저작자표시-비영리-변경금지 2.0 대한민국 이용자는 아래의 조건을 따르는 경우에 한하여 자유롭게 l 이 저작물을 복제, 배포, 전송, 전시, 공연 및 방송할 수 있습니다. 다음과 같은 조건을 따라야 합니다: l 귀하는, 이 저작물의 재이용이나 배포의 경우, 이 저작물에 적용된 이용허락조건 을 명확하게 나타내어야 합니다. l 저작권자로부터 별도의 허가를 받으면 이러한 조건들은 적용되지 않습니다. 저작권법에 따른 이용자의 권리는 위의 내용에 의하여 영향을 받지 않습니다. 이것은 이용허락규약(Legal Code)을 이해하기 쉽게 요약한 것입니다. Disclaimer 저작자표시. 귀하는 원저작자를 표시하여야 합니다. 비영리. 귀하는 이 저작물을 영리 목적으로 이용할 수 없습니다. 변경금지. 귀하는 이 저작물을 개작, 변형 또는 가공할 수 없습니다.
Master’s Thesis in
Medical Science
Inter-observer Agreement of Major
and Ancillary imaging Features for
Diagnosis of HCC in LI-RADS
Lexicon by using Gadoxetic-acid
enhanced MR imaging
Ajou University Graduate School
Medical Science Major
Inter-observer Agreement of Major
and Ancillary imaging Features for
Diagnosis of HCC in LI-RADS
Lexicon by using Gadoxetic-acid
enhanced MR imaging
Jei Hee Lee, M.D., Ph.D., Advisor
I submit this thesis as the
Master
’s thesis in Medical Science.
August, 2017
Ajou University Graduate School
Medical Science Major
The Master's thesis of Seulgi Yoll in Medical Science is
hereby approved.
Thesis Defense CoⅡ 1Inittee President
브 츠노
뢰 ∠
墅
촬
外
,'—
Member
Member
⇒ ι 닌 노ι τ
p낭¼
ν\
f'
Aㅂ
ou IJniversity Graduate Schoo1
i ABSTRACT
Inter-observer Agreement of Major and Ancillary imaging
Features for Diagnosis of HCC in LI-RADS Lexicon by using
Gadoxetic-acid enhanced MR imaging
Objectives: To assess the inter-observer agreement of imaging features of LI-RADS using
contrast-enhanced CT (CECT) and gadoxetic-acid enhanced MR (GAeMR) between expert and novice radiologists
Materials and Methods: From January 2013 to December 2015, sixty-three patients
(M:F=54:9, mean age: 55.8±9.5 years) which were confirmed with HCC pathologically and undergoing CECT and GAeMR were included in this study. Two abdominal special radiologists analyzed CT and MR images with consensus and other two novice radiologists analyzed CT and MR images with consensus. The size of the tumor, which is an important diagnostic criterion in the LI-RADS lexicon, was compared to the pathologically measured size to assess the measurement error in each imaging modality and in each phase. We also evaluated inter-observer agreement between the readers of arterial hyperenhancement, washout, and capsule appearance, which are the major imaging findings of LI-RADS in HCC. In addition, inter-observer agreement of final LI-RADS categorization was evaluated.
Results: A total of 63 patients were included in the study. When comparing the difference
between the measured value of each tumor and the size of pathologically measured tumor as a reference value, it was confirmed that the measurement error was smaller than that of CT by MRI. However, there was no statistical difference in the measurement error between expert radiologists and novice radiologists (p=0.29, p=0.62). When we assessed the inter-observer agreement of the HCC imaging features of LI-RADS, the arterial hyperenhancement was moderate in both CT and MR (к=0.566, 0.475). Inter-observer agreement on washout appearance was fair in CT (к= 0.364) and substantial in MR (к =0.630). In the case of capsule appearance, inter-observer agreement was moderate in CT
ii
(к=0.491) and fair in MR (к=0.303). There was no significant difference in the proportion of the LI-RADS category between experts and novices. When evaluating the value of intraclass correlation coefficients (ICC), it was found that the inter-reader agreement of MR was lower than that of CT (ICC = 0.574 in CT, 0.318 in MR).
