Le Fort I 골절단술을 통한 상악의 후상방 회전에 따른 상순과 비부의 연조직 변화
권영욱
1, 표성운
2, 이 원
3, 박재억
11
가톨릭대학교 서울성모병원,
2가톨릭대학교 부천성모병원,
3가톨릭대학교 의정부성모병원 구강악안면외과
Abstract(J Korean Assoc Oral Maxillofac Surg 2011;37:457-63)
Soft tissue changes of upper lip and nose following posterosuperior rotation of the maxilla by Le Fort I osteotomy
Young-Wook Kwon
1, Sung-Woon Pyo
2, Won Lee
3, Je Uk Park
1Department of Oral and Maxillofacial Surgery,
1Seoul St. Mary's Hospital, The Catholic University of Korea, Seoul,
2
Bucheon St. Mary's Hospital, The Catholic University of Korea, Bucheon,
3
Uijeongbu St. Mary's Hospital, The Catholic University of Korea, Uijeongbu, Korea
Introduction: This study evaluate the soft tissue changes to the upper lip and nose after Le Fort I maxillary posterosuperior rotational movement.
Materials and Methods: Twenty Skeletal class III patients, who had undergone bimaxillary surgery with a maxillary Le Fort I osteotomy and bilateral sagittal split ramus osteotomy, were included in the study. The surgical plan for maxilla was posterosuperior rotational movement, with the rotation center in the anterior nasal spine (ANS) of maxilla. Soft and hard tissue changes were measured by evaluating the lateral cephalograms obtained prior to surgery and at least 6 months after surgery. For cephalometric analysis, four hard tissue landmarks ANS, posterior nasal spine [PNS], A point, U1 tip), and five soft tissue landmarks (pronasale [Pn], subnasale [Sn], A' Point, upper lip [UL], stomion superius [StmS]) were marked.
A paired t test, Pearson's correlation analysis and linear regression analysis were used to evaluate the soft and hard tissue changes and assess the correlation. A P value <0.05 was considered significant.
Results: The U1 tip moved 2.52±1.54 mm posteriorly in the horizontal plane (P<0.05). Among the soft tissue landmarks, Pn moved 0.97±1.1 mm downward (P<0.05), UL moved 1.98±1.58 mm posteriorly (P<0.05) and 1.18±1.85 mm inferiorly (P<0.05), and StmS moved 1.68±1.48 mm posteriorly (P<0.05) and 1.06±1.29 mm inferiorly (P<0.05). The ratios of horizontal soft tissue movement to the hard tissue were 1:0.47 for the A point and A' point, and 1:0.74 for the U1 tip and UL. Vertically, the movement ratio between the A point and A' point was 1:0.38, between U1 tip and UL was 1:0.83, and between U1 tip and StmS was 1:0.79.
Conclusion: Posterosuperior rotational movement of the maxilla in Le Fort I osteotomy results in posterior and inferior movement of UL. In addition, nasolabial angle was increased. Nasal tip and base of the nose showed a tendency to move downward and showed significant horizontal movement.
The soft tissue changes in the upper lip and nasal area are believed to be induced by posterior movement at the UL area.
Key words: Orthognathic surgery, Le Fort osteotomy, Cephalometry, Angle class III malocclusion
[paper submitted 2011. 6. 13 / revised 2011. 8. 30 / accepted 2011. 10. 12]
료결과를얻기어려운경우고려된다
.
상악과하악의다양 한악교정술식중1901
년Rene Le Fort
에의해서명명된두 개안면부의골절술중하나인Le Fort I
골절단술은1859
년 에von Langenbeck
1에의해서처음기술되었다. Cheever
2는
1867
년상악의이동을처음기술하였고, Wassmund
3는1927
년에Le Fort I
골절단술을악교정수술에처음적용하였다
.
이후Axhausen
4, Schuchardt
5 등에의해서수술방법 이발전되었고, 1960
년대에Obwegeser
6가Le Fort I
을이용 한다양한수술방법을정리,
보고하여Le Fort
골절단술이 널리활용되는계기가되어최근30
년간전세계적으로보편적인술식이되었다
.
이러한상악의Le Fort I
골절단술을I. 서 론
악교정수술은 골격성부정교합환자들의치료에 있어 서교정치료만으로기능적인교합과심미적인안모의치 박 재 억
137-501 서울시 서초구 반포동 505
가톨릭대학교 서울성모병원 구강악안면외과 Je Uk Park
Department of Oral and Maxillofacial Surgery, Seoul St. Mary's Hospital, The Catholic University of Korea
505 Banpo-dong, Seocho-gu, Seoul, 137-501, Korea TEL: +82-2-2258-6291 FAX: +82-2-237-5374 E-mail: [email protected]
비발치치료를하였고
,
상악은18
명에서비발치치료를하 였다.
상악치아발치가이루어진환자들에서1
명의경우양 측제1
소구치의발치그리고2
명에있어서편측제2
소구치 의발치가시행되었다.
이들중수술전과수술후6
개월까 지에서발치공간의변화는1
명에서만관찰되었다.
2. 연구 방법
이 논문은 가톨릭대학교 생명윤리심의위원회
(Institu-
tional Review Board)
의 승인을 받아시행되었다(
과제번호
:KC11RASI0042).
