한 늘어날 수 있을 것이라는 가설을 가지고 진행하였으며 그 결 과 또한 group 1에서 group 2에 비해 더 긴 생존기간을 보여 가 설에 부합하였다.
이른 의뢰와 관련된 선행연구에서 새롭게 진단된 전이성 비소세포폐암 환자에서 완화의료를 종양치료와 함께 받았 을 경우와 종양치료만 받았을 경우로 나누어서 12주 후 삶의 질과 기분에 대해 재평가하였다. 그 결과 107명의 대상자 중 완화의료를 함께 받은 그룹에서 더 높은 삶의 질을 보였으며 더 적은 우울증상을 보였다. 또한 평균 생존기간의 경우 각각 11.6개월, 8.9개월로 생존기간도 연장되었음을 보였다.8)
이렇듯 말기 암 환자의 생존기간을 늘리기 위해서 이른 시 기에 호스피스로의 의뢰가 필요하다. 물론 호스피스로의 이 른 의뢰를 비롯하여 말기 암 환자의 여명에 영향을 주는 많은 요소들이 밝혀져 있으며 연구되고 있다. 일반적으로 암의 종 류, 암의 분화도, 환자의 기능상태, 연령 등은 암 환자의 여명에 영향을 줄 수 있는 요소이다.11,12) 본 연구는 후향적 연구라 제 한적이기는 하나 연령, 성별, 고위험 암, 기능지수를 보정한 후 에도 두 그룹 간에 유의한 차이를 보였다.
하지만 이런 호스피스로의 이른 의뢰를 위해서 극복해야 할 여러 과제들이 있다. 호스피스완화의료로의 늦은 의뢰는 환자, 가족, 의사, 의료시스템 등 여러 요인들과 관련이 있을 수
있다.13-15) 또한 우리나라의 환자들은 그들의 치료에 대한 결정
을 간혹 그들의 가족에게 위임하고 환자의 가족들은 환자에 게 모든 가능한 치료를 제공함으로써 희망을 유지하며, 그럼 으로써 그들의 의무를 다하는 것이라고 생각하기에 더 침습 적인 치료를 원하는 경향이 있다.16) 그리고 국내에서는 호스 피스완화의료에 대한 인식이 아직까지 매우 낮다. 말기 암 환 자를 치료하는 의사들이 호스피스완화의료를 더 나은 선택 으로서 잘 받아들이지 않는 경향이 있으며 말기 암 환자 중 오 직 9.1%의 환자만이 의뢰된다.17) 그러므로 호스피스완화의료 에 대한 인식도 제고를 위해 환자와 가족, 의사 모두 교육 및 홍 보가 필요한 상황이다. 특히 의뢰를 하는 주 역할은 의사이기
에,13,18) 교육을 통해 의사의 행동을 바꾸는 것이 중요하다.14,19)
본 연구는 다음과 같이 몇 가지 제한점을 가지고 있다.
Group 1의 n수 9명, group 2의 n수 146명으로 두 그룹 간의 n수 의 차이가 많이 나는 점과 group 1과 group 2를 구분 짓는 최종
항암제 투여 후 입원까지 15일이라는 기간에 대한 기준이 불 명확한 점이다. 이는 아마도 호스피스 의뢰 결정까지는 항암 치료 후 치료의 효과, 암의 진행 여부를 보는 추적 관찰기간 이 필요한데 본 연구에서는 15일을 기점으로 유의한 차이를 보인 것으로 생각한다. 또한 고위험군 암인 간담췌암의 경우 group 1에서 5%로 group 2의 30%에 비해 더 적게 관찰되어 이 결과가 생존기간에 영향을 주었을 가능성도 배재할 수 없다.
하지만 본 연구는 우리나라에서 처음으로 호스피스 의뢰 기간과 생존기간과의 관계에 대해서 분석하였다는 점에서 무 엇보다 의미가 있다. 추후 호스피스 의뢰기간과 생존기간과 의 상관관계에 대한 보다 정확한 상관관계에 대한 결과를 얻 기 위해서는 후향적인 충분한 데이터 수집이나 전향적 관찰 연구가 필요하다. 본 연구의 결과를 통해 환자와 가족, 의사 모 두에게 말기 암 환자의 더 나은 삶의 질, 더 긴 생존기간을 위한 호스피스로의 이른 의뢰를 하도록 하는 인식도 제고의 기회 가 되었으면 한다.
요약
연구배경: 최근 말기 암 환자에 있어서의 높은 질의 삶, 통증 및 증상조절을 위한 호스피스 치료에 대한 관심이 높아지고 있다. 이에 본 연구는 말기 암 환자의 호스피스로의 의뢰시기 와 환자의 남은 생존기간 간의 상관관계에 대해 알아보고자 하였다.
