Coronary artery fistulas to cardiac chambers are rare medical conditions and in most cases, are found inciden- tally (1-7). Although the majority of cases are asympto- matic, some may cause coronary steal. For several decades, the conventional coronary angiography has been the best diagnostic modality for identifying coro- nary artery fistulas. However, with recent advances, the coronary angiography was replaced by the development of an electrocardiographically gated multi-detector row computed tomography (MDCT) (1, 8-10). We present a patient with a rare variation of the left anterior descend- ing coronary artery to the left ventricular fistula, which was diagnosed by 64-MDCT.
Case Report
A 67-year-old man was referred from a private clinic to our institution for the evaluation of long standing
chest pain. The patient had a medical history of hyper- tension. Moreover, an echocardiography showed a nor- mal ventricular ejection fraction and a good wall mo- tion, except for aortic valve degeneration with mild mi- tral valve regurgitation. Upon examination, the patient was found to have a blood pressure of 130/84 mmHg and a pulse rate of 52 beats per minute without a mur- mur.
For his cardiac evaluation, a coronary CT angiography (CCTA) was performed with a 64-slice multi-detector system (Brilliance 64; Phillips Medical System, Cleveland, Ohio, U.S.A.). An 18 gauge intravenous catheter was placed in an antecubital vein for venous ac- cess. To achieve a target heart rate of 65 beats per minute or fewer, the patients received a 25 mg oral dose of atenolol (Tenormin; Hyundai Pham, Seoul, Korea) at 30 minutes before the study. In addition, 0.6 mg of Nitroglycerin (Nitroglycerin SL TAB, Myungmoon Pham, Seoul, Korea) was administrated sublingually be- fore the scan initiation. The following imaging and re- construction parameters were used: 1) a detector colli- mation of 0.2 mm, 2) a voltage of 120 kV, 3) an effective current of 1000 mA, 4) a relative pitch of 0.2 seconds, a rotation time of 0.4 seconds, a slice thickness of 0.9 mm,
J Korean Soc Radiol 2010;62:203-205
─ 203 ─
Unusual Coronary Artery Fistula: Left Anterior Descending Coronary Artery - Left Ventricular Fistula Diagnosed by ECG-Gated Multi-
Detector Row Coronary CT Angiography
1Jiyoung Oh, M.D., Soon-Young Song, M.D., Yo Won Choi, M.D., Seok Chol Jeon, M.D.
1Department of Radiology, Hanyang University Medical College, Korea Received October 15, 2009 ; Accepted October 25, 2009
Address reprint requests to : Soon-Young Song, M.D., Department of Radiology, Hanyang University Seoul Hospital, 17 Haengdang-dong, Sungdong-ku, Seoul 133-792, Korea.
Tel. 82-2-2290-9160 Fax. 82-2-2293-2111 E-mail: [email protected]
Coronary artery fistulas to cardiac chamber are an uncommon condition. In most cases, coronary arteries empty into the right chambers and left coronary artery-left ventricular fistula is a very rare condition. We report a case of a left anterior descend- ing coronary artery-left ventricular fistula in a 67-year-old man, which was diagnosed by a 64-multi-detector row coronary CT angiography.
Index words :Tomography, X-Ray Computed Coronary Angiography
Coronary Artery Disease Fistula
and a reconstruction interval 0.45 mm. In total, 80 milli- liters of nonionic contrast material (iopromide, Ultravist 370; Schering, Berlin, Germany) was injected through an antecubital vein at a rate of 5 mL/s via a dual-syringe injector (Stellant D; Medrad, Indiana, Pa, U.S.A.). The injection was immediately followed by a 40-mL saline flush at a rate of 5 mL/s. For timing purposes, automat- ed bolus tracking software was used with the com- mencement of image acquisition when the contrast den- sity reached a predefined threshold of 150 Hounsfield units in the ascending aorta. The post-processing tech- niques, including multi-planar reformation, maximum- intensity projections, and volume-rendered reconstruc- tions, were performed on a PC-based 3-dimensional software (Rapidia 2.8; Infinit, Seoul, Korea).
On CCTA, there was a tortuous distal artery from the distal left anterior descending artery (LAD), which was connected into the base of the left ventricle (Fig. 1). We
diagnosed it as a coronary artery to left ventricular fistu- la.
Discussion
Congenital coronary anomalies are rare conditions and are diagnosed incidentally by a coronary angiogra- phy or autopsy. Coronary artery anomalies may be found incidentally in 0.3-1% of the healthy population.
Coronary artery fistulas account for 15% of all coronary artery anomalies (1, 2). Approximately 60% of these fis- tulas arise from the right coronary artery (RCA). In most cases, it terminates in the right side of the heart in 90%
of the cases. Drainage to the left ventricle is the least common (2).
Only five cases of the LAD to left ventricular fistulas have been reported in the previous English literature thus far. The LAD to the left ventricular fistulas arose
Jiyoung Oh, et al: Unusual Coronary Artery Fistula
─ 204 ─
A B
C
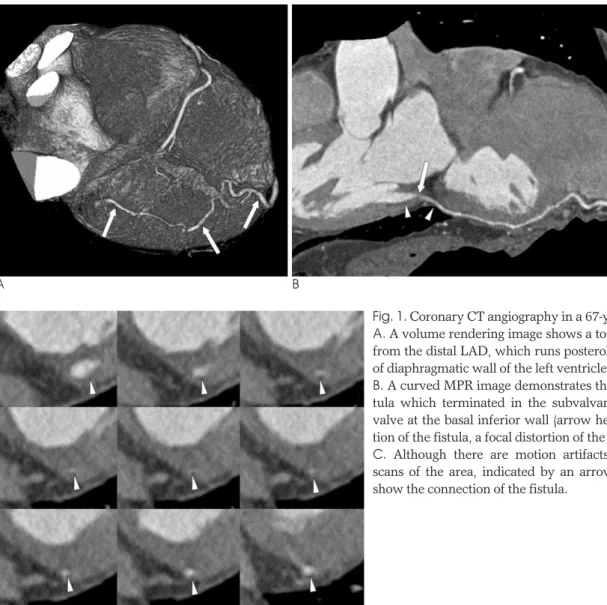
Fig. 1. Coronary CT angiography in a 67-year-old male patient.
A. A volume rendering image shows a tortuous branch (arrows) from the distal LAD, which runs posterolaterally on the surface of diaphragmatic wall of the left ventricle.
B. A curved MPR image demonstrates the connection of the fis- tula which terminated in the subvalvar portion of the mitral valve at the basal inferior wall (arrow heads). At the distal por- tion of the fistula, a focal distortion of the image is seen (arrow).
C. Although there are motion artifacts, cropped serial axial scans of the area, indicated by an arrow in figure 1B, clearly show the connection of the fistula.
from single or multiple origins of the left coronary artery (3-7). When the fistula connection is to a left-sided car- diac chamber, a coronary artery fistula that drains to the left ventricle produces hemodynamic changes similar to aortic insufficiency. Myocardial perfusion may be de- creased for the portion of the myocardium, which is supplied by the abnormally connecting coronary artery and this situation represents a hemodynamic steal (1, 2).
For the several decades, the diagnosis of coronary artery anomalies was made with a conventional coro- nary angiography. However, with progress in the method (MDCT), the CCTA has been accepted as the new standard method for visualizing the origin, while the 3-D display of the anatomy is in contrast with demonstrating the 2-D display of the anomalous artery in the conventional angiography (8-10). For patients with atypical chest pain, the non-invasive CCTA is help- ful for a physician to exclude a cardiac etiology with a high negative predictive value. The physicians can un- derstand the complex anatomy of coronary anomalies better and hence, contemplate interventions made, thor- oughly based on 3-D volume rendered images (9).
Our case had two limitations. First, we could not clari- fy the hemodynamic significances or myocardial changes relating to the fistula, because additional imag- ing studies such as conventional coronary angiography or nuclear perfusion testing were not performed.
Second, follow-up results were not obtained. Despite these limitations, our case demonstrated the ease of di- agnosis of this rare variation with use of the CCTA. To
our knowledge, we present the first case of LAD to the left ventricular fistula which was diagnosed by CCTA.
References
1. Kim SY, Seo JB, Do K-H, Heo J-N, Lee JS, Song J-W, et al.
Coronary artery anomalies: classification and ECG-gated multi-de- tector row CT findings with angriographic correlation.
Radiographics 2006;26:317-333
2. Latson LA. Coronary artery fistulas: how to manage them.
Catheter Cardiovasc Interv 2007;70:110-116
3. Papazoqlou PD, Mitsibounas D, Nanas JN. Left anterior descend- ing coronary artery-left ventricular fistula presenting as unstable angina and syncope. Int J Cardiol 2004;96:121-122
4. Lozano I, Batalla A, Rubin J, Avanzas P, Martin M, Moris C.
Sudden death in a patient with multiple left anterior descending coronary artery fistula to the left ventricle. Int J Cardiol 2008;
125:e37-e39
5. Kiuchi K, Nejima J, Kikuchi A, Takayama M, Takano T, Hayakawa H. Left coronary artery-left ventricular fistula with acute myocardial infarction, representing the coronary steal phe- nomenon: a case report. J Cardiol 1999;34:279-284
6. Arani DT, Greene DG, Klocke FJ. Coronary artery fistulas empty- ing into left heart chambers. Am Heat J 1978;96:438-443
7. Sambu N, Sharma R, Kalra PR. Multiple coronary to left ventricu- lar fistulae. Eur J Echocardiogr 2009;10:352
8. Duran C, Kantarci M, Durur Subasi I, Gulbaran M, Sevimli S, Bayram E, et al. Remarkable anatomic anomalies of coronary ar- teries and their clinical importance: a multidetector computed to- mography angiographic study. J Comput Assist Tomogr 2006;30:
939-948
9. Zenia AR, Blinder J, Sharif D, Rosenschein U, Barmeir E.
Congenital coronary artery anomalies in adults: non-invasive as- sessment with multidetector CT. Br J Radiol 2009;82:254-261 10. Datta J, White CS, Gilkeson RC, Meyer CA, Kansal S, Jani ML, et
al. Anomalous coronary arteries in adults: depiction at multi-detec- tor row CT angiography. Radiology 2005;235:812-818
J Korean Soc Radiol 2010;62:203-205
─ 205 ─
대한영상의학회지 2010;62:203-205
보기 드문 관상동맥루:
관상동맥 다절편 전산화 단층촬영 혈관 조영술로 진단된 좌전하행 관상동맥-좌심실간 관상동맥루11한양대학교병원 영상의학과 오지영∙송순영∙최요원∙전석철
심강과 연결된 관상동맥루는 흔하지 않으며, 대부분은 우심강과 연결되어 좌측 관상동맥-좌심실간 관상동맥루는 매우 드문 경우이다. 저자들은 67세 남자에서 64-다절편 전산화단층촬영 혈관조영술로 진단되었던 좌전하행 관상동 맥-좌심실간 관상동맥루를 경험하였기에 이의 영상의학적 소견을 보고하고자 한다.