ORIGINAL ARTICLE
Received: September 18, 2018, Revised: October 4, 2018, Accepted: October 9, 2018 Corresponding author: Tae Kyung Ha, 222 Wangsimni-ro, Seongdong-gu, Seoul 04763, Korea
Department of Surgery, Hanyang University College of Medicine
Tel: +82-2-2290-8443, Fax: +82-2-2281-0224, E-mail: [email protected]
CC This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
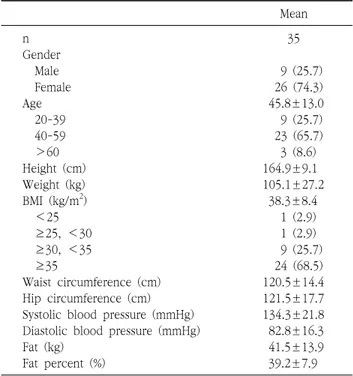
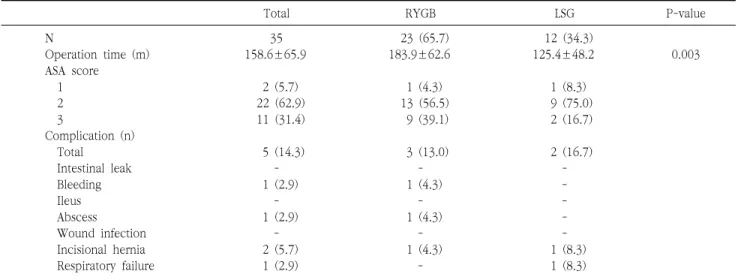
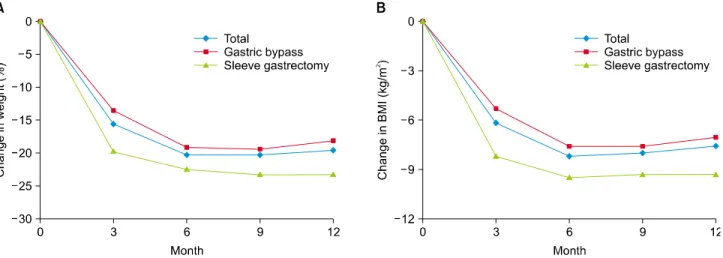
Characteristics of Bariatric Surgery Patients in a Single University Hospital
1