1)
측모두부방사선사진의촬영및계측수술전
1
개월이내(T0),
그리고수술후6
개월이후(T1)
에측모두부계측방사선사진이자연두부위치,
중심위교합 상태,
그리고상순과하순이이완된상태에서촬영되었다.
측모두부계측방사선 사진의 계측은
V-Ceph (Ver. 5.5,
Cybermed, Seoul, Korea)
를 이용하여 단일검사자에 의해서 시행되었다
.
측모두부계측방사선의 분석은 수정된Burstone
등12, Legan
과Burstone
13의 방법을사용해서시 행하였다.
수평기준선(horizontal reference line, HRL)
은 포함하는악교정수술은골격성부정교합의치료에있어서자주선택되어시행되고있다
.
상악의악교정수술중상악 의상방이동에대한안정성을Proffit
등7이알아본바있고,
42
명을1
년이상경과관찰했을때매우안정적인술식임을보고하였다
.
또한Baek
등8은성인환자20
명을대상으로 한연구에서상악의후상방회전움직임을시행했을때수 술후1
년까지안정적임을보고한바있어그안정성이검 증되었다.
그동안안면골의움직임에따른연조직의변화를예측 하기위한여러가지연구방법들이시행되어왔다
.
측모두 부계측방사선사진을활용한방법, videocephalometric
예측방법그리고최근에는
computed tomography
를활용한삼차원적인방법등이있다
.
그중에서도측모두부계측방사선사진을활용한방법은
1930
년대에보고되기시작하여현재까지악교정치료의계획수립에있어서기본적인방법으 로활용되고있다
.
상악의
Le Fort I
골절단술의시행후이에상응하는연조직변화에대한많은연구들이보고되고있다9-35
.
하지만이 러한상악이동과연관된상순및비부연조직의변화에대 한연구들은주로상악의전방또는상방이동에관한것이었다10,14,15,19,21-25
.
그러나최근에는안모의심미에대한개념이바뀌면서기능적인교합을가지고있더라도전안면고경 및이부전돌의감소를위해 상악을후상방이동하는양악 수술을시행하는경우가급격히증가하고있다
.
즉심미적 안모의형성을위해서상악의시계방향의회전이동이근래 에많이시행되고있다.
따라서이에따른상순과비부의연 조직변화에대한연구가필요하다고생각되었다.
본연구 에서는상악수술에서 설정할수있는 여러회전중심점들 중에서상악기저골의전후방적인위치변화를계획하지않 고anterior nasal spine (ANS)
을회전점으로하여후상방회 전한증례들에있어서,
그에따른상순및비부의변화를알 아보아향후 보다예지성있는악교정수술계획의수립에 도움이되고자하였다.
II. 연구 대상 및 방법
1. 연구 대상
2008
년10
월에서2010
년3
월 사이에 가톨릭대학교의과대학서울성모병원구강악안면외과에내원하여
Le Fort I
골절단술 및 양측성 하악골상행지 시상분할 골절단술(bilateral sagittal split ramus osteotomy, BSSRO)
을시행받 은골격성III
급부정교합환자군중ANS
를회전중심으로 하여상악골을후상방으로회전이동한 뒤수술후6
개월 경과관찰한환자군을대상으로하였다.
남자는10
명(
범위20-30
세,
평균23
세),
여자는11
명(
범위20-37
세,
평균26.5
세)
이었다.
수술전후교정치료에있어서21
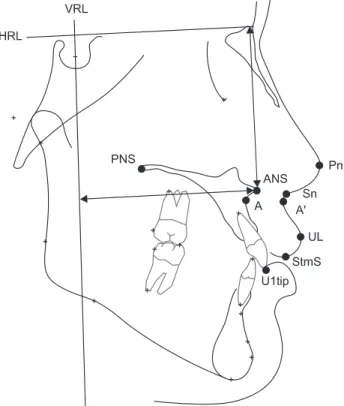
명모두하악은Fig. 1. Cephalometric landmarks and reference planes. (ANS:
anterior nasal spine, PNS, posterior nasal spine; A, A point; U1 tip, upper incisor tip; Pn, pronasale; Sn, subnasale; A', soft tissue A point; UL, upper lip; StmS, Stomion superius)
Young-Wook Kwon et al: Soft tissue changes of upper lip and nose following posterosuperior rotation of the maxilla by Le Fort I osteotomy. J Korean Assoc Oral Maxillofac Surg 2011
측값들의신뢰도를확인하기위해급내상관계수
(intraclass correlation coefficient)
를확인하였고,
모든계측점에대해서
0.99
보다큰값을보이는높은신뢰도를보였다.
통계분석프로그램으로는
SAS system version 9.1 (SAS Institute Inc., Cary, USA)
를사용하였다.
