저작자표시-비영리-변경금지 2.0 대한민국 이용자는 아래의 조건을 따르는 경우에 한하여 자유롭게 l 이 저작물을 복제, 배포, 전송, 전시, 공연 및 방송할 수 있습니다. 다음과 같은 조건을 따라야 합니다: l 귀하는, 이 저작물의 재이용이나 배포의 경우, 이 저작물에 적용된 이용허락조건 을 명확하게 나타내어야 합니다. l 저작권자로부터 별도의 허가를 받으면 이러한 조건들은 적용되지 않습니다. 저작권법에 따른 이용자의 권리는 위의 내용에 의하여 영향을 받지 않습니다. 이것은 이용허락규약(Legal Code)을 이해하기 쉽게 요약한 것입니다. Disclaimer 저작자표시. 귀하는 원저작자를 표시하여야 합니다. 비영리. 귀하는 이 저작물을 영리 목적으로 이용할 수 없습니다. 변경금지. 귀하는 이 저작물을 개작, 변형 또는 가공할 수 없습니다.
의학박사 학위논문
Duct-to-Duct Biliary Reconstructions and Complications
in 100 Living Donor Liver Transplantation
Bong-Wan Kim
Major in Medicine
Department of Medical Science
The Graduate School, Ajou University
Duct-to-Duct Biliary Reconstructions and Complications
in 100 Living Donor Liver Transplantation
by
Bong-Wan Kim
A Dissertation Submitted to The Graduate School of Ajou University
in Partial Fulfillment of the Requirements for the Degree of
Ph.D. of Medicine
Surpervised by
Hee-Jung Wang M.D., Ph.D.
Major in Medicine
Department of Medical Science
The Graduate School, Ajou University
This certifies that the dissertation
of Bong-Wan Kim is approved.
SUPERVISORY COMMITTEE
Sang-Uk Han
Hee-Jung Wang
Jae-Hwan Won
Yong-Sik Jung
Sung-Woo Hong
The Graduate School, Ajou University
December, 21st, 2009
i - ABSTRACT -
Duct-to-Duct Biliary Reconstructions and Complications
in 100 Living Donor Liver Transplantation
Background. The biliary complications in duct-to-duct biliary reconstruction of right or left lobe living-donor liver transplantation (LDLT) have been reported various in incidence up to 40 %. And that could result in serious morbidity or mortality to the recipient’s. We evaluated the risk factors for biliary complication and feasible surgical procedure of duct-to-duct reconstruction in adult LDLT. Methods. From February 2005 to March 2008, 100 cases of adult LDLT with duct-to-duct biliary reconstruction were performed. 64 right lobe grafts, 33 left lobe grafts, and 3 right lateral grafts were used. There were four types of duct-to-duct procedure; all interrupted suture with 6-0 prolene (Group 1, n = 9), continuous posterior and interrupted anterior wall suture with 6-0 prolene (Group 2, n = 49), all continuous suture with 7-0 prolene (Group 3, n = 26), and all continuous 7-0 prolene suture with external stent (Group 4, n = 16). Biliary complications were defined as anastomosis stricture and leakage. Results. 34 patients experienced biliary complications during follow-up time (median 27 months). The incidence of stricture was 27% and that of leakage was 8%. There were no risk factors of biliary complication associated with peri-operative, intra-operative, and anatomical characteristics, except types of duct-to-duct procedure. Group 1 and 2 patients had higher incidence of biliary stricture than Group 3 and 4 (43.1% vs. 4.7%, P = 0.00). And Group 3
patients experienced higher incidence of bile leakage than other groups (23.1% vs. 2.7%, P = 0.004). Conclusion. The technical type of biliary reconstruction is the factor affecting biliary complication following duct-to-duct anastomosis in LDLT. Duct-to-duct biliary anastomosis with 7-0 monofilament suture and small external stent is a feasible procedure in LDLT to significantly reduce the incidence of biliary complication.
Key Words: Living donor liver transplantation, Duct-to-duct anastomosis. Biliary complication.
iii
TABLE OF CONTENTS
ABSTRACT i
TABLE OF CONTENTS iii
LIST OF TABLE iv
LIST OF FIGURE v
I. INTRODUCTION 1
II. PATIENTS AND METHODS 3
A. Preparation of Graft Bile Duct 5
B. Recipient Operation 7
C. Diagnosis and Treatment of Biliary Complications 11
D. Statistical Analysis 12 III. RESULTS 13 IV. DISCUSSION 24 V. CONCLUSION 32 VI. REFERENCES 33 VII. 국문요약 36
LIST OF TABLE
Table 1. Numbers of graft, bile ducts and biliary anastomosis. 14
Table 2. Risk factor analysis for biliary stricture. 20
v
LIST OF FIGURE
Figure 1. Types of procedures and materials in duct-to-duct anastomosis. 9
Figure 2. Comparisons of biliary complication-free survival rates between Groups. 18 Figure 3. A pitfall in technique of graft’s duct slid into recipient’s duct to 27
I. INTRODUCTION
Recently, with improved surgical techniques of preservations for the blood supply to the recipient’s supraduodenal common bile duct and partial graft’s bile ducts, duct-to-duct biliary reconstruction has become standard in living-donor liver transplantation (LDLT). Many LDLT centers adopted duct-to-duct anastomosis as the choice of biliary reconstruction nowadays because it has certain advantages in terms of physiological, anatomical, and technical feasibility over Roux-en-Y hepaticojejunostomy (RYHJ). Yet, the long-term biliary complications in duct-to-duct biliary reconstruction of right or left lobe LDLT have been reported various in incidence up to 40 %.(Soejima, 2003; Liu, 2004; Kasahara, 2006; Tashiro, 2007) And biliary stricture and leakage at the anastomosis site are major concerns of these complications, which are strongly associated with surgical techniques of bile duct preparations and anastomosis.