방법: 2011년 1월부터 2011년 12월까지 서울성모병원 호스피 스센터에 입실 이후 사망한 155명의 환자의 의무기록을 후향 적으로 분석하였다. 최종 항암제 투여일과 호스피스 병동 입 실일, 사망일을 통하여 최종 항암제 투여 후 입원까지의 기간 및 입원 후 사망까지의 기간을 산출하였다.
결과: Group 1(최종 항암제 투여 후 입원까지 15일 이하)과 group 2(최종 항암제 투여 후 입원까지 15일 초과)의 입원 후 사망까지의 기간에서 group 1의 경우 중간값 26일로 group 2 의 10일에 비해 생존기간이 유의하게 더 길게 나왔다(P=0.035).
결론: 본 연구의 결과로서 말기 암 환자의 진료에 있어서 적절 한 시기에 호스피스로의 이른 의뢰가 환자의 생존기간에 더 유익한 결과를 보였다.
중심단어: 호스피스; 말기암; 생존율; 항암치료
Jung-Wook Lee, et al: Effect of Survival Rate: Perioid from Last Chemotherapy to Hospice Care
80 |
Vol. 3, No. 1 Mar 2013 Korean J Fam PractREFERENCES
1. Earle CC, Neville BA, Landrum MB, Ayanian JZ, Block SD, Weeks JC. Trends in the aggressiveness of cancer care near the end of life. J Clin Oncol 2004;22:315-21.
2. von Gruenigen VE, Daly BJ. Futility: clinical decisions at the end- of-life in women with ovarian cancer. Gynecol Oncol 2005;97:
638-44.
3. Emanuel LL, von Gunten CF, Ferris FD. Gaps in end-of-life care.
Arch Fam Med 2000;9:1176-80.
4. Ferris FD, Bruera E, Cherny N, Cummings C, Currow D, Dudgeon D, et al. Palliative cancer care a decade later:
accomplishments, the need, next steps: from the American Society of Clinical Oncology. J Clin Oncol 2009;27:3052-8.
5. Levy MH, Back A, Benedetti C, Billings JA, Block S, Boston B, et al. NCCN clinical practice guidelines in oncology: palliative care.
J Natl Compr Canc Netw 2009;7:436-73.
6. Follwell M, Burman D, Le LW, Wakimoto K, Seccareccia D, Bryson J, et al. Phase II study of an outpatient palliative care intervention in patients with metastatic cancer. J Clin Oncol 2009;27:206-13.
7. Jordhoy MS, Fayers P, Loge JH, Ahlner-Elmqvist M, Kaasa S.
Quality of life in palliative cancer care: results from a cluster randomized trial. J Clin Oncol 2001;19:3884-94.
8. Temel JS, Greer JA, Muzikansky A, Gallagher ER, Admane S, Jackson VA, et al. Early palliative care for patients with metastatic non-small-cell lung cancer. N Engl J Med 2010;363:733-42.
9. Ho F, Lau F, Downing MG, Lesperance M. A reliability and validity study of the Palliative Performance Scale. BMC Palliat Care 2008;7:10.
10. Greer JA, Pirl WF, Jackson VA, Muzikansky A, Lennes IT, Heist
RS, et al. Effect of early palliative care on chemotherapy use and end-of-life care in patients with metastatic non-small-cell lung cancer. J Clin Oncol 2012;30:394-400.
11. Forster LE, Lynn J. Predicting life span for applicants to inpatient hospice. Arch Intern Med 1988;148:2540-3.
12. Shin HS, Lee HR, Lee DC, Shim JY, Cho KH, Suh SY. Uric acid as a prognostic factor for survival time: a prospective cohort study of terminally ill cancer patients. J Pain Symptom Manage 2006;31:493-501.
13. Christakis NA, Escarce JJ. Survival of Medicare patients after enrollment in hospice programs. N Engl J Med 1996;335:172-8.
14. Friedman BT, Harwood MK, Shields M. Barriers and enablers to hospice referrals: an expert overview. J Palliat Med 2002;5:73- 84.
15. Bennett M, Corcoran G. The impact on community palliative care services of a hospital palliative care team. Palliat Med 1994;
8:237-44.
16. Kwon YC, Shin DW, Lee JH, Heo DS, Hong YS, Kim SY, et al.
Impact of perception of socioeconomic burden on advocacy for patient autonomy in end-of-life decision making: a study of societal attitudes. Palliat Med 2009;23:87-94.
17. Keam B, Oh DY, Lee SH, Kim DW, Kim MR, Im SA, et al.
Aggressiveness of cancer-care near the end-of-life in Korea. Jpn J Clin Oncol 2008;38:381-6.
18. McGorty EK, Bornstein BH. Barriers to physicians’ decisions to discuss hospice: insights gained from the United States hospice model. J Eval Clin Pract 2003;9:363-72.
19. Morita T, Akechi T, Ikenaga M, Kizawa Y, Kohara H, Mukaiyama T, et al. Late referrals to specialized palliative care service in Japan. J Clin Oncol 2005;23:2637-44.