III. 결 과
1. 수술 전과 수술 후 6개월 계측값의 비교
A point
는수평적으로1.5±1.43 mm
후방이동양상을보였다
(P<0.05). U1 tip
은수평적으로후방으로2.52±1.54 mm
이동하였고(P<0.05), PNS
는수직적으로4.76±1.38 mm
상 방이동하였다( P<0.05). (Table 1)
연조직 점들 중
Pn
은 수직적으로 하방0.97±1.1 mm (P<0.05), Sn
은하방1.05±0.9 mm (P<0.05), A' point
는하방1±0.84 mm (P<0.05)
이동하였다. UL
점은후방으로1.98±
1.58 mm (P<0.05),
하방으로1.18±1.85 mm (P<0.05)
이동 하였고, StmS
점은후방으로1.68±1.48 mm (P<0.05),
하방 으로1.06±1.29 mm (P<0.05)
이동하였다.
각도계측값 중
palatal plane angle
은수술로 평균5.9±
2.24
o증가하였으며(P<0.05),
상악전치각도는3.73±3.97
o감 소하였다( P<0.05). Nasolabial angle
은5.93±4.93
o증가하였 다(P<0.05).
2. 경조직과 연조직 계측값들의 상관관계
수평적으로
U1 tip
와UL
간(r=0.73, P<0.05)
의강한(r>0.7)
양의상 관관계가관찰되었다. A point
와A' point
간에는중등도의(0.7>r>0.3)
양의상관관계가 관찰되었다(r=0.59, P<0.05).
(Table 2) Sella-Nasion plane-7
o상방선으로설정하였다.
수직기준선(vertical reference line, VRL)
은Sella
를지나면서HRL
에수 직인선으로하였다.
계측항목은아래와같다.(Fig. 1)
(1)
상악골이동에 따른경조직수직변화(HRL
에의수직거리
): U1 tip, A point, ANS, posterior nasal spine (PNS)
(2)
상악골이동에따른경조직수평변화(VRL
에의수직거리
): U1 tip, A point, ANS, PNS
(3)
상악골이동에따른경조직각도 변화: palatal plane angle to HRL,
상악전치의HRL
에대한각도(U1 to HRL)
(4)
상악골이동에따른연조직수직변화: pronasale (Pn), subnasale (Sn), soft tissue A point (A' point), upper lip (UL), stomion superius (StmS)
(5)
상악골 이동에 따른연조직 수평변화: Pn, Sn, A' point, Upper lip, StmS
(6)
상악골 이동에 따른 연조직 각도변화: nasolabial
angle
2)
통계분석술전 계측값과술 후
6
개월계측값 간에유의성있는차이가있는지를알아보기 위하여
paired t-test
를 사용하여 평가하였다
.
또한경조직 계측점의 변화에 대한연조 직계측점 변화값의상관관계를알아보고 경조직의 변화에대한연조직변화의비율을산출하기위해서
Pearson's
correlation analysis
와linear regression analysis
를시행하였 다. P<0.05
인경우유의성이있는것으로설정하였다.
측모두부계측방사선사진계측의신뢰성을확인하기위 해서
10
개의측모두부방사선사진을무작위선정하여 동 일한검사자가처음계측시행한날로부터1
개월후에다시
tracing
하여계측하였다.
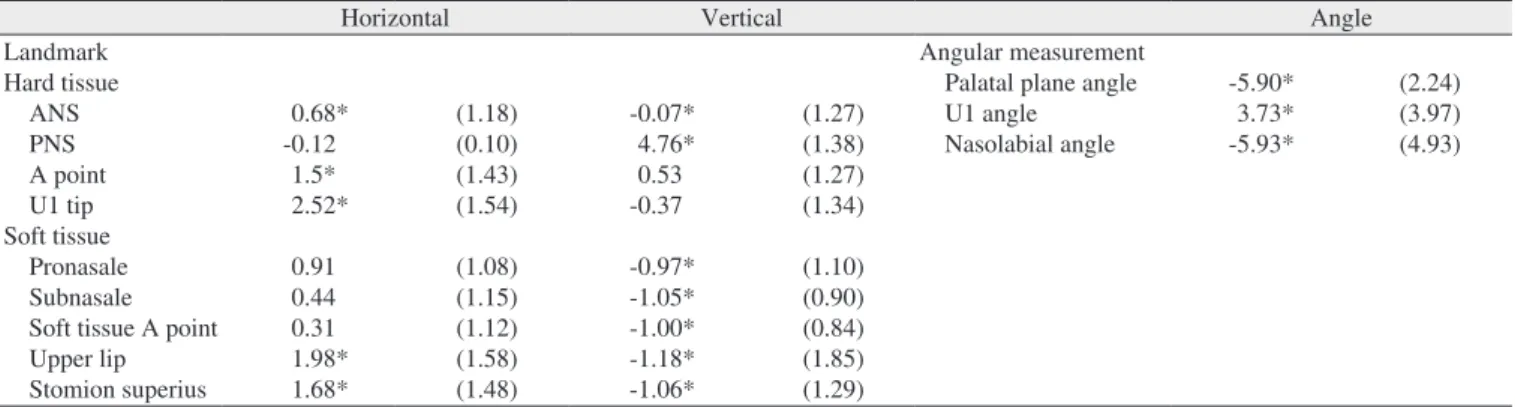
측모두부계측방사선사진계Table 1. Horizontal, vertical (mm) and angular (o) changes of hard and soft tissue landmarks (T0-T1)
Horizontal Vertical Angle
Landmark Hard tissue ANS PNS A point U1 tip Soft tissue Pronasale Subnasale Soft tissue A point Upper lip Stomion superius
0.68*
-0.12 1.5*
2.52*
0.91 0.44 0.31 1.98*
1.68*
(1.18) (0.10) (1.43) (1.54) (1.08) (1.15) (1.12) (1.58) (1.48)
-0.07*
4.76*
0.53 -0.37 -0.97*
-1.05*
-1.00*
-1.18*
-1.06*
(1.27) (1.38) (1.27) (1.34) (1.10) (0.90) (0.84) (1.85) (1.29)
Angular measurement Palatal plane angle U1 angle Nasolabial angle
-5.90*
3.73*
-5.93*
(2.24) (3.97) (4.93)
(ANS, anterior nasal spine; PNS, posterior nasal spine) (*P<0.05)
Values are presented as mean (standard deviation).
