의
의
의
의학
학
학
학
석사학위
석사학위
석사학위
석사학위
논문
논문
논문
논문
Surface Models of the Gastrointestinal
Tract and Neighboring Structures
Made from the Visible Korean Human
아
아
아
아
주
주
주
주
대
대
대
대
학
학
학
학
교
교
교
교
대
대
대
대
학
학
학
학
원
원
원
원
의
의
의
의
학
학
학
학
과
과
과
과
박
박
박
박
효
효
효
효
석
석
석
석
Surface Models of the Gastrointestinal
Tract and Neighboring Structures
Made from the Visible Korean Human
by
Hyo Seok Park
A Dissertation Submitted to The Graduate School of
Ajou University
in Partial Fulfillment of the Requirements for the Degree of
MASTER OF MEDICAL SCIENCES
Supervised by
Min Suk Chung, M.D., Ph.D.
Department of
Department of
Department of
Department of Medical Sc
Medical Sc
Medical Sc
Medical Sciences
iences
iences
iences
The Graduate School, Ajou University
The