Conclusion: MR was slightly more accurate than CT in measuring the size of HCC,
especially for beginners. Inter-reader agreement was higher in CT than MR in arterial hyperenhancement and capsule appearance, whereas in terms of washout appearance, that was higher in MR than in CT. LI-RADS showed fair to moderate agreement for diagnosis of HCC on CT and GAeMR.
iii
TABLE OF CONTENTS
ABSTRACT ··· i
TABLE OF CONTENTS ··· iii
LIST OF FIGURES ··· iv
LIST OF TABLES ··· v
I. INTRODUCTION ··· 1
II. MATERIALS AND METHODS ··· 3
A. Patients selection ··· 3 B. Image Acquisition ··· 3 C. Image Analysis ··· 4 D. Statistical Analysis ··· 5 III. RESULTS ··· 7 A. Turmor size ··· 7
B. Major Imaging Features ··· 7
C. Ancillary Imaging Features ··· 8
D. LI-RADS Categorization ··· 8
IV. DISCUSSION ··· 14
V. CONCLUSION ··· 18
REFERENCES ··· 19
iv
LIST OF FIGURES
Figure 1. Image from a 36- year-old man with hepatocellular carcinoma (HCC) in
segment VII of the liver ··· 12
v
LIST OF TABLES
Table 1. MR Imaging Sequences and Parameters ··· 9
Table 2. Measurement errors of hepatocellular carcinomas (HCCs) size measured
by novice and experts ··· 10
Table 3. Inter-observer agreement of LI-RADS major imaging features by CT and
1
I. INTRODUCTION
Hepatocellular carcinoma (HCC) is the sixth most common cancer and the third most common cause of death from cancer worldwide.(1) Early diagnosis of hepatic cancer is important as it can lead to early intervention with curative intent resulting in improved patients’ prognosis.
Noninvasive imaging-based diagnosis of HCC is widely accepted in patients with chronic liver disease. The classic criteria include arterial hyperenhancement, washout appearance and pseudocapsule. This is due to unique feature of HCC, which reflects the development of anomalous arterial vascularization and decreased portal venous supply.(2)
Up to now, findings of liver imaging have been interpreted and recorded inconsistently between radiologists. In this background, the Liver Imaging Reporting and Data System (LI-RADS) has been developed for computed tomography (CT) and magnetic resonance (MR) imaging of the liver in patients undergoing HCC surveillance.(2) LI-RADS provides standardized reporting system of imaging findings and assigns imaging findings to one of five categories. The aim of LI-RADS is to reduce variability in lesion interpretation, to improve communication with clinicians, and to facilitate decision making processes, outcome monitoring, performance auditing, quality assurance and research.3 Imaging features that favor HCC in LI-RADS lexicon include major imaging features (arterial phase hyperenhancement, portal venous or later phase washout, capsular appearance, threshold growth) and other ancillary imaging features.(3)
Gadoxetic acid disodium (gadolinium ethoxybenzyl diethylenetriaminepentaacetic acid; Eovist and Primovist, Bayer Healthcare Pharmaceuticals, Berlin, Germany), which has the properties of both extracellular and hepatocyte-specific contrast agents, enables both dynamic and hepatobiliary phase (HBP) imaging.(4, 5) Gadoxetic acid-enhanced MR (GAeMR) imaging
2
shows higher sensitivity for HCC detection, especially for small nodules compared with other imaging modalities.(6, 7)
Previous studies have shown high inter-observer reliability in the overall grading of lesions using LI-RADS and other criteria.(8) Several studies reported that high inter-reader agreement in assessing arterial hyperenhancement and moderate inter-reader agreement in assessing the washout or capsular appearance.(8, 9)
Numerous methods have been applied to define the longest diameter of a tumor, including sonography, CT, and MR imaging and the size of HCC may differ according to the imaging modality.(10) Furthermore, even practical guidelines do not clarify the measurement method for tumor size.(11) And substantial discordance between CT and MR for stratification of hepatic nodules using LI-RADS has been reported.(12)
However, inter-reader agreement of imaging features of LI-RADS at CT and GAeMR has not been known yet.
So, the purpose of this study was to determine for expert and novice readers the inter-observer agreement of imaging features of LI-RADS using contrast-enhanced CT and GAeMR.
3
II. MATERIALS AND METHODS
A. Patients Selection
The institutional review board of our hospital approved this study and waived the requirement of informed consent because of the retrospective nature of the study and its use of data from anonymous images. Patients who underwent GAeMR and dynamic CT between Jan 2013 and Dec 2015 were included for analysis.
We include one largest HCC per patient to avoid a cluster effect in the statistical analysis, and patients who had undergone preoperative transarterial chemoembolization, hepatic arterial infusion chemotherapy, and systemic chemotherapy were excluded although the lesions show typical enhancement of HCC.
B. Image Acquisition
Multidetector CT (MDCT) was performed by using one of the following CT scanners: Sensation 16 (Siemens Healthcare, Forchheim, Germany) (n=10), SOMATOM Definition Flash (Siemens Healthcare, Forchheim, Germany) (n=22), Brillance 16 (Philips Healthcare, Cleveland, Ohio, USA) (n=11), or Brillance 64 (Philips Healthcare, Cleveland, Ohio, USA) (n=20).
Unenhanced CT scans were obtained before contrast media injection. A total of 120 mL to 150 mL of a nonionic contrast material (iohexol, Omnipaque 300, Nycomed, Princeton, NJ, USA or iopromide, Ultravist 300; Schering, Berlin, Germany) was injected into an antecubital vein through an 18-gauge plastic intravenous catheter. Hepatic arterial phases (AP) were obtained with a scan delay of 18 seconds after the Hounsfield unit (HU) of the abdominal aorta reached 100 HU with a power injector at a rate of 3 ml/s. Thirty seconds after the hepatic AP
4
(about 75–85 seconds after injection of the contrast agent), scans for the portal venous phase (PVP) were acquired. Delayed phase (DP) images were acquired 100 seconds (about 180-190 seconds after injection of the contrast agent) after the end of the acquisition of the PVP. CT scans were obtained at a tube current-time product of 150-200 mAs and a peak voltage of 120 kVp. Whole-liver scanning was completed in 4–8 seconds while the patients held their breath. Images were reconstructed with a 5-mm slice thickness using raw imaging data with a standard reconstruction algorithm.
All of the MR studies were performed with a 1.5-T system (Signa HDxt; GE Healthcare, Milwaukee, Wisconsin, United States) with phased array coils. All of the images were obtained on the axial plane. The field of view (40 cm × 32-40 cm) was adjusted for each patient. The MR protocol consisted of a dual-echo T1-weighted gradient-echo sequence (in-phase and opposed-phase), a respiratory-triggered fast spin T2-weighted sequence, and a contrast-enhanced dynamic sequence using a T1-weighted 3D gradient-echo sequence with fat-suppression. The parameters for all of the sequences are presented in Table 1. For the contrast-enhanced dynamic and HBP MR images, gadoxetic acid disodium was administered at 0.025 mmol per kilogram of body weight at 1 mL per second, followed by a 20-mL saline flush. After administering the contrast, AP (25-30 sec), PVP (60 sec), and additional HBP (after 20 min) images were obtained.
C. Image Analysis
Preoperative contrast enhanced liver CT and GAeMR images were analyzed retrospectively on a picture archiving and communication system (Infinitt PACS, version 3.0; Infinitt Healthcare, Seoul, Korea).
Two board-certified abdominal radiologists (J.H.L., B.K., 20 and 8 years of experience, respectively) evaluated the CT and MR images as well as the lesion size and segmental location as noted in the pathology report in consensus. In cases
5
where identifying lesions of the correct size and location was difficult, or the two readers disagreed on lesion location, lesions were excluded from further analysis. For this study, two novice radiology residents (S.Y, P.S.S) at the same center interpreted CT and MR examinations. Before the beginning of the study, readers were provided 1 hour of lecture-based and hands-on instruction that explained LI-RADS definitions in detail.
All readers were aware that patients had undergone liver surgery and that the pathologic reports confirmed HCC but they were blinded to all other clinical, laboratory, and pathologic details.
Each reader measured the size of each lesion on multiphasic images on CT (unenhanced, AP, PVP, and DP) and MRI (unenhanced, AP, PVP, and HBP). Each reader was asked to measure the longest diameter of the HCC for each phase/sequence. Average values of measured longest diameter by two novices and experts were used for statistical analysis. We regarded gross pathological size of the HCC as reference standard.
Each lesion was then assessed in terms of AP hyperenhancement, the presence or absence of washout and capsule appearance. According the LI-RADS lexicon v2014, washout was defined as a temporal reduction in enhancement relative to liver in the PVP on GAeMR.
In cases of disagreement between the two readers, images were re-reviewed and a consensus categorization was performed. Each lesion was then assigned a LI-RADS category based on the v2014 guidelines.
D. Statistical Analysis
Statistical evaluations were performed using MedCalc Statistical Software version 17.5.5 (MedCalc Software bvba, Ostend, Belgium; http://www.medcalc.org; 2017). Significant differences were defined as those with P< 0.05.
6
Numeric data were presented as an average and standard deviation. Inter-observer agreement of categorical data was evaluated using Cohen’s kappa statistic. Intraclass correlation coefficients and 95% confidence intervals (CIs) were used to assess the inter-reader agreement and intraclass correlation coefficients (ICC) was calculated.
Regarding gross pathologic diameter of HCC as standard reference, differences of the diameter of the HCCs measured by novice readers and expert readers were tested by using repeated measures analysis of variance (ANOVA). A two-way repeated-measures ANOVA was used to detect the bias of parameter estimates across the each phases, imaging modalities, and observers.
A Fisher’s exact test was used to compare the proportion of lesions demonstrating AP hyperenhancement, washout, and capsule appearance as well as rates of LI-RADS category with CT and MRI. κ results were stratified qualitatively by score (slight agreement, 0.01–0.20;fair agreement, 0.21–0.40; moderate agreement, 0.41–0.60; substantial agreement, 0.61–0.80; almost perfect agreement, 0.81–0.99).
7
III. RESULTS
Total 63 patients (M:F = 54:9, mean age 55.8±9.5 years) were included in this study. Patients were pathologically confirmed HCCs after surgical resection wedge resection: 19, segmentectomy: 15, sectionectomy: 14, hemihepatectomy: 13, extended hemihepatectomy: 1, total hepatectomy: 1). The underlying causes of cirrhosis (as determined from available pathological/laboratory data and hepatology clinical notes) included viral hepatitis B (n=52), viral hepatitis C (n=3), and alcohol abuse (n=8).
A. Tumor Size
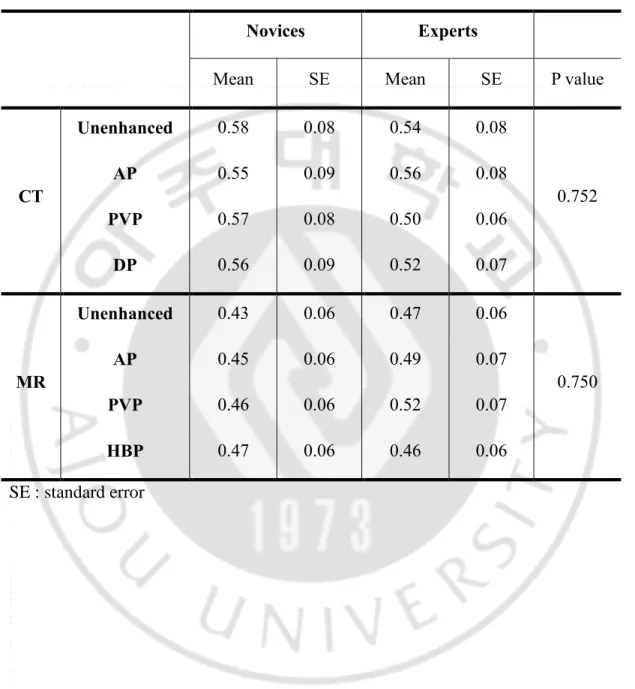
Mean tumor size was 3.4± 2.4cm [1.0-14.0] on basis of the pathologic reports. Regarding gross pathologic diameter as standard reference, the mean and standard error of the measurement error of tumor measured on each phase/sequence by novices and experts are summarized in Table 2. There were no statistical significances on the measurement errors in each CT phases by novice or experts with ANOVA. The measurement errors on MR were slightly smaller than CT, but there were no statistical significances by novices (P=0.29) or experts (P=0.62). There were no statistical significances on the measurement errors in each MR phases by novices or experts.
B. Major Imaging Features
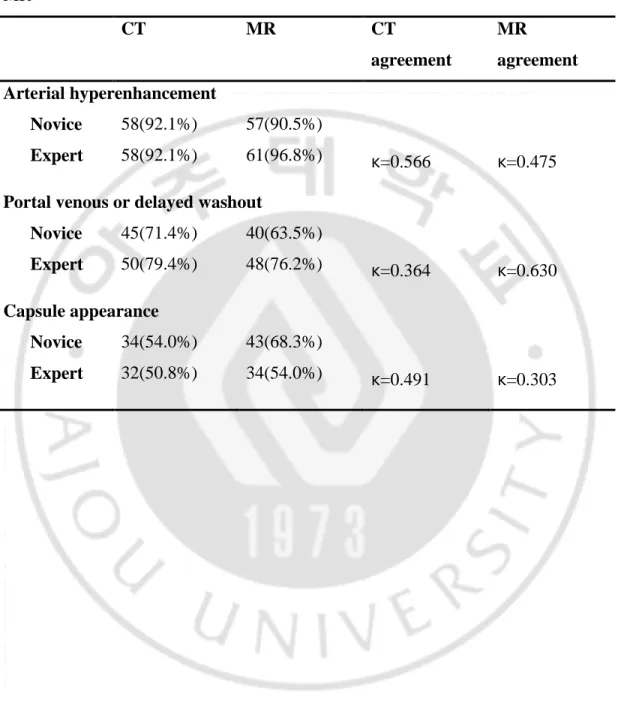
Table 3 shows the frequency of LI-RADS major imaging features and inter-observer agreement. Inter-observer agreement on AP hyperenhancement was moderate in CT and MR (к=0.566, 0.475). Inter-observer agreement on washout
8
appearance was fair in CT (к= 0.364) and substantial in MR (к=0.630). Inter-observer agreement on capsule appearance was moderate in CT (к=0.491) and fair in MR (к=0.303).
C. Ancillary Imaging Features
In only two cases, novice used ancillary imaging feature from LI-RADS 3 lesions to LI-RADS 4 lesions on CT. There was no case in expert’s reading used ancillary imaging feature on CT. In two cases on MR, novice used ancillary imaging features from LI-RADS 3 lesions to LI-RADS 4 lesions. In only one case on MR, expert used ancillary imaging features from RADS 3 lesion to LI-RADS 4 lesion.
D. LI-RADS Categorization
Figure 2 shows the distribution of LI-RADS category in each reader. ICC for LI-RADS category in CT between individual readers was 0.574 with 95% CI of [0.393, 0.755]. ICC for LI-RADS category in MR between individual readers was 0.318 with 95% CI of [0.098, 0.537]. Overall inter-observer agreement was better when measured by CT than by MR.
9 Table 1. MR Imaging Sequences and Parameters
Parameters TR/TE (msec) Flip angle (degree) Section thickness (mm) Intersection
gap (mm) Matrix size
Reduction factor
Double-echo T1-weighted gradient echo Single shot heavily T2 wieghted
Respiratory-triggered fast-spin T2-weighted T1-weighted 3D Gradient echo
6.2 / 2.0–4.1 900-1100 / 160 7000-8000 / 84 4.2 / 2.0 12 90 90 12 2.5 7 7 2.5 0 1 1 0 288 x 192 380 x 380 320 x 224 361 x 380 1.74 2 1 1.73
10
Table 2. Measurement errors of hepatocellular carcinomas (HCCs) size measured
by novice and experts
Novices Experts
Mean SE Mean SE P value
CT Unenhanced 0.58 0.08 0.54 0.08 0.752 AP 0.55 0.09 0.56 0.08 PVP 0.57 0.08 0.50 0.06 DP 0.56 0.09 0.52 0.07 MR Unenhanced 0.43 0.06 0.47 0.06 0.750 AP 0.45 0.06 0.49 0.07 PVP 0.46 0.06 0.52 0.07 HBP 0.47 0.06 0.46 0.06 SE : standard error
11
Table 3. Inter-observer agreement of LI-RADS major imaging features by CT and
MR CT MR CT agreement MR agreement Arterial hyperenhancement Novice 58(92.1%) 57(90.5%) Expert 58(92.1%) 61(96.8%) к=0.566 к=0.475
Portal venous or delayed washout
Novice 45(71.4%) 40(63.5%)
Expert 50(79.4%) 48(76.2%) к=0.364 к=0.630
Capsule appearance
Novice 34(54.0%) 43(68.3%)
12
Figure 1. Image from a 36- year-old man with hepatocellular carcinoma (HCC) in
segment VII of the liver
A. Contrast enhanced arterial phase CT image shows a HCC with nodule-in-nodule
appearance with indistinct margin. B. Contrast enhanced delayed phase CT image shows a HCC with indistinct margin. C. Gadoxetic acid-enhanced arterial phase MR image shows a HCC with nodule-in-nodule appearance. D. Gadoxetic acid-enhanced HBP MR image shows a HCC with clear outline with surrounding parenchyma.
13
14
IV. Discussion
Our study results show the tumor size measurement varies with imaging modalities and each phase. It is still debate which phase should be used to measure the exact size of tumor. The Organ Procurement and Transplantation Network (OPTN) protocol recommends size measurements in the late hepatic arterial or early portal venous phase.(13) On the other hand, LI-RADS allows to measure the size in the most visible phase.(3) The American Association for the Study of Liver Diseases (AASLD) practice guidelines does not specify size measurement methods.(11) Our results showed that the measurement errors of tumor diameter measured by MR were smaller than those measured by CT. It indicates that MR is favorable for size measurement, especially in beginners. Interestingly, there were no statistical significances of the measurement errors between novices and experts on both CT and MR.
Davenport MS et al. reported an inter-observer agreement of the major imaging features in MR, substantial agreement for arterial hyperenhancement (κ = 0.67), moderate for washout appearance (κ = 0.48), and moderate for capsule appearance (κ = 0.52).(8) In contrast, the degree of inter-observer agreement demonstrated in this study was moderate (к = 0.475) for AP hyperenhancement, substantial (к = 0.630) for washout appearance, and fair (к = 0.303) for capsule appearance. These results are lower than those of previous reports, which can be explained in relation to the characteristics of gadoxetic acid. In MR imaging using gadoxetic acid, which shows not only hepatocyte uptake and also biliary excretion, the hepatic AP may appear less intense than with conventional agents.(14) These characteristics of gadoxetic acid can affect low inter-observer agreement in
15
assessing arterial hyperenhancement. In HBP, normal liver parenchyma appears uniformly bright on T1- weighted images because gadoxetic acid accumulates in the extracellular space.(14) Enhanced normal parenchyma can obscure capsule and it could be a cause of low inter-observer agreement.
Comparing the major imaging features, the inter-observer agreement was higher in CT (к = 0.566) than in MR (к = 0.475) for arterial enhancement. When reviewed by expert, the arterial enhancement was better detected in MR than in CT (96.8% vs. 92.1%). Novice’s readings showed a frequency of arterial enhancement similar to that of expert (92.1%) in CT, but revealed a significantly lower detection rate in MR, compared to that of expert’s (90.5% vs. 96.8%). It might be due to characteristics of gadoxetic acid. Since gadoxetic acid may show less intense enhancement in the AP than other contrast agents, it is important to familiarize with the images using gadoxetic acid.
In terms of washout appearance, the inter-observer agreement was higher in MR (к = 0.630) than in CT (к = 0.364) and it might be caused by higher tissue contrast in MR than in CT.
In capsule appearance, the inter-observer agreement was lower in MR (к = 0.303) than in CT (к = 0.491). Specifically, the frequency of capsule appearance in CT and MR was similar (50.8%, 54.0%) in expert, however, there was a significant difference in the frequency of capsule appearance between CT and MR (54.0%, 68.3%) in novice. It suggests that sufficient experience in MR imaging using gadoxetic acid is needed for precise image reading in GAeMR. The frequency of capsular appearance was higher in MR than in CT, not only in expert but also in novice. Strong association between the imaging features of subjective washout and
16
capsule in hypervascular liver nodules may be partially derived from an optical illusion and/or reader predisposition.(15) Therefore, the inter-observer agreement could be lower in capsule appearance.
Ancillary imaging features that favor HCC in LI-RADS includes mild to moderate T2 hyperintensity, restricted diffusion, corona enhancement, mosaic architecture, nodule-in-nodule architecture, intra-lesional fat, lesional iron sparing, lesional fat sparing, blood products, diameter increase less than threshold growth, distinctive rim, HBP hypointense rim, HBP hypointensity.(3) But in our study, limited numbers of cases used ancillary imaging features, because we already knew pathological results. Because there are no standard guidelines, the use of ancillary features may cause bias by radiologist’s discretion.
There was no significant difference between expert and novice in the frequency of final categorization of LI-RADS. When evaluating the value of ICC, it was found that the inter-reader agreement of MR was lower than that of CT (ICC: 0.574 in CT, 0.318 in MR). Although not significant, there was a trend toward increased proportion of LI-RADS 5 lesions at MRI compared to CT.
There are several limitations in our study. First, shrinkage factor after formalin fixation should be considered when reporting tumor size. The tumor size may slightly larger in vivo condition, and that may differ according to the various imaging modalities. So we used the gross pathological size of HCC as reference standard. Second, in our institution, the pathological specimens are usually sectioned in the sagittal or coronal plane, coronal and sagittal images are not always available in retrospective study with CT and GAeMR. Accordingly, we used mainly axial images. Third, we measured the size of each phases of one HCC at the same session, bias could exist. The differences between each phases was very small. It is difficult to measure the size of the HCC with irregular peritumoral
17
enhancement on AP, but it is easier than that to measure the size of HCC with clear outline on HBP image.
18
V. CONCLUSION
In conclusion, the measurement errors of tumor diameter measured by MR were smaller than that measured by CT and MR is favorable for size measurement, especially in beginners. The inter-observer agreement of arterial hyperenhancement and capsule appearance was higher in CT than in MR and in terms of washout appearance, that was higher in MR than in CT. LI-RADS showed fair to moderate agreement for diagnosis of HCC on CT and GAeMR.
19
REFERENCES
1. Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127(12):2893-917.
2. Purysko AS, Remer EM, Coppa CP, Leao Filho HM, Thupili CR, Veniero JC. LI-RADS: a case-based review of the new categorization of liver findings in patients with end-stage liver disease. Radiographics. 2012;32(7):1977-95.
3. Quality and safety resources: Liver Imaging–Reporting and Data System [Internet]. 2012. Available from: http://www.acr.org/Quality-Safety/Resources/LIRADS. 4. Ringe KI, Husarik DB, Sirlin CB, Merkle EM. Gadoxetate disodium-enhanced MRI of the liver: part 1, protocol optimization and lesion appearance in the noncirrhotic liver. AJR Am J Roentgenol. 2010;195(1):13-28.
5. Doo KW, Lee CH, Choi JW, Lee J, Kim KA, Park CM. "Pseudo washout" sign in high-flow hepatic hemangioma on gadoxetic acid contrast-enhanced MRI mimicking hypervascular tumor. AJR Am J Roentgenol. 2009;193(6):W490-6.
6. Ahn SS, Kim MJ, Lim JS, Hong HS, Chung YE, Choi JY. Added value of gadoxetic acid-enhanced hepatobiliary phase MR imaging in the diagnosis of hepatocellular carcinoma. Radiology. 2010;255(2):459-66.
7. Kim SH, Kim SH, Lee J, Kim MJ, Jeon YH, Park Y, et al. Gadoxetic acid-enhanced MRI versus triple-phase MDCT for the preoperative detection of hepatocellular carcinoma. AJR Am J Roentgenol. 2009;192(6):1675-81.
20
8. Davenport MS, Khalatbari S, Liu PS, Maturen KE, Kaza RK, Wasnik AP, et al. Repeatability of diagnostic features and scoring systems for hepatocellular carcinoma by using MR imaging. Radiology. 2014;272(1):132-42.
9. Ehman EC, Behr SC, Umetsu SE, Fidelman N, Yeh BM, Ferrell LD, et al. Rate of observation and inter-observer agreement for LI-RADS major features at CT and MRI in 184 pathology proven hepatocellular carcinomas. Abdom Radiol (NY). 2016;41(5):963-9. 10. Cha MJ, Lee MW, Cha DI, Kim JH, Rhim H, Cho YK, et al. Size discrepancy between sonographic and computed tomographic/magnetic resonance imaging measurement of hepatocellular carcinoma: the necessity of tumor size measurement standardization. J Ultrasound Med. 2013;32(10):1703-9.
11. Bruix J, Sherman M, American Association for the Study of Liver D. Management of hepatocellular carcinoma: an update. Hepatology. 2011;53(3):1020-2. 12. Zhang YD, Zhu FP, Xu X, Wang Q, Wu CJ, Liu XS, et al. Liver Imaging Reporting and Data System:: Substantial Discordance Between CT and MR for Imaging Classification of Hepatic Nodules. Acad Radiol. 2016;23(3):344-52.
13. Policy 9: Allocation of livers and liver-intestines [Internet]. 2017. Available from: https://optn.transplant.hrsa.gov/governance/policies.
14. Goodwin MD, Dobson JE, Sirlin CB, Lim BG, Stella DL. Diagnostic challenges and pitfalls in MR imaging with hepatocyte-specific contrast agents. Radiographics. 2011;31(6):1547-68.
21
perception of capsule affects interpretation of washout in hypervascular liver nodules in patients at risk for hepatocellular carcinoma. J Magn Reson Imaging. 2016;43(6):1337-45.
22 국문 요약
Gadoxetic-acid 조영 증강 자기공명영상을 이용한
간세포암 진단의 LI-RADS 판독자간 일치도의 평가
아주대학교 대학원 의학과 유슬기 (지도교수: 이제희)연구 목적: Gadoxetic-acid를 사용한 조영 증강 자기공명영상(MRI)에서 Liver imaging-reporting and data system (LI-RADS)에 따른 간세포암 진단의 판독자간 의 일치도를 평가하고자 한다. 연구 대상 및 방법: 2013년 1월에서 2015년 12월 사이에 조직학적으로 간세포암으로 확진 된 환자 중 Gadoxetic-acid 조영증강 자기공명영상과 역동적 컴퓨터 단층촬영 (CT)을 진행한 환자들을 대상으로 후향적으로 연구한다. 영상 판독은 2명의 복부 영 상 전문가가 합의하여 판독한 결과와 2명의 전공의가 합의하여 판독한 결과를 비교한 다. LI-RADS 카테고리의 중요 진단 기준인 종양의 크기를 병리학적으로 측정된 크기 와 비교하여 어떤 시기의 영상의 종양의 크기 측정에 가장 정확한지 평가한다. 또한 LI-RADS의 간세포암 진단의 주요 영상소견인 동맥기 조영증강, 세척효과(washout), 피막(capsule appearance)의 판독자간 일치도를 평가하며, 최종 LI-RADS 카테고리 의 CT와 MR에서의 판독자간 일치도를 평가한다. 연구 결과: 총 63명의 환자가 연구에 포함되었다. 병리학적으로 측정된 종양의 크기를 기준값으로 하여 각각의 영상소견에서 측정된 측정값과의 차이를 비교해 보았을 때 측 정 오차는 MRI에서 CT에 비해 더 적은 것을 확인할 수 있었다. 하지만 전공의와 전 문의 사이의 측정 오차에 통계학적인 차이는 없었다. (p=0.29, p=0.62) LI-RADS의 주요 간세포암 영상 특징의 판독자간 일치도를 평가해 보았을 때, 동맥기 조영증강은 CT와 MR에서 모두 중등도의 일치도를 보였으며(к=0.566, 0.475). 세척 효과의 경
23
우 MR에서는 우수한 일치도(к=0.630)를 보인 반면 CT에서는 보통의 일치도(к =0.364)를 보였다. 피막의 경우에는 CT에서 우수한 일치도(к=0.491)를 보였으며, MR에서는 보통의 일치도(к=0.303)를 보였다. LI-RADS 카테고리의 비율은 전공의 와 전문의 비율 간의 큰 차이는 없었고, CT에서의 판독자간 일치도는 우수한 (Intraclass correlation coefficients (ICC) = 0.574) 반면 MR에서는 보통의 일치도 (ICC = 0.318)를 보였다. 연구 결론: 간세포암 종양의 크기 측정에 있어 MR이 CT에 비해 조금 더 정확했으며, 특히 초심자에게 MR이 유리하였다. 판독자간 일치도는 동맥기 조영증강과 피막의 경 우 CT가 MR에 비해 높았으며, 세척 효과의 경우 MR이 CT에 비해 높았다. LI-RADS 카테고리 평가의 판독자간 일치도는 CT와 Gadoxetic-acid 조영증강 MR에서 보통에서 우수한 정도의 일치도를 보였다.