Positive value inhorizontal movement indicates posterior movement and negative value indicates anterior movement.
Positive value in vertical movement indicates superior movement and negative value indicates inferior movement.
Young-Wook Kwon et al: Soft tissue changes of upper lip and nose following posterosuperior rotation of the maxilla by Le Fort I osteotomy. J Korean Assoc Oral Maxillofac Surg 2011
전의연구들을통해서대부분의
Le Fort I
상악수술에따른 연조직변화가비부와상순에서이루어지는것이관찰되었다17,18,20
.
그동안여러방향의상악의움직임에상응하는연조직의위치변화 정도를알아보는 연구들이 시행되어왔 다
.
하지만상악의후상방회전이동에의한상순및비부연 조직변화에대한연구는부족하였고,
그중에서도상악의특정회전점
(rotation center)
을중심으로한시계방향의회전이동에의한상순및비부연조직의변화에대해서평가 한연구는없었다
.
따라서본연구에서는ANS
를중심으로 상악을후상방으로회전한경우비부및상순의연조직변 화를평가하였다.
본연구의경조직계측점들중에서수술계획시에상악 골의 회전기준점으로설정하였던
ANS
가수술후에수평,
수직적으로유의한이동이있었던것으로관찰되었다. Le
Fort I
골절단술후상악골을수술계획대로위치시키는것과 관련하여
Jacobson
과Sarver
36는1
명의 교정의와2
명 의외과의가치료한46
명의 환자들을대상으로한연구에 서,
시상면상에서환자군의43%
는1 mm
이내, 80%
에서2 mm
오차범위내로수술이이루어졌다고하였고, Semaan
과Goonewardene
37은42
명의환자들을대상으로한연구에 서66%
의환자들에서시상면상에서2 mm
오차범위내로 수술이이루어졌다고하였다.
본연구에서ANS
는수평적 으로는후방으로0.68±1.18 mm ( P<0.05),
수직적으로는하 방으로0.07±1.27 mm ( P<0.05)
이동하였다.
이는비록수술 계획에서ANS
를회전중심으로설정하였지만수술시에발 생하는오차로인하여실제적인이동이있었다는것을의 미한다.
하지만그 오차는통상적으로 받아들여지는범위 내에있었고임상적으로무의미한이동량이었다고생각된 다.
상악의이동에의해서비부의형태는영향을받는다14-18,24,25,27
.
특히비첨부를포함한하방부의변화가두드러져서
,
코의 너비(alar width),
비첨부의돌출정도,
비소주길이, nasobla-
bial angle
의 변화가 나타나게 된다.
상악의이동방향에수직적으로
, A point
와A' point (r=0.57, P<0.05),
그리고U1 tip
과UL
간에는중등도의양의상관관계가관찰되었다
(r=0.61, P<0.05). U1 tip
과StmS
의수직이동간에는강한 양의상관관계가관찰되었다(r=0.82, P<0.05).
각도계측값들은상악전치각도와
nasolabial angle
간에 중등도의음의상관관계(r=-0.44, P<0.05)
가관찰된것이외 에는유의한상관관계가관찰되지않았다.(Table 3)
3. 연조직 계측점의 경조직 계측점에 대한 변화 비율
수평적인연조직계측점의경조직움직임에대한이동비 율은
A point
의후방이동에대해서A' point
는1 : 0.47, U1 tip
의후방이동에대한UL
의이동비율은1 : 0.74
이었다.
수직 적으로, A point
와A' point
는1 : 0.38, U1 tip
과UL
은1 : 0.83, U1 tip
과StmS
는1 : 0.79
의이동비율을보였다.(Table 2)
IV. 고 찰
골격성
III
급부정교합환자에서심미,
교합및저작기능 개선의목적으로하악의수술만으로는부족한경우하악과 더불어상악의악교정수술이시행되고있다.
특히전치부 개교합,
하악 이부및상순 전돌해소등의 목적으로상악 의후상방회전움직임을시행하는경우가흔히있다.
이러 한목적의상악의시계방향회전을통해서교합평면의시 계방향회전,
상악전치각도의감소,
후안면고경의증가방 지효과가동시에이루어진다.
이러한악교정수술계획을 수립함에있어서상악의움직임에따른해당부위연조직의 이동양상을미리고려하여치료결과를예측하는것은악 교정수술의성공을위해서는필수적이라고할수있다.
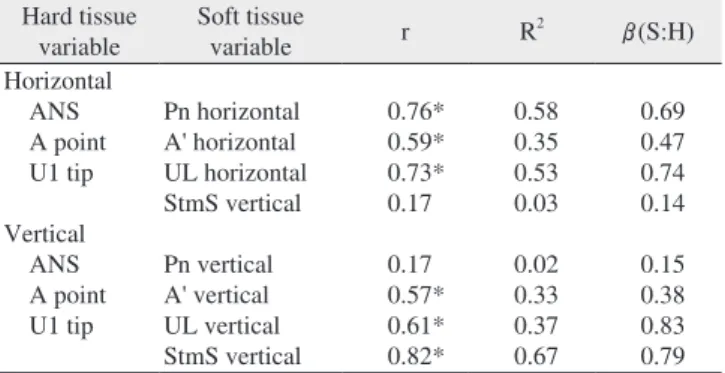
이Table 2. Correlations between corresponding soft to hard tissue movements and soft to hard tissue movement ratios in both horizontal and vertical planes
Hard tissue
variable Soft tissue
variable r R2 β(S:H)
Horizontal ANS A point U1 tip Vertical ANS A point U1 tip
Pn horizontal A' horizontal UL horizontal StmS vertical Pn vertical A' vertical UL vertical StmS vertical
0.76*
0.59*
0.73*
0.17 0.17 0.57*
0.61*
0.82*
0.58 0.35 0.53 0.03 0.02 0.33 0.37 0.67
0.69 0.47 0.74 0.14 0.15 0.38 0.83 0.79 (r: Pearson correlation coefficient, R2: coefficient of determination, ANS: anterior nasal spine, PNS: posterior nasal spine, Pn: pronasale, UL: upper lip, StmS: stomion superius)
(*P<0.05)
Young-Wook Kwon et al: Soft tissue changes of upper lip and nose following posterosuperior rotation of the maxilla by Le Fort I osteotomy. J Korean Assoc Oral Maxillofac Surg 2011
Table 3. Correlations between hard tissue angular changes to soft tissue movement and their ratios
Angular
measurement Soft tissue
variable r R2 β(S:H)
U1 to HRL Palatal plane angle
UL horizontal StmS vertical Nasolabial angle UL horizontal StmS vertical Nasolabial angle
0.22 -0.22 -0.44*
0.01 0.23 0.14
0.05 0.05 0.19 0.0001 0.05 0.02
0.09 -0.07 -0.54
0.007 0.13 0.31 (r: Pearson correlation coefficient, R2: coefficient of determination, HRL: horizontal reference line, UL: upper lip, StmS: stomion superius) (*P<0.05)
Young-Wook Kwon et al: Soft tissue changes of upper lip and nose following posterosuperior rotation of the maxilla by Le Fort I osteotomy. J Korean Assoc Oral Maxillofac Surg 2011
으로
1.18±1.85 mm (P<0.05)
하방위치하는것을확인할수 있었다. U1 tip
과UL
은수평적으로는1 : 0.74,
수직적으로는
1 : 0.83
의높은비율의상호관련성을보여주었다.
기존의연구들에서하악만을
BSSRO
시행하여후방이 동하였을때 상순이하악전치에 대해서0.2 : 1
의 비율로 후방이동하는것이보고된바있다9,38,39.
본연구의환자들 은상악수술과하악수술을동시에시행하였으므로,
하악BSSRO
에의한상순에의영향이있을것으로생각된다.
A' point
는 수평적으로는유의한이동을보이지않았고,
수직적으로는
1.06±1.29 mm (P<0.05)
하방으로이동하였다
.
이러한차이는A' point
가회전점에UL
보다가깝게위치하기때문이라고생각할수있다
. Chew
27는A point
에상 응하는연조직점으로Sn
을설정하였고,
수평적으로는1 : 0.6,
수직적으로는1:0.57
의비율을보인다고하였다.
본연구에서는
A point
에상응하는연조직점을A' point
로설정하였는데
, Chew
27의 연구보다는작은이동비율인수직적으로1 : 0.38
의비율이관찰되었고수평적으로는유의한변화가관찰되지않았다
.
Jeong
등28은16
명의골격성3
급부정교합환자들에서상 악의시계방향회전이동을시행하였을때,
상순의길이,
비 순각이 증가하고,
상순의 전방점이후방으로이동한다고 하였다.
이러한점은본연구에서도 확인되었다.
먼저,
상 악의시계방향회전이동후에UL
점이수평적으로후방이 동하였고, StmS
점이수술후에1.06±1.29 mm (P<0.05)
하 방위치하였다.
이를통해서상순의HRL
에대해서수직적인길이의증가가있었다고생각할수있다
.
하지만U1 tip
의 수평적 후방이동에 대한
StmS
의 수직적 위치의 유의 한 상관관계는관찰되지않았다. U1 tip
의수직적 이동에대한
StmS
의수직적위치변화는높은 상관관계를보였고(r=0.82, P<0.05),
이동비율은1 : 0.79
였다.
두번째로
,
술후에nasolabial angle
의5.93±4.93
o증가가 관찰되었다(P<0.05). Nasolabial angle
의증가는상악전치 각도값과중등도의 음의상관관계를보였고반비례하는 양상이었다(r=-0.44, P<0.05, β=-0.54).
상악의시계방향으로의회전이동에의해서비첨부에서
StmS
까지의연조직은대부분유의한하방이동을나타내었 고,
수평적으로는회전점에서떨어진UL
과StmS
에서만유 의한후방이동을보였다. Chew
등29에의한연구에서, 30
명 의중국인골격성III
급부정교합자의상악골Le Fort I
전진 술시행시에연조직의이동비율이상악전치와상순부위에 서는선형적인양상이었지만, ANS
와Sn
부위에서는비선 형적인곡선의관계를보였다고하였고,
상악의이동에따 른상순의이동비율은상악의이동량,
상순의치아-
치조구 조물에의해지지되는양상에따라서달라질수있다고하 였다.
따라서수술결과를예측하려면술전치아-
치조구조 물과상순의관계,
상악의이동계획량,
연조직저항성등이 고려되어야한다.
따라서비부의 연조직변화 양상이 달라진다
. O’Ryan
과Carlotti
16는상악의후방이동시에비기저부(alar base)
에는 별다른변화가없고,
비첨부돌출은감소, nasolabial angle
은증가된다고하였다. Radney
와Jacobs
14는상악의상방이 동시에 비첨부는전방이동하게되고,
상방이동과전방이 동이같이이루어질경우보다많은전방이동을보이게된 다고하였지만통계적인비율을제시하지않았다.
또한,
상 악의상방이동과후방이동이같이이루어질경우비첨부의수평적인위치는변함이없다고하였다
. Mansour
등15은상악의전방이동시에상악전치와
Pn
의이동비율이1 : 0.17
이 라고하였다. Park
과Lee
24는상악의전방이동시에Pn
은수평적으로
32%
전방이동,
수직적으로9%
상방이동하였고,
상악의상방이동시에는상방으로
15%,
수평적으로15%
전방이동하였다고하였다
. Chew
27는34
명의중국인골격성III
급부정교합환자의양악수술시행후에ANS
의수평적인이동에대해서
Pn
이1 : 0.35
비율의이동양상을보인다고하였다
(r=0.56, P<0.01).
또한ANS
의수직적인이동에대해 서Pn
은1 : 0.33
비율의이동양상을보인다고하였다(r=0.36,
P<0.05).
하지만상악의수술적이동방향에대해서언급한바는없었고상악골이동량의평균값을보았을때전상방 이동이었다
.
이번연구에서상악의ANS
를기준으로한시계 방향회전움직임이후에Pn
은수평적으로는유의한변화를 보이지않았고수직적으로0.97±1.1 mm
하방이동하였다( P<0.05).
비부의하방부에위치하는Sn
은술후에 수평적 으로는유의한움직임이없었던반면에,
수직적으로는Pn
과유사하게하방으로이동하였다(1.05±0.9 mm, P<0.05).
상순은상악의수술에의해서많은영향을받게된다
.
하 지만,
하순과는다르게상순은비부구조물에연결되어있어
,
경조직에대해서1 : 1
에가까운변화량을보이지않게된다9
. Chew
27는상악중절치의이동에대해서상순은1:0.84
의이동비율을보인다고하였다. Mansour
등15은상악골의 전방이동시에상악전치에대해서상순의변화율이1:0.62
라고하였다
. Park
과Lee
24는상악골의전방이동에대해서상순이
62%,
전상방이동시에는56%
의연조직변화비율을보였다고하였다
.
상순의 길이는상악의상방이동시에25%,
전상방이동시에는31%
짧아지는변화를보였다고하였다
. Schendel
등11은상악의후방이동시에상순의상악전치에대한이동비율이
1 : 0.76
임을보고하였고, Radney
와Jacobs
14는1 : 0.67
의비율을보인다고하였다.
본연구에서는
1 : 0.74
의비율을보였다.
하지만이들의연구는상악의상방이동을동반한후방이동이었다
.
상순의후방이동을위한변형된
Cupar
법으로의상악전치부분절골 절단술을시행한
Park
과Hwang
33의연구에의하면,
상악전치부분절 골절단술을통한후방이동하는것에의한상악전치와상 순의이동비율은1 : 0.67
로상악의전체적인이동보다작 았다.
본연구에서상악의시계방향회전후에UL
이수평 적으로1.98±1.58mm (P<0.05)
후방이동하는것과,
수직적References
1. von Langenbeck B. Beiträge zur osteoplastik - Die osteoplastische resektion des oberkiefers. In: Göschen A, ed. Deutsche Klinik.
Berlin: Reimer; 1859.
2. Cheever DW. Naso-pharyngeal polypus, attached to the basilar process of occipital and body of the sphenoid bone successfully removed by a section, displacement, and subsequent replacement and reunion of the superior maxillary bone. Boston Med Surg J 1867;8:162.
3. Wassmund M. Frakturen und Luxationen des Gesichtsschädels.
Leipzig: Meusser; 1927.
4. Axhausen G. Technik und Ergebnisse der Lippenplastiked.
Leipzig: Thieme; 1941.
5. Schuchardt K. Ein Beitrag zur chirurgischen Kieferorthopädie unter Berücksichtigung ihrer Bedeutung für die Behandlung angeborener und erworbener Kieferdeformitäten bei Soldaten.
Dtsch Zahn Mund Kieferheil 1942;9:73-89.
6. Obwegeser H. [Surgery of the maxilla for the correction of prognathism]. SSO Schweiz Monatsschr Zahnheilkd 1965;75:365- 74.
7. Proffit WR, Turvey TA, Phillips C. The hierarchy of stability and predictability in orthognathic surgery with rigid fixation: an update and extension. Head Face Med 2007;30:3-21.
8. Baek SH, Kim K, Choi JY. Evaluation of treatment modality for skeletal Class III malocclusion with labioversed upper incisors and/
or protrusive maxilla: surgical movement and stability of rotational maxillary setback procedure. J Craniofac Surg 2009;20:2049-54.
9. Betts NJ, Edwards SP. Soft tissue changes associated with orthog- nathic surgery. In: Perterson’s Oral And Maxillofacial Surgery.
Vol. II, 2nd ed. Hamilton; BC Decker; 2004:1221-46.
10. Dann JJ 3rd, Fonseca RJ, Bell WH. Soft tissue changes associated with total maxillary advancement: a preliminary study. J Oral Surg 1976;34:19-23.
11. Schendel SA, Eisenfeld JH, Bell WH, Epker BN. Superior repositioning of the maxilla: stability and soft tissue osseous relations. Am J Orthod 1976;70:663-74.
12. Burstone CJ, James RB, Legan H, Murphy GA, Norton LA.
Cephalometrics for orthognathic surgery. J Oral Surg 1978;36:269- 77.
13. Legan HL, Burstone CJ. Soft tissue cephalometric analysis for orthognathic surgery. J Oral Surg 1980;38:744-51.
14. Radney LJ, Jacobs JD. Soft-tissue changes associated with surgical total maxillary intrusion. Am J Orthod 1981;80:191-212.
15. Mansour S, Burstone C, Legan H. An evaluation of soft-tissue changes resulting from Le Fort I maxillary surgery. Am J Orthod 1983;84:37-47.
16. O'Ryan F, Carlotti A. Nasal anatomy and maxillary surgery. III.
Surgical techniques for correction of nasal deformities in patients undergoing maxillary surgery. Int J Adult Orthodon Orthognath Surg 1989;4:157-74.
17. O'Ryan F, Schendel S. Nasal anatomy and maxillary surgery. II.
Unfavorable nasolabial esthetics following the Le Fort I osteotomy.
Int J Adult Orthodon Orthognath Surg 1989;4:75-84.
18. O'Ryan F, Schendel S. Nasal anatomy and maxillary surgery. I.
Esthetic and anatomic principles. Int J Adult Orthodon Orthognath Surg 1989;4:27-37.
19. Stella JP, Streater MR, Epker BN, Sinn DP. Predictability of upper lip soft tissue changes with maxillary advancement. J Oral Maxillofac Surg 1989;47:697-703.
20. Betts NJ, Fonseca RJ. Soft tissue changes associated with ortho- gnathic surgery. In: Bell WH, ed. Modern practice in orthognathic and reconstructive surgery, Volume III. Philadelphia: Saunders;
1992:2171-209.
21. Jensen AC, Sinclair PM, Wolford LM. Soft tissue changes associated with double jaw surgery. Am J Orthod Dentofacial Orthop 1992;101:266-75.
Dann
등10과Stella
등19은상악의악교정수술후에관련 연조직구조물이6
개월 후에 안정화된다고보고하였다.
그이후의많은연구들에서악교정수술후안정성 및연 조직변화를알아보는기간을 최소6
개월이상으로하고있다24-27,29,31,32
.
상악의이동에따른상응하는연조직을알아보고자하는연구에있어서수술에의한효과와술후교정 치료에의한효과를구분할필요가있다
.
골격성III
급부정 교합의악교정수술후에 특히상악의비발치교정치료를 하는경우술후III
급고무줄을적용하여상악전치의순측 회전이발생하여연조직의변화에영향을주는경우도있 다. Baek
등8에의한상악의Le Fort I
후상방회전움직임과하악의
BSSRO
후방이동후골격적인안정성을알아본연구에서
,
상악골에위치하는골격성계측점들은수술후1
주 일과수술후1
년을비교하였을때안정적이었지만상악제1
대구치근심협측교두정이나상악전치절단연과같은치 성계측점은수술후1
년에서수직,
수평적으로유의한재 발성변화가있었다고하였다.
이러한술후교정치료의상 순에의영향을최소한으로하기위해서본연구에서는수 술후평가기간을술후6
개월로설정하였다.
본 연구를통해서상악골의 시계방향의 회전움직임으 로상순비부의하방이동이이루어진다는 점을확인하였 고
,
상악전치의이동에대해서상순은높은비율의후방이동량을보인반면에
A' point
및Sn
등은유의한후방이동을 보이지 않았다
.
이전의 상악골의이동에 따른 비부와 상순의변화에대한연구들중9
명의환자를대상으로한Schouman
등35에의한연구에서는평균3.1 mm
의 상악골의후방이동으로
nasolabial angle
이평균8.9
o증가하였다고 하였고,
이는본연구결과에서상악전치의평균2.52 mm
후 방이동에의한nasolabial angle
이5.93
o증가한수치와상응 하는결과였다.
본연구에포함된 환자의수는통상적으로 만족할만한표본의수는아닌것으로생각되며,
보다많은표본수를대상으로할필요가있을것으로생각된다
. Lee
40는입술이얇을수록상악의이동에대해서보다예측가능 한상관관계를 보이고
,
두꺼울수록상관관계를 예측하기 힘들어진다고하였다.
이러한술후연조직변화에영향을 줄수있는요인들인연조직두께,
길이및기저근육및피 부의긴장도등과수술부위의봉합법등을고려하는것이 향후연구에서는필요할것이다.
V. 결 론
ANS
를회전중심으로하는상악골의후상방회전시행에따라서상순의후하방이동이 나타났다
. U1 tip
의이동에대해서
UL
은수평적으로는1 : 0.74,
수직적으로는1 : 0.83
의높은비율의상호관련성을보여주었다. Nasolabial angle
이증가되었고,
비첨부및비첨부하방부위비부는평균약1 mm
의하방이동양상이관찰되었다.
a longitudinal and long-term follow-up study. Eur J Orthod 2008;30:16-23.
32. Joss CU, Vassalli IM, Thuer UW. Stability of soft tissue profile after mandibular setback in sagittal split osteotomies: a longitu- dinal and long-term follow-up study. J Oral Maxillofac Surg 2008;66:1610-6.
33. Park JU, Hwang YS. Evaluation of the soft and hard tissue changes after anterior segmental osteotomy on the maxilla and mandible. J Oral Maxillofac Surg 2008;66:98-103.
34. Marsan G, Cura N, Emekli U. Soft and hard tissue changes after bimaxillary surgery in Turkish female Class III patients. J Craniomaxillofac Surg 2009;37:8-17.
35. Schouman T, Baralle MM, Ferri J. Facial morphology changes after total maxillary setback osteotomy. J Oral Maxillofac Surg 2010;68:1504-11.
36. Jacobson R, Sarver DM. The predictability of maxillary repositioning in LeFort I orthognathic surgery. Am J Orthod Dentofacial Orthop 2002;122:142-54.
37. Semaan S, Goonewardene MS. Accuracy of a LeFort I maxillary osteotomy. Angle Orthod 2005;75:964-73.
38. Robinson SW, Speidel TM, Isaacson RJ, Worms FW. Soft tissue profile change produced by reduction of mandibular prognathism.
Angle Orthod 1972;42:227-35.
39. Hershey HG, Smith LH. Soft-tissue profile change associated with surgical correction of the prognathic mandible. Am J Orthod 1974;65:483-502.
40. Lee JJ. Maxillary osteotomies: Le Fort I Osteotomy. In: Turvey TA, ed. Oral and Maxillofacial Surgery. Vol. III. 2nd ed. St. Louis:
Saunders; 2009:172-91.
22. Hack GA, de Mol van Otterloo JJ, Nanda R. Long-term stability and prediction of soft tissue changes after LeFort I surgery. Am J Orthod Dentofacial Orthop 1993;104:544-55.
23. Enacar A, Taner T, Toroğlu S. Analysis of soft tissue profile changes associated with mandibular setback and double-jaw surgeries. Int J Adult Orthodon Orthognath Surg 1999;14:27-35.
24. Park JO, Lee SC. A clinico-statistical study of soft tissue changes of upper lip & nose following Le Fort I maxillary movement. J Korean Assoc Maxillofac Plast Reconstr Surg 2000;22:310-8.
25. Mommaerts MY, Lippens F, Abeloos JV, Neyt LF. Nasal profile changes after maxillary impaction and advancement surgery. J Oral Maxillofac Surg 2000;58:470-5.
26. Koh CH, Chew MT. Predictability of soft tissue profile changes following bimaxillary surgery in skeletal class III Chinese patients.
J Oral Maxillofac Surg 2004;62:1505-9.
27. Chew MT. Soft and hard tissue changes after bimaxillary surgery in Chinese Class III patients. Angle Orthod 2005;75:959-63.
28. Jeong MH, Choi JH, Kim BH, Kim SG, Nahm DS. Soft tissue changes after double jaw rotation surgery in skeletal class III malocclusion. J Korean Assoc Oral Maxillofac Surg 2006;32:559- 65.
29. Chew MT, Sandham A, Wong HB. Evaluation of the linearity of soft- to hard-tissue movement after orthognathic surgery. Am J Orthod Dentofacial Orthop 2008;134:665-70.
30. Chung C, Lee Y, Park KH, Park SH, Park YC, Kim KH. Nasal changes after surgical correction of skeletal Class III malocclusion in Koreans. Angle Orthod 2008;78:427-32.
31. Joss CU, Thüer UW. Stability of the hard and soft tissue profile after mandibular advancement in sagittal split osteotomies: