접수일: 2013년 9월 10일, 게재승인일: 2013년 10월 18일 책임저자: 김동휘, 경기도 안산시 단원구 고잔1동
152-703, 고려대학교 안산병원 재활의학과
Tel: 031-412-5330, Fax: 031-412-4215 E-mail: [email protected]
당뇨병성 말초신경병증 환자에서 신경병성 통증의 치료
고려대학교 안산병원 재활의학과
김 동 휘
Treatment of Neuropathic Pain in Patients with Diabetic Peripheral Neuropathy
Dong Hwee Kim, M.D., Ph.D.
Department of Physical Medicine & Rehabilitation, College of Medicine, Korea University, Ansan, Korea
Neuropathic pain of diabetic peripheral neuropathy or pain- ful diabetic peripheral neuropathy is common problem, which is related with quality of life. Management of neuro- pathic pain in people with diabetic peripheral neuropathy is challenging to the practicing physician as it must be ad- justed to individual requirements based on the co-morbid- ities or other factors. This review is designed to present recommendation for treatment algorithm of painful diabetic peripheral neuropathy based on the clinical trials. (Clinical
Pain 2013;12:75-79)Key Words: Diabetic peripheral neuropathy, Painful, Treatment, Medication
서 론
당뇨병은 말초신경병증의 가장 흔한 원인이며, 유병기간 이 긴 당뇨병 환자의 50%에서 말초신경병증이 동반된다.1-3 당뇨병성 말초신경병증(diabetic peripheral neuropathy, DPN) 은 다양한 임상양상을 가진 이질적인 질환으로 원위부 양 측성 다발신경병증(distal symmetric polyneuropathy, DSPN), 단발신경병증(mononeuropathy), 당뇨병성근위축증(diabetic amyotrophy), 자율신경이상(autonomic dysfunction), 뇌신 경병증(cranial neuropathies), 포착신경병증(entrapment neu- ropathies) 등을 포함한다. Thomas4,5와 Boulton 등6,7은 당뇨 병성 신경병증(diabetic peripheral neuropathy, DPN)을 전 반적 형태(generalized variety)와 국소 및 다발(focal/multi- focal)신경병증으로 구분하였다. 2009년 19th annual Diabetic
Neuropathy Study Group of the European Association for the Study of Diabetes (NEURODIAB)와 8th International Symposium on Diabetic Neuropathy의 연합모임에서 전반 적 신경병증을 전형적인 당뇨병성말초신경병증(typical DPN) 과 비정형적 당뇨병성 말초신경병증(atypical DPN)으로 구 분하였다.8 또한 이 모임에서 통증성 당뇨병성말초신경병 증(painful DPN)에 대한 진단과 약물치료에 대한 검토가 이루어졌다. 본 논문은 당뇨병성신경병증에서 나타날 수 있는 신경병성 통증의 치료를 고찰하고자 한다.
본 론
당뇨환자에서의 신경병성 통증의 정의는 ‘당뇨병 환자에 서 체성감각신경계 이상의 직접적인 결과로 일어난 통증 (pain arising as a direct consequence of abnormalities in the somatosensory system in people with diabetes)’이다.9 당뇨환자들이 주로 호소하는 통증의 표현은 작열통(burning pain), 적격통증(shooting pain), 칼로베는 통증(lancinating pain)이며, 종종 양말이나 이불에 스칠 때 야기되는 접촉성 통증 즉 이질통(allodynia)을 경험하게 된다. 걸을 때 불편 감, 즉 ‘대리석을 맨발로 걷는 느낌(walking barefoot on mar- bles)’ 또는 ‘뜨거운 모래 위를 맨발로 걷는 느낌(walking barefoot on hot sand)’을 호소하며 발이 너무 뜨겁거나 차 갑다는 온도 인식에 대한 주관적 감각의 변화를 표현한다.
가끔 이런 증상들은 발부터 시작해서 하지의 상부로 진행 하여 하지 전체를 침범하기도 하고, 나중에는 상지까지 침 범하게 된다.9,10 당뇨병 환자에서 신경병성 통증은 특징적 으로 밤에 더 심하며 이로 인해 수면에 영향을 주게 된다.11 또한 낮 동안 통증은 일상생활동작 수행에 어려움을 일으 킬 수 있다. 통증의 증상들은 수년에 걸쳐 악화와 호전을 반복하다 감각소실이 악화될 때 궁극적으로 감소한다고 일 반적으로 믿어지고 있으나, 다른 연구들은 의미 있는 통증 의 감소가 일어나지 않는다고 한다.
신경병성 통증은 만성 원위부 양측성 다발신경병증을 가 진 당뇨병 환자에서 가장 흔하게 나타난다. 그러나 아주 드 물게 급성 통증성 당뇨병성 말초신경병증이 발생하며, 아 주 심한 감각증상이 있지만, 검사에서 신경학적 징후는 거 의 없다. 급성 통증성 당뇨병성 말초신경병증을 가진 환자
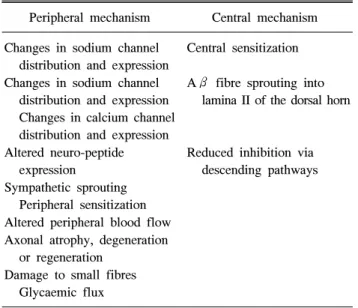
Table 1. Mechanisms of Neuropathic Pain16
Peripheral mechanism Central mechanism Changes in sodium channel
distribution and expression
Central sensitization Changes in sodium channel
distribution and expression Changes in calcium channel distribution and expression
Aβ fibre sprouting into lamina II of the dorsal horn
Altered neuro-peptide expression
Reduced inhibition via descending pathways Sympathetic sprouting
Peripheral sensitization Altered peripheral blood flow Axonal atrophy, degeneration
or regeneration Damage to small fibres
Glycaemic flux
Table 2. Definitions of Minimal Criteria for Distal Symmetric Polyneuropathy24 Confirmed Clinical DSPN
Symptoms or signs of DSPN. Symptoms may include: decreased sensation, positive neuropathic sensory symptoms (e.g. ‘asleep numbness’, ‘prickling’ or ‘stabbing’, ‘burning’ or ‘aching’ pain) predominantly in the toes, feet, or legs. Signs may include: sym- metric decrease of distal sensation or unequivocally decreased or absent ankle reflexes.
Confirmed Clinical DSPN
A combination of symptoms and signs of distal sensorimotor polyneuropathy with any two or more of the following: neuropathic symptoms, decreased distal sensation, or unequivocally decreased or absent ankle reflexes.
Confirmed Clinical DSPN
An abnormal nerve conduction study and a symptom or symptoms or a sign or signs of sensorimotor polyneuropathy. Severity of DSPN can be assessed by staged or continuous approaches described above and by dysfunction and disability scores Subclinical DSPN (Stage 1a)
No signs or symptoms of polyneuropathy. Abnormal nerve conduction, as described above, is present 의 공통된 증상들은 아주 심한 통증이고, 그 외에 체중감소,
우울증이 나타날 수 있으며, 남자의 경우 발기부전이 동반 될 수 있다.10,12 이런 증상은 혈당의 급격한 조절(insulin neuritis)이나 제1형 당뇨병 환자에서 혈당 조절이 잘 되지 않는 경우(diabetic ketoacidosis)에 발생할 수 있다.10,12 보 통 급성 통증성 당뇨병성 말초신경병증의 예후는 좋은 것 으로 알려져 있으며, 발생 후 1년 안에 모든 증상들이 완전 히 소실된다.10,13
1. 역학
당뇨병성 말초신경병증에 대한 역학이나 위험요인들은 연구가 많이 되었지만, 통증의 유병률을 특별하게 본 연구 는 드물며, 통증의 유병률은 10-26%로 알려져 있다.14,15 영 국에서 한 인구 모집단 연구에서 구조화된 설문지와 진찰
을 통해 통증을 평가하였을 때 급성 통증성 당뇨병성 말초 신경병증의 유병률은 16%이었다. 그러나 이 환자들 중 12.5%는 한번도 의사에게 자신의 통증을 보고하지 않았고, 39%는 자신들의 통증에 대해 치료를 받아 본 적이 없다고 하였다.15
2. 당뇨병 환자에서 신경병성 통증의 기전
통증성 당뇨병성 말초신경병증에 대한 신경-구조 관련성 (neuro-structural correlates)을 포함한 여러 기전들이 제안 되기는 하지만(Table 1),16 아직까지는 당뇨병 환자에서 신 경병성 통증의 정확한 병리생리학적 기전은 수수께끼로 남 아있다. 그 외 잠재적인 기전으로는 혈중 포도당 수치의 불 안성과의 관련, 말초신경의 신경외막 내 혈류 증가, 족부 피부내 미세혈류의 변화, 피하내 신경섬유 밀도 감소, 자율 신경 이상 등이 있다.17-22
3. 당뇨병 환자에서 신경병성 통증의 평가 및 진단
Boulton 등은 통증성 당뇨병성 말초신경병증의 진단은 환자의 통증에 대한 표현에 기초한 임상진단이며,23 전기진 단검사와 정량적 감각검사를 통해 보완될 수 있고, 통증의 다른 원인, 예를 들어 포착신경병증과 같은 동반질환을 감 별하는데 중요하다고 하였다. 그러나 19th annual Diabetic Neuropathy Study Group of the European Association for the Study of Diabetes (NEURODIAB)와 8th International Symposium on Diabetic Neuropathy의 연합 모임에서 전형 적인 당뇨병성 말초신경병증인 원위부 양측성 말초신경병 증의 진단을 위한 최소 기준의 정의를 정하였다(Table 2).24 이 기준에서는 환자의 증상 및 징후 뿐 아니라 신경전도검 사가 confirmed clinical DSPN과 subclinical DSPN의 진단 에 중요한 역할을 한다.24
당뇨병성 말초신경병증의 진단은 제외의 진단이기 때문 에 자세한 임상병력과 하지의 말초 신경 및 혈관에 대한
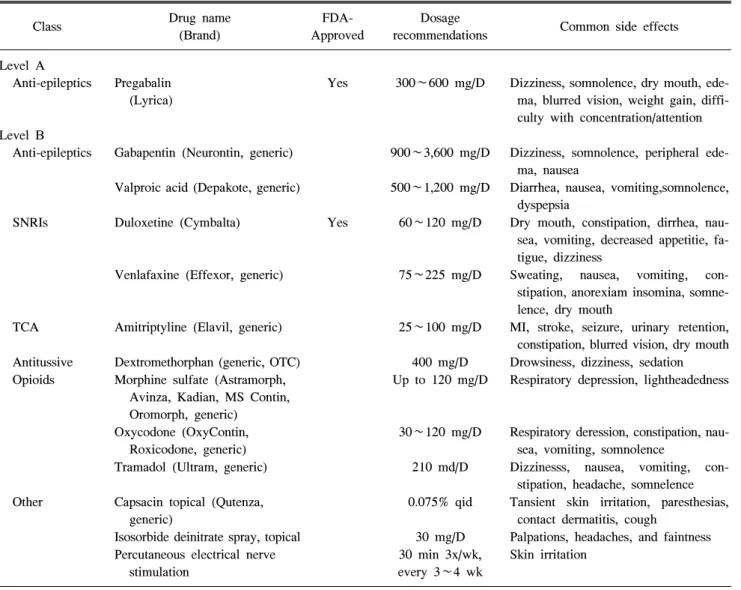
Table 3. Evidence-based Treatment of Painful Diabetic Neuropathy8
Class Drug name
(Brand)
FDA- Approved
Dosage
recommendations Common side effects Level A
Anti-epileptics Pregabalin (Lyrica)
Yes 300∼600 mg/D Dizziness, somnolence, dry mouth, ede- ma, blurred vision, weight gain, diffi- culty with concentration/attention Level B
Anti-epileptics Gabapentin (Neurontin, generic) 900∼3,600 mg/D Dizziness, somnolence, peripheral ede- ma, nausea
Valproic acid (Depakote, generic) 500∼1,200 mg/D Diarrhea, nausea, vomiting,somnolence, dyspepsia
SNRIs Duloxetine (Cymbalta) Yes 60∼120 mg/D Dry mouth, constipation, dirrhea, nau- sea, vomiting, decreased appetitie, fa- tigue, dizziness
Venlafaxine (Effexor, generic) 75∼225 mg/D Sweating, nausea, vomiting, con- stipation, anorexiam insomina, somne- lence, dry mouth
TCA Amitriptyline (Elavil, generic) 25∼100 mg/D MI, stroke, seizure, urinary retention, constipation, blurred vision, dry mouth Antitussive Dextromethorphan (generic, OTC) 400 mg/D Drowsiness, dizziness, sedation Opioids Morphine sulfate (Astramorph,
Avinza, Kadian, MS Contin, Oromorph, generic)
Up to 120 mg/D Respiratory depression, lightheadedness
Oxycodone (OxyContin, Roxicodone, generic)
30∼120 mg/D Respiratory deression, constipation, nau- sea, vomiting, somnolence
Tramadol (Ultram, generic) 210 md/D Dizzinesss, nausea, vomiting, con- stipation, headache, somnelence Other Capsacin topical (Qutenza,
generic)
0.075% qid Tansient skin irritation, paresthesias, contact dermatitis, cough
Isosorbide deinitrate spray, topical 30 mg/D Palpations, headaches, and faintness Percutaneous electrical nerve
stimulation
30 min 3x/wk, every 3∼4 wk
Skin irritation
Adapted from Guidelines from American Academy of Neurology, the American Association of Neuromuscular and Electrodiagnostic Medicine, and the American Academy of Physical Medicine and Rehabilitation. Based on reference 20. MI: myocardial infarction, OTC: over-the-counter, qid: 4 times daily, SNRIs: serotonin norepinephrine reuptake inhibitor, TCA: tricyclic antidepressant.
진찰을 통해 신경병성 통증을 일으킬 수 있는 다른 질환들 을 제외하는 것이 중요하다. 통증성 당뇨병성 말초신경병 증은 양측성이기 때문에 편측성 증상이나 징후를 보이는 경우 다른 원인이 있는지 찾아야 한다.
통증의 정도는 단순하게 평가할 수 있는 시각통증등급 (visual analogue scale)이나 numerical rating scale (an 11-point Likert scale)을 사용한다. 삶의 질도 평가하는데, NeuroQol, Norfolk Quality of Life Scale, Neuropathic Pain Impact on Quality-of-Life Questionnaire (NePIQoL) 등을 이용한다.
4. 당뇨병 환자에서 신경병성 통증의 치료
당뇨병 환자에서 신경병성 통증의 평가와 치료는 임상의 에게는 쉽지 않고, 신경병성 통증의 영향이 다양하고 다각 적이기 때문에 감정이입 및 다학제적 접근(an empathic &
multi-disciplinary approach)가 중요하다. 신경병성 통증과 잘 조절되지 않는 혈당과 관련이 있다는 여러 연구들을 고 려할 때, 어떤 형태의 당뇨병성 말초신경병증이든, 우선적 과정은 혈당 조절이라는 것에는 전반적으로 동의한다. 또 한 고혈압이나 고지혈증과 같은 대혈관 질환의 다른 위험 인자들이 당뇨병성 말초신경병증에서 흔하기 때문에 이런 인자들을 조절하는 것은 중요하다.
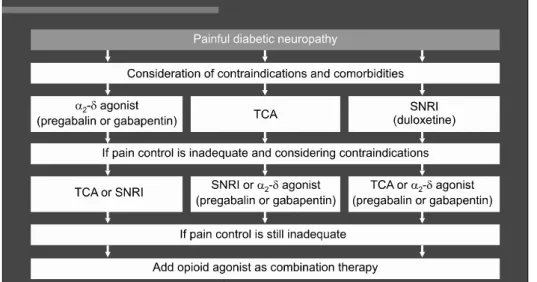
Fig. 1. Treatment algorithm for painful diabetic peripheral neuro- pathy.26
5. 당뇨병 환자에서 신경병성 통증의 약물치료 미국의 FDA와 European Medicines Agency에 의해 당 뇨병 환자에서의 신경병성 통증에 인정된 약물은 dulox- etine과 pregabalin 두 가지뿐이다. 2011년 American Aca- demy of Neurology, the American Association of Neuromus- cular and Electrodiagnostic Medicine, and the American Academy of Physical Medicine and Rehabilitation에서는 통증성 당뇨병성 신경병증의 치료에 대한 근거중심 가이드 라인을 통해 신경병성 통증에 효과가 있는 것으로 알려진 약물적 치료와 비약물적 치료를 제시하였다(Table 3).8 이 중 level A 강도로 추천된 것은 pregabalin이며, 비약물적 치료 중에는 level B의 강도로 경피적 전기신경자극(percu- taneous electrical nerve stimulation)이 추전되었다. 그러나 level B의 강도로 사용하지 않도록 추천된 치료에는 oxcar- bazepine, lamotrigine, lacosamide, clonidine, pentoxifylline, mexiletine, 자기장 치료(magnetic field treatment), 저출력 레이저 치료(low-intensity laser therapy), Reiki therapy 등 이 있다. 철저한 혈당조절을 제외하고는 Table 3에 제시된 약물치료로 신경섬유의 점진적 소실에 이르게 하는 당뇨병 성 말초신경병증의 자연적 경과에 영향을 미치지 않는다.
여러 disease-modifying agents이 연구되고 있지만, 하나 의 메타분석 연구에 의해 그 효과가 인정되고 있는 것은 항산화제(anti-oxidant)인 α-lipoic acid이다. 3주 동안 하루 에 한번 600 mg을 정맥 내 주사한 경우 신경병성 통증의 감소에 효과가 있었으며,25 구강투여 제재에 대한 결과는 현재 기다리고 있는 중이다.
6. 치료 알고리듬에 대한 제안
당뇨병 환자에서 신경병성 통증에 대한 다양한 약물에 대한 임상연구를 기초로 Fig. 1과 같은 algorithm이 제안되 었다.26 Table 3의 약물들의 상대적 효용과 안정성을 고려 할 때, 삼환계 항우울제, selective norephrine reuptake in- hibitor (SNRI, duloxetine), 항전간제(pregabalin)이 일차약 으로 고려되어져야만 한다. 일차약으로 통증이 적절하게 조절되지 않는다면 금기 적응증을 기초로 다른 약들이 고 려되어질 수 있다. 일차약을 바꾸었는데도 통증 조절이 되 지 않는 경우 일차약들의 병합요법을 사용하고, 그래도 통 증 조절이 이루어지지 않으면, tramadol이나 oxycodone과 같은 마약 계통의 약을 추가할 수 있다. 그러나 2010년 영 국의 National Institute for Health and Clinical Excellence 에서 제안한 당뇨병 환자에서 신경병성 통증의 약물치료에 대한 알고리듬에서는 일차약으로 삼환계 항우울제와 SNRI 을 제안하였고, 일차약으로 통증 조절이 되지 않는 경우 pregabalin으로 바꾸거나 추가하도록 제안하였다.27
결 론
신경병성 통증은 당뇨병 환자들의 약 1/4까지 영향을 줄 수 있는 중요한 임상문제이며, 삶의 질의 저하를 야기하지 만, 덜 진단되고 덜 치료되고 있다. 이런 상황은 변화되어야 하며 당뇨병 환자들에서 신경병성 통증을 진단하기 위한 최소한의 요구조건인 증상에 대한 평가와 신경학적 진찰이 이루어져야 한다. 통증의 다른 원인들이 제외되어야만 하 고 각각의 약에 대한 금기사항이 있는지 확인해야만 한다.
적절한 혈당 조절, 심혈관계 위험인자에 대한 적극적인 치 료와 함께 신경병성 통증에 효과가 있는 것으로 증명된 약 물들(삼환계 항우울제, selective norephrine reuptake in- hibitor, 항전간제)을 단독 또는 복합요법을 통해 적절하게 통증을 관리해야 한다.
참 고 문 헌
1. Boulton AJM, Malik RA, Arezzo J, Sosenko JM. Diabetic somatic neuropathies. Diabetes Care 2004; 27: 1458-1486 2. Soedamah-Muthu SS, Chaturvedi N, Witte DR, Stevens
LK, Porta M, Fuller JH; EURODIAB Prospective Complica- tions Study Group. Relationship between risk factors and mortality in type 1 diabetic patients in Europe: the EURODIAB Prospective Complications Study (PCS).
Diabetes Care 2008; 31: 1360-1366
3. Carrington AL, Shaw JE, Van Schie CMH, Abbott CA, Vileikyte L, Boulton AJM. Can motor nerve conduction ve- locity predict foot problems in diabetic subjects over a 6-year outcome period? Diabetes Care 2002; 25: 2010-2015 4. Thomas PK. Classification, differential diagnosis and stag- ing of diabetic peripheral neuropathy. Diabetes 1997; 46:
S54-S57
5. Thomas PK. Classification of the diabetic neuropathies. In Textbook of Diabetic Neuropathy, Arnold Gries G, Cameron NE, Low PA, Ziegler D (eds). Thieme: Stuttgart, 2003;
175-177
6. Boulton AJM, Malik RA, Arezzo JC, Sosenko JM. Diabetic somatic neuropathies. Diabetes Care 2004; 27: 1458-1486 7. Boulton AJ, Vinik AI, Arezzo JC, et al. Diabetic neuro- pathies: a statement by the American Diabetes Association.
Diabetes Care 2005; 28: 956-962
8. Bril VB, England J, Franklin GM, et al. Evidence-based guideline: Treatment of painful diabetic neuropathy.
Neurology 2010; 76: 1758-1765
9. Treede R-D, Jensen TS, Campbell JN, et al. Neuropathic pain: redefinition and a grading system for clinical and re- search purposes. Neurology 2008; 70: 1630-1635 10. Boulton AJM, Malik RA, Arezzo J, Sosenko JM. Diabetic
somatic neuropathies. Diabetes Care 2004; 27: 1458-1486 11. Zelman DC, Brandenburg NA, Gore M. Sleep impairment
in patients with painful diabetic peripheral neuropathy. Clin J Pain 2006; 22: 681-685
12. Tesfaye S, Malik RA, Harris N, et al. Arterio-venous shunt- ing and proliferating new vessels in acute painful neuro- pathy and rapid glycaemic control (insulin neuritis).
Diabetologia 1996; 39: 329-335
13. Vinik A. The approach to the management of the patient with neuropathic pain. J Clin Endocrinol Metab 2010; 95:
4802-4811
14. Tesfaye S, Boulton AJM (eds). Diabetic Neuropathy.
Oxford: Oxford University Press: 2009.
15. Daousi C, McFarlane IA, Woodward A, Nurmikko TJ, Bendred PE, Benbow SJ. Chronic painful peripheral neuro- pathy in an urban community: a control comparison of peo- ple with and without diabetes. Diabet Med 2004; 21: 976-982 16. Tesfaye S, Kempler P. Painful diabetic neuropathy. Diabeto-
logia 2005; 48: 805-807
17. Oyibo SO, Prasad YDM, Jackson NJ, Boulton AJM. The relationship between blood glucose excursions and painful diabetic peripheral neuropathy: a pilot study. Diabet Med 2002; 19: 870-873
18. Eaton SE, Harris ND, Ibrahim S, et al. Differences insural nerve haemodynamics in painful and painless neuropathy.
Diabetologia 2003; 934-939
19. Quattrini C, Harris ND, Malik RA, Tesfaye S. Impaired skin microvascular reactivity in painful diabetic neuropathy.
Diabetes Care 2007; 30: 655-659
20. Sorensen L, Molyneaux L, Yue DK. The relationship among pain, sensory loss, and small nerve fibers in diabetes.
Diabetes Care 2006; 29: 883-887
21. Selvarajah D, Wilkinson ID, Gandhi R, Griffiths PD, Tesfaye S. Microvascular perfusion abnormalities of the Thalamus in painful but not painless diabetic polyneuropathy: a clue to the pathogenesis of pain in type 1 diabetes. Diabetes Care 2011; 34: 718-720
22. Gandhi R, Marques JLB, Selvarajah D, et al. Painful dia- betic neuropathy is associated with greater autonomic dys- function than painless diabetic neuropathy. Diabetes Care 2010; 33: 1585-1590
23. Boulton AJM, Vinik AI, Arezzo JC, et al. Diabetes neuro- pathies: a statement by the American Diabetes Association.
Diabetes Care 2005; 28: 1-7
24. Tesfaye S, Boulton AJM, Dyck PJ, et al. Diabetic neuro- pathies: update on definitions, diagnostic criteria, estima- tion of severity and treatments. Diabetes Care 2010; 33:
2285-2293
25. Ziegler D, Nowak H, Kempler P, Vargha P, Low PA. Treat- ment of symptomatic diabetic polyneuropathy with al- pha-lipoic acid: a meta-analysis. Diabetic Med 2004; 21:
114-121
26. Tesfaye S, Vileikyte L, Rayman G, et al. Painful diabetic peripheral neuropathy: consensus recommendations on di- agnosis, assessment and management. Diabetes Metab Res Rev 2011; 27: 629-638
27. Centre for Clinical Practice at NICE (UK). Neuropathic Pain: The Pharmacological Management of Neuropathic Pain in Adults in Non-Specialist Settings. London: National Institute for Health and Clinical Excellence (UK); 2010 Mar