Despite considerable innovation of duct-to-duct procedure was achieved in the while, some procedures are still open questions. Technical consensus was established to preserve adequate blood supply in procedures for preparation of graft and recipient’s bile
2
ducts.(Shokouh-Amiri, 2001; Ishiko, 2002) However, type of suture techniques, selection of suture materials, and use of stenting tube are still on debates.( Liu, 2004; Kasahara, 2006; Yan, 2007)
Duct-to-duct biliary reconstruction in LDLT has been used as standard procedure in our center since 2005. We have performed four different procedures of biliary anastomosis, according to type of anastomosis, suture material, and use of external stent tubing. In this study, we evaluated the risk factors of biliary complications and the most feasible surgical technique and material for duct-to-duct reconstruction in LDLT.
II. PATIENTS AND METHODS
Between February 2005 and March 2008, 100 adult patients (26-68 years old, 82 male patients and 18 female patients) underwent LDLT with duct-to-duct biliary reconstruction at Ajou University Hospital and survived longer than 1 month after transplantation. We excluded the patients who had definite risk factor of biliary complication: five ABO blood-type incompatible recipients and two patients who experienced immediate postoperative hepatic artery thrombosis. The underlying liver diseases of the 100 recipients were liver cirrhosis (n = 55), hepatocellular carcinoma (n = 40), Metabolic liver disease (n = 2), fulminant hepatic failure (n = 2), and primary biliary cirrhosis (n = 1). The Model for End-Stage Liver Disease score ranged from 6 to 43.
The body weight of the recipients ranged from 45 to 89 kg, and the median was 66 kg. The actual graft volume (GV) was measured on the back table after graft perfusion of Histidine-Tryptophan-Ketoglutarate (HTK) solution. And the graft weight ranged from 302 to 930 g. The standard liver volume (SLV) of the recipients was calculated according to the formula of Urata et al.(Urata, 1995) The GV/SLV ratio ranged from 31 to 79.7%, and the
4 median was 49%.
The types of graft were right lobe graft with or without middle hepatic vein (n = 64), left lobe graft with or without caudate lobe (n = 33), and right lateral graft (segments VI and VII) (n = 3). The follow-up period ranged from 6 to 42 months (median 27).
A. Preparation of Graft Bile Duct
Standard surgical techniques for donor hepatectomy have been previously described.(Kim, 2007) After cholecystectomy, intraoperative cholangiogram was routinely performed through cystic duct to identify the anatomy of the bile duct. After parenchymal dissection of the liver, intraoperative cholangiogram was performed again with radio-opaque marker on the bile duct to determine the site of bile duct transection. Minimal dissection of peri-biliary soft tissue without using electro-cautery on hilar bile duct was performed, and the bile duct was divided with sharp scissors. Arterial bleeding from soft tissue around the cut end of graft duct was regarded as a good sign. The bile duct was transected with more than 2-3 mm safe margin from the origin of bifurcation to prevent bile duct stricture of remnant liver. The openings of the remnant liver bile ducts were closed using continuous 6-0 or 7-0 prolene suture. Finally, dye leakage test and cholangiogram were performed to confirm no leakage or stricture.
The harvested grafts were stored at ice-water temperature in HTK solution. On the back table, in cases of the proximal two bile ducts or the prominent septum in single duct opening,
6
ductoplasty or septoplasty were performed to create a common bile duct orifice with 7-0 nonabsorbable polypropylene monofilament (prolene) continuous suture.
B. Recipient Operation
Preparation of recipient bile ducts was performed by minimal dissection of pericholedochal soft tissue to preserve the “3 o’clock” and “9 o’clock” arteries. The bundle of soft tissue including bile duct and hepatic arteries was dissected from the portal vein to avoid arterial devascularization of bile duct, and it was transected above hilar bifurcation with sharp scissors. We confirmed that the recipient bile duct had a good blood supply by identifying significant arterial bleeding from the cut end of the duct.
After completion of vascular anastomosis, the graft bile duct was anastomosed to the recipient bile duct in the end-to-end manner. Before starting duct-to-duct anastomosis, we confirmed that the length of recipient’s duct was sufficient to prevent tension at the anastomosis. We preferred to use recipient’s common hepatic duct for single biliary anastomosis for good blood supply to recipient’s bile duct. And recipient’s right and left hepatic ducts are used for biliary reconstructions when two duct-to-duct anastomoses were needed. The duct-to-duct biliary anastomosis was performed in all patients, but in one case, additional Roux-en-Y hepaticojejunostomy (RYHJ) was performed for second opening of the
8 graft bile duct which was too far from the first.
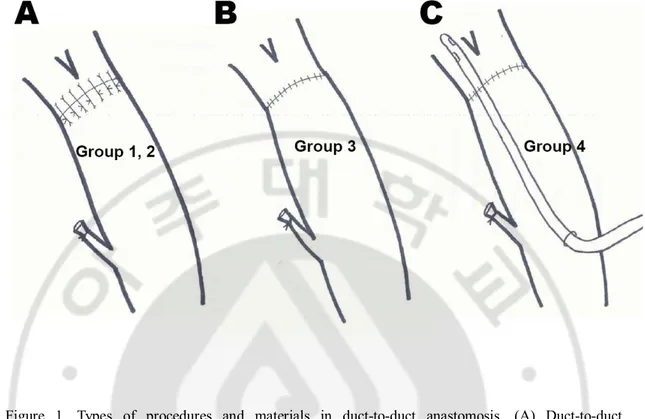
All biliary anastomoses were performed by two surgeons under surgical loupe. We have used four different types of duct-to-duct procedures according to manners of anastomosis and suture materials in three years of this study. First, duct-to-duct anastomosis was performed with interrupted 6-0 prolene suture on both anterior and posterior walls (Group 1; n = 9) between February and August 2005. Then we had changed the anastomosis procedure to continuous suture on the posterior wall and interrupted suture on the anterior wall using 6-0 prolene up to September 26-06-06 (Group 2; n = 49). Next, from October 26-06-06, we have changed fashion and material of suture to continuous manner on both anterior and posterior walls with 7-0 prolene (Group 3; n = 26). And finally, from December 2007 to February 2008, we have additionally inserted 4- or 5-French polyethylene external stents into recipient bile duct up across the anastomosis site (Group 4; n = 16). The type of bile duct anastomosis in each group is illustrated in Figure 1.
Figure 1. Types of procedures and materials in duct-to-duct anastomosis. (A) Duct-to-duct anastomosis with 6-0 prolene suture. Interrupted sutures on posterior and anterior duct walls were performed in Group 1 patients (n = 9). And continuous posterior wall sutures with interrupted anterior wall sutures were performed in Group 2 patients (n = 49). (B) Group 3 patients (n = 26) had continuous posterior and anterior wall sutures with prolene 7-0. (C) Group 4 patients (n = 16) underwent external stent tubing during continuous 7-0 prolene duct anastomosis.
The distance between the stitches was about 1 mm in the patients using 6-0 prolene (Group 1, 2), and about 0.5 - 0.7 mm in the patients using 7-0 prolene (Group 3, 4). The external stent was anchored with 6-0 absorbable polyglyconate monofilament suture (maxon). It was placed to drain bile until two weeks after transplantation and was clamped.
10
Then it was removed three or four months after transplantation.
The protocols of immunosuppression have not changed for this study period. Induction of immunosuppression was consisted of basiliximab and steroid. 20 mg of basiliximab was given on transplantation day and postoperative day 4, and corticosteroid bolus injection (10mg/kg of methylprednisolone) was given in anhepatic period to all patients. Maintenance of immunosuppression was consisted of calcineurin inhibitor (tacrolimus or cyclosporine), and if needed, mycophenolate mofetil was added. Postoperative oral steroid (prednisolone) was tapered and discontinued within three months after transplantation.
C. Diagnosis and Treatment of Biliary Complications
The biliary complications were classified as biliary stricture and anastomosis leakage, and those were diagnosed clinically and radiologically. Liver dynamic computed tomography (CT) and hepatobiliary scintigraphy (HBS) were routinely performed weekly during the first month after transplantation, and then two or three times over the following year. Postoperative cholangiogram was not routinely performed in the patients who were introduced external stent unless they were suspected to have clinical or radiological biliary complications. If and when the patients showed any clinical finding of biliary complications such as bile stained abdominal drainage, abnormal liver function tests, itching symptom, and etc, the radiological examinations mentioned above were performed immediately.
Biliary stricture was confirmed and treated using percutaneous transhepatic biliary drainage (PTBD), and sequential dilatation was repeated every month until complete resolution. Endoscopic retrograde biliary drainage (ERBD) and percutaneous drainage (PCD) were used for treating the patients who had anastomosis leakage.
12
D. Statistical Analysis
Chi-square or Student’s T test were used for comparison of variables. Survival curves were estimated using Kaplan-Meier method and compared using log-rank tests. A P value < 0.05 was considered to be significant.
III. RESULTS
The number of bile duct opening in every graft was one or two, and there was no graft with more than two duct openings in this series. Among 64 right lobe grafts, 41 grafts had single bile duct opening and 23 had two bile duct openings. Among 41 right grafts with single duct, 7 underwent septoplasty on the back table due to significant septum inside the orifice. And among 23 right grafts with two duct openings, 15 grafts had proximal duct openings which were unified with ductoplasty to make a single opening, and remaining 8 had two distant openings that were anastomosed to recipient’s bile duct separately. All 33 left lobe grafts had single bile duct opening, but 3 grafts had septoplasty due to significant septum in the bile duct orifice. Three right lateral grafts each had a single duct opening.
The number of patients using right or right lateral graft in each group was 6 of 9 (66.7%) in Group 1, 34 of 49 (69.4%) in Group 2, 15 of 26 (61.5%) in Group 3, and 11 of 16 in Group 4 (68.8%). The proportion of right or right lateral graft LDLT was nearly homogenous among the groups (P = 0.92). Characteristics of grafts and bile ducts in each group are summarized in Table 1.
14
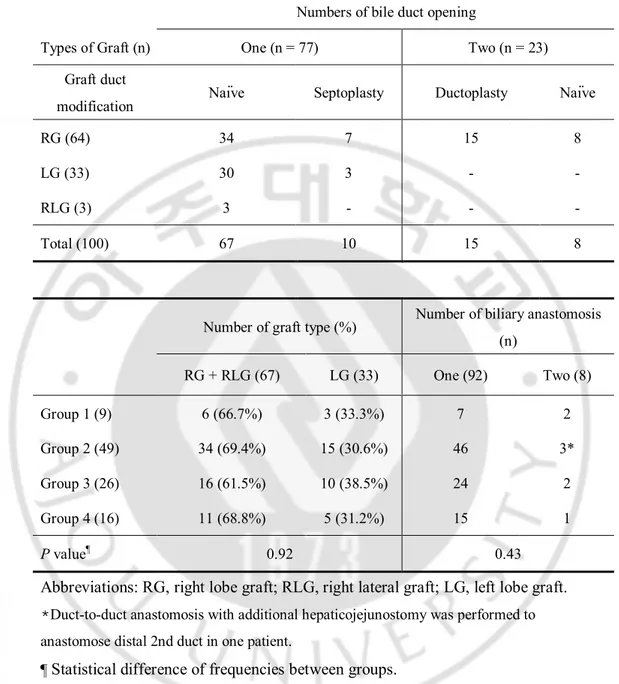
Table 1. Numbers of graft, bile ducts and biliary anastomosis. Numbers of bile duct opening
Types of Graft (n) One (n = 77) Two (n = 23)
Graft duct
modification Naïve Septoplasty Ductoplasty Naïve
RG (64) 34 7 15 8
LG (33) 30 3 - -
RLG (3) 3 - - -
Total (100) 67 10 15 8
Number of graft type (%) Number of biliary anastomosis (n) RG + RLG (67) LG (33) One (92) Two (8) Group 1 (9) 6 (66.7%) 3 (33.3%) 7 2 Group 2 (49) 34 (69.4%) 15 (30.6%) 46 3* Group 3 (26) 16 (61.5%) 10 (38.5%) 24 2 Group 4 (16) 11 (68.8%) 5 (31.2%) 15 1 P value¶ 0.92 0.43
Abbreviations: RG, right lobe graft; RLG, right lateral graft; LG, left lobe graft. *Duct-to-duct anastomosis with additional hepaticojejunostomy was performed to anastomose distal 2nd duct in one patient.
The median follow-up period was 27 months (range 6 - 42), and during this period, seven patients died due to recurrent HCC (n = 4), rejection (n = 2), and cardiac tamponade (n = 1). Overall 1-yr and 3-yr survival rates were 97.9% and 91.2%. Biliary complications developed in total of 34 patients (34%), and eight patients (8%) were diagnosed as anastomosis leakage while 27 patients (27%) developed stricture. One patient developed biliary stricture following leakage.
All anastomosis leakage (n = 8) developed within the first month (7 – 23 days) after transplantation. All of them were successfully treated with ERBD and abdominal drainage. Two of 8 patients, who had experienced anastomosis leakage, died of recurrent carcinoma or severe rejection at 7 and 12 months respectively after transplantation. The time onset of biliary stricture (n = 27) ranged from 14 days to 32 months after transplantation. Nine patients developed stricture within 3 months, 16 between 4 months and 1 year, and two 1 year after transplantation. All biliary strictures were diagnosed as biliary stenosis at the anastomosis site, and there was no ischemic-type biliary complication.(Sanchez-Urdazpal, 1993) The patients were treated using PTBD and sequential dilatation. And they all have survived up to now, and 22 of them have been successfully completed interventional therapy.
16
The incidences of biliary complication using right lobe and left lobe graft were 37.5% (24 of 64) and 30.3% (10 of 33) respectively (P = 0.35). Among 64 patients with right lobe graft, 21 patients (32.8%) experienced biliary stricture and four patients (6.3%) experienced anastomosis leakage. In cases of left lobe graft (n = 33), biliary stricture was developed in six (18.2%) patients and leakage was developed in four (12.1%) patients. And there was no right lateral graft recipient (n = 3) who developed biliary complications. There was no difference in incidence of anastomosis leakage and stricture according to the graft type (P = 0.67, 0.17 respectively).
No significant risk factors affecting development of biliary complications existed except the procedure types of biliary reconstruction (Table 2, 3). The incidences of biliary complication in each group according to types of duct-to-duct anastomosis were 44.4% in Group 1, 44.9% in Group 2, 30.7% in Group 3, and 0% in Group 4.
Biliary stricture developed in four patients (44.4%) and no patient had leakage in the Group 1 patients (n = 9). And the patients of Group 2 (n = 49) developed anastomosis stricture in 21 patients (42.8%) and 2 leakage (4%). The incidences of biliary stricture and leakage in the Group 3 patients (n = 26) were 7.7% (2 of 26) and 23% (6 of 26) respectively. No biliary
stricture and leakage (0%) was developed in the patients of Group 4 (n = 16).
The biliary stricture-free survival rates in Group 3 and 4 were significantly higher than Group 1 and 2 (P = 0.001), and biliary leakage-free survival rates were lower in Group 3 than Group 1,2 and 4 with statistical significance (P = 0.009) (Fig. 2). There was no patient who developed bile leakage related to removal of external stent in Group 4.
18 Group 1 Group 2 Group 3 Group 4
A
Group 1 Group 2 Group 3 Group 4B
Figure 2. Comparisons of biliary complication-free survival rates between Groups. (A) Stricture-free survival rates showed in Group 3 (92.1%) and 4 (100%) patients were significantly higher than Group 1 (55.6%) and 2 (54.6%) patients (P = 0.001). (B) Leakage-free survival rates were lower in Group 3 patients (76.9%) than other groups of patients (100%, 95.9% and 100% in group order) (P = 0.009).
20 Table 2. Risk factor analysis for biliary stricture
Biliary stricture (number or mean ± standard deviation) Risk factors No (73) Yes (27) P Recipient age (yr) 46.6 ± 8.5 49.5 ± 6.7 0.25 Donor age (yr) 32.1 ± 9.4 28.5 ± 8.7 0.69 CIT (min) 156.9 ± 49.6 152.3 ± 51.5 0.93 WIT (min) 48.7 ± 15.1 51.6 ± 28.3 0.19 AAT (min) 77.2 ± 41.6 93.7 ± 42.8 0.97 MELD score 17.5 ± 8.6 15.9 ± 6.7 0.21 GV/SLV (%) 49.3 ± 10.5 54.5 ± 12.5 0.09 Graft type Right lobe 43 21 0.17 Left lobe 27 6 Right lateral sector 3 0
Bile duct diameter (mm) 4.1 ± 1.56 4.2 ± 1.3 0.64 Number of bile duct
Single 56 21 0.57 Two 17 6
Graft duct modification
No 54 21 0.87 Septoplasty 8 2
Ductoplasty 11 4 Number of duct anastomosis
One 67 25 0.63 Two 6 2
Technique of duct anastomosis
Group 1 5 4 0.001 Group 2 28 21
Group 3 24 2 Group 4 16 0
Abbreviation: GV, actual graft volume; SLV, standard liver volume; CIT, cold ischemic time; WIT, warm ischemic time;
22 Table 3. Risk factor analysis for biliary leakage
Biliary leakage (number or mean ± standard deviation)
Risk factors No (n = 91) Yes (n = 8) P Recipient age (yr) 47.9 ± 8.2 42.7 ± 7 0.07 Donor age (yr) 31.2 ± 9.6 30.2 ± 7.2 0.75 CIT (min) 152.3 ± 48.9 163.5 ± 51.2 0.34 WIT (min) 49.4 ± 20.2 50 ± 12.2 0.94 AAT (min) 83.7 ± 43.1 62.2 ± 28.5 0.14 MELD score 17.1 ± 7.8 17.8 ± 11.1 0.82 GV/SLV (%) 50.8 ± 11.3 47.8 ± 9.6 0.46 Graft type Right lobe 60 4 0.52 Left lobe 29 4 Right lateral sector 3 0
Bile duct diameter (mm) 4.1 ± 1.5 3.4 ± 1.0 0.17 Number of bile duct
Single 71 6 0.59 Two 21 2
Graft duct modification
No 68 7 0.58 Septoplasty 10 0
Ductoplasty 14 1 Number of duct anastomosis
One 85 7 0.5 Two 7 1
Technique of duct anastomosis
Group 1 9 0 0.011 Group 2 47 2
Group 3 20 6 Group 4 16 0
24
IV. DISCUSSION
The biliary complication following liver transplantation is a significant cause of patient’s long term morbidity and mortality, and it usually deprives the patient’s quality of life for a long time, even though most of them could be treated with non-surgical modality. In the absence of specific contraindications, duct-to-duct anastomosis in LDLT is the choice of biliary reconstruction in many programs nowadays, even in cases with multiple graft ducts. The incidences of biliary complications reported in patients who underwent LDLT with duct-to-duct reconstruction widely ranged from 8 to 60%.(Kawachi, 2002; Sugawara, 2003) Such wide ranges of incidences of biliary complications among centers could be due to difference in technique and experience. Also in this study, we experienced that the type of procedure and material in duct-to-duct anastomosis was significantly associated with incidences of biliary complication following LDLT.
There are some advantages and disadvantages in duct-to-duct biliary reconstruction compared to bilioenterostomy in LDLT. Duct-to-duct biliary anastomosis is technically quicker, more physiologic and anatomic, and easily accessible by endoscopic approach to
biliary system after transplantation. On the other hand, there could be two major surgical disadvantages. One is possible tension at the anastomosis when recipient’s duct is inappropriately prepared, and the other is size discrepancy between openings of graft’s and recipient’s duct.
Preparation of sufficient length of recipient’s bile duct with adequate blood supply is fundamental to perform tension-free duct-to-duct anastomosis. Because the axial arteries from gastroduodenal artery and right hepatic artery have important role in pericholedocal vascular network, it is necessary to minimally dissect the soft tissues around the bile duct.(Northover, 1979) During preparation of graft’s and recipient’s ducts, arterial bleedings from the cut end of bile ducts should be identified before duct-to-duct anastomosis. If it is not, the bile duct should be shortened. Lee et al.(Lee, 2004) introduced a useful technique of preparing recipient’s bile duct, the high hilar dissection, to provide sufficient length and blood supply of recipient’s bile duct. We think this technique is very useful especially when preparing quite a length of recipient’s bile duct or when multiple duct-to-duct anastomoses are necessary.
26
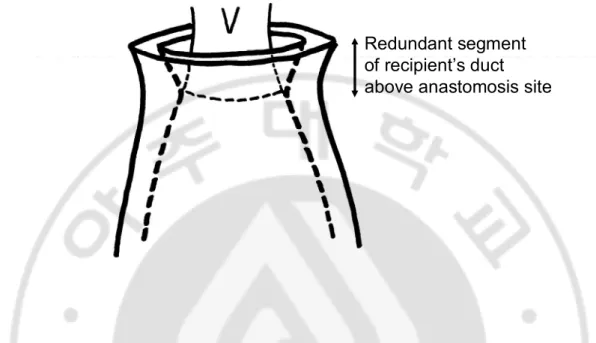
problem in duct-to-duct-anastomosis. Ensuring tension-free anastomosis, we preferred to anastomose graft’s duct to recipient’s common hepatic duct because the cut end of recipient’s intrahepatic bile ducts are usually thin and friable. According to our data, the average diameter of partial graft duct was about 4 mm, whereas the recipient’s common hepatic duct usually had twice the luminal diameter than the graft’s duct. To overcome this problem, the graft duct was slid into the socket of recipient’s common hepatic duct mucosa by transmural suture of graft’s duct and transmucosal suture of recipient’s common hepatic duct. In our experience, this technique was useful to successfully deal with size discrepancy. But it had a possible problem when the graft duct was too deeply slid into recipient’s common hepatic duct so that too much redundant segment of recipient’s duct could be left around graft’s duct (Fig. 3). That could cause collapse of graft’s bile duct and sequential bile duct obstruction. So we recommend that the sliding depth of graft’s duct should be minimized.
Redundant segment
of recipient’s duct
above anastomosis site
Figure 3. A pitfall in technique of graft’s duct slid into recipient’s duct to overcome size discrepancy; If redundant segment of recipient’s duct were left over around anastomosis site, it could compress graft’s bile duct and develop biliary obstruction. Unused segment of recipient’s bile duct should be minimized.
In this series, we used three types of suturing methods in duct-to-duct biliary anastomosis: all interrupted, posterior wall continuous with anterior wall interrupted, and all continuous. Between 6-0 prolene duct-to-duct anastomosis groups (Group 1 and 2), there was no difference in the incidence of stricture and leakage. Therefore, the selection of suturing type between all interrupted or posterior wall continuous had a little effect on the
28
outcomes after duct-to-duct anastomosis. Unfortunately, we could not compare the outcomes of all continuous sutures with the other methods because we used different sizes of needle and thread.
However, the incidence of biliary complications was reduced after changing suture material from 6-0 to 7-0 prolene. Especially, the incidence of biliary stricture significantly decreased from 43% to 4.7% (P = 0.00). According to this result, the size of the suture needle could be an important factor in duct-to-duct biliary anastomosis in LDLT.
In biliary anastomosis, there are two possible difficulties in suturing ducts; the first is due to the direction of stitching. Putting stitches in graft duct is performed in direction from hidden dorsal side to visible ventral side, and it is more challenging to make fine stitches on graft’s duct than recipient’s duct. Secondly, bigger the size of suture needle, fine handling becomes more difficult. Commonly used 6-0 sized needle has quite a length (13 mm) compared to the size of partial graft’s duct and operative space in duct anastomosis. Therefore, when the anastomosis is performed with 6-0 needle, it largely depends on surgeons’ experience to achieve exact suture points at the graft duct. And frequently it could be more deeply pointed than the surgeons’ target, which could cause narrowing of duct
lumen and technical failure in biliary anastomosis.
Using smaller suture needle in duct-to-duct biliary reconstruction has advantages in achieving precise anastomosis. In our experience, smaller 7-0 needle was much comfortable to stitch exact site on the graft duct than 6-0. After using 7-0 prolene suture in this study, we experienced that the incidence of biliary stricture was significantly reduced. Using smaller suture material allowed us to improve technical refinement in biliary reconstruction.
Many centers prefer to use 6-0 monofilament suture even nowadays for biliary reconstruction. Although, Kyoto group reported that they recently started to use 7-0 monofilament suture, they didn’t report the outcomes of using this material.(Kasahara, 2006) Recently, Yan et al.(Yan, 2007) reported favorable result of microsurgical technique to biliary reconstruction of small hepatic duct with 8-0 prolene. In the future, further study with larger number of patients using small suture material for biliary anastomosis should be initiated to figure out the effective outcomes on reduced incidence of biliary complications.
Meanwhile, we also experienced that incidence of biliary leakage was increased after using 7-0 prolene suture (six of 26 Group 3 patients, 23%). Fortunately, all of them were successfully treated with endoscopic and abdominal drainage. Treating these six leakage
30
patients, no major disruption of anastomosis but pinpoint leakage from biliary anastomosis was observed. According to these findings, we concluded that the cause of bile leakage in continuous 7-0 biliary anastomosis was not from breaking of thread due to weakness but from partial tearing of sutured graft duct because some part was stitched too shallowly. To solve that problem, we adopted 4- or 5-French sized external biliary stent tubing rather than deeper pointing of stitches to the graft duct.
Our experience showed that external stent tubing was possibly able to reduce incidence of biliary complications, especially leakage. Among patients with 7-0 continuous suture, the incidence of biliary complication was reduced from 30.8% to 0% (P = 0.01) after using external stent. Also we did not experience any complications related to removal of 4- or 5-French external stent. Our current preference of duct-to-duct biliary procedure in LDLT is 7-0 continuous suture with external stent. We think this procedure is feasible in duct-to-duct biliary reconstruction to reduce incidence of biliary complication following LDLT.
However, a multicenter, prospective randomized trial in deceased liver transplantation showed that incidence of biliary complication was significantly higher in group of patients with T-tube biliary stenting than without. (Scatton, 2001) Ben-Ari et al.(Ben-Ari, 1998) also
didn’t recommend T-tube stenting after cadaveric liver transplantation due to high incidence of septic complication. Also, previous studies reported bile leakage complication following T-tube removal.(Urbani, 2002; Wojcicki, 2006)
But tube stenting in duct anastomosis is still controversial in LDLT where the bile duct openings are usually small in size. Hong Kong group reported that duct-to-duct reconstruction was safely performed in LDLT without biliary stent tube, reporting 24% incidence of biliary complication.(Liu, 2004) However, Kyoto group reported slightly lower incidence of biliary complication compared to Hong Kong group using biliary stent in right lobe LDLT (17.6%).(Ishiko, 2002) It should be subject to large sized, prospective randomized study to prove the effectiveness of biliary stent tubing in LDLT.
32
V. CONCLUSION
In conclusion, the development of biliary complication after duct-to-duct biliary reconstruction in LDLT is significantly related to technical procedure and suture material. Duct-to-duct biliary anastomosis with 7-0 monofilament suture and small external stent is a feasible procedure in LDLT. Using these procedures could provide refined surgical techniques and reduce the incidence of biliary complication to a satisfactory level.
VI. REFERENCES
1. Ben-Ari Z, Neville L, Davidson B, Rolles K, Burroughs AK. Infection rates with and without T-tube splintage of common bile duct anastomosis in liver transplantation. Transpl Int 11: 123-126, 1998
2. Ishiko T, Egawa H, Kasahara M, et al. Duct-to-duct biliary reconstruction in living donor liver transplantation utilizing right lobe graft. Ann Surg 236: 235-40, 2002
3. Kasahara M, Egawa H, Takada Y, et al. Biliary reconstruction in right lobe living-donor liver transplantation: Comparison of different techniques in 321 recipients. Ann Surg 243: 559-566, 2006
4. Kawachi S, Shimazu M, Wakabayashi G, et al. Biliary complications in adult living donor liver transplantation with duct-to-duct hepaticocholedochostomy or Roux-en-Y hepaticojejunostomy biliary reconstruction. Surgery 132: 48-56, 2002
5. Kim BW, Park YK, Paik OJ, Lee BM, Wang HJ, Kim MW. Effective anatomic reconstruction of the middle hepatic vein in modified right lobe graft living donor liver transplantation. Transplant Proc 39: 3228-3233, 2007
6. Lee KW, Joh JW, Kim SJ, et al. High hilar dissection: new technique to reduce biliary complication in living donor liver transplantation. Liver Transpl 10: 1158-1162, 2004
34 77: 726-732, 2004
8. Northover JM, Terblanche J. A new look at the arterial supply of the bile duct in man and its surgical implications. Br J Surg 66: 379-384, 1979
9. Sanchez-Urdazpal L, Gores GJ, Ward EM, et al. Diagnostic features and clinical outcome of ischemic-type biliary complications after liver transplantation. Hepatology 17: 605-609, 1993
10. Scatton O, Meunier B, Cherqui D, et al. Randomized trial of choledochocholedochostomy with or without a T tube in orthotopic liver transplantation. Ann Surg 233: 432-437, 2001
11. Shokouh-Amiri MH, Grewal HP, Vera SR, Stratta RJ, Bagous W, Gaber AO. Duct-to-duct biliary reconstruction in right lobe adult living donor liver transplantation. J Am Coll Surg 192: 798-803, 2001
12. Soejima Y, Shimada M, Suehiro T, et al. Feasibility of duct-to-duct biliary reconstruction in left-lobe adult-living-donor liver transplantation. Transplantation 75: 557-559, 2003
13. Sugawara Y, Sano K, Kaneko J, et al. Duct-to-duct biliary reconstruction for living donor liver transplantation: experience of 92 cases. Transplant Proc 35: 2981-2982, 2003
14. Tashiro H, Itamoto T, Sasaki T, et al. Biliary complications after duct-to-duct biliary reconstruction in living-donor liver transplantation: causes and treatment. World J Surg 31: 2222-2229, 2007
15. Urata K, Kawasaki S, Matsunami H, et al. Calculation of child and adult standard liver volume for liver transplantation. Hepatology 21: 1317-1321, 1995
16. Urbani L, Campatelli A, Romagnoli J, et al. T-tube removal after liver transplantation: a new technique that reduces biliary complications. Transplantation 74: 410-413, 2002
17. Wojcicki M, Silva MA, Jethwa P, et al. Biliary complications following adult right lobe ex vivo split liver transplantation. Liver Transpl 12: 839-844, 2006
18. Yan L, Li B, Zeng Y, et al. Preliminary experience for reducing biliary complication in adult-to-adult living donor liver transplantation using right lobe graft. Hepatol Res 37: 305-309, 2007
19. Yan L, Li B, Zeng Y, et al. Introduction of microsurgical technique to biliary reconstruction in living donor liver transplantation. Transplant Proc 39: 1513-1516, 2007
36 - 국문 요약 –
담도-담도 문합술을 시행한 100례의 생체 부분 간이식
환자에서 담도합병증의 위험인자 분석
생체 부분 간을 이용한 간이식에서 담도 합병증은 현재까지도 보고자에 따라 40%의 유병율을 보이며, 부분 간이식의 술기의 ‘Achilles’ hill’ 이라고 불리고 있 다. 간이식 후 발생한 담도 합병증은 심각한 합병증을 남기거나 심지어 사망에 이르게 할 수 있어, 이를 줄이는 것은 간이식 의사에게 매우 중요한 일이다. 본 연구에서는 담도-담도 문합을 시행한 생체 부분 간이식 환자에서 담도 합병 증 발생의 위험인자를 분석하여 보고자 하였다. 대상 및 방법 : 2005년 2월부터 2008년 3월 까지 담도-담도 문합을 시행하였던 생체 부분 간이식 환자 100명을 대상으로 하였다. 그 중 64명의 환자는 간 우엽을, 33명은 간 좌엽을, 3명의 환 자는 간 우후엽을 이용하여 간이식을 시행 받았다. 100명의 대상 환자는 시기 에 따라 4가지 방식의 담도 분합 방법을 취하였는데, 제 1군은 (n = 9) 담도의 앞과 뒷벽을 모두 prolene 6-0 를 이용하여 단속봉합을 시행하였고, 제 2군은 (n = 49) prolene 6-0를 이용하여, 담도의 뒷벽은 연속봉합, 앞면은 단속봉합을 시행 하였으며, 제3군은 (n = 26) prolene 7-0를 이용하여 담도의 앞과 뒷벽 모두 연속 봉합, 마지막으로 제 4군은 (n = 16) 제 3군과 같은 봉합 방법을 사용하고 부가 적으로 담도 내 도관 삽입을 시행한 군이었다. 담도 합병증은 담도 협착증과 담도 누출로 정의 하였다. 결과 : 추적 기간 중 (평균 27 개월) 34명에서 담도합병증을 경험하였다. 담도 협착증이 27예에서, 담도 누출이 8예에서 보였다. 단변량 분석결과 수술 관련 요소 및 해부학적인 요소 중 오로지 담도의 봉합 방법 만이 유일한 차이를 보이는 위험인자로 분석되었다. 제 1, 2 군의 경우 제 3, 4 군에 비해 담도 협착증이 유의하게 많았다 (43.1% vs. 4.7%, P = 0.00). 제 3 군에서는 다른 군에 비해 담도 누출이 유의하게 많았다 (23% vs. 2.7%, P = 0.004). 결론 : 담도 문합의 술기적인 방법은 담도 합병증의 발생과 매우 밀법 한 관계가 있다. 생체 부분 간이식의 담도-담도 문합에 있어 7-0 monofilament 봉합사를 이용한 봉합과 부가적인 도관 삽입은 담도 합병증의 발생을 줄일 수 있는 유용한 방법이라고 생각한다. 핵심 단어: 생체 부분 간이식, 담도-담도 문합술, 담도 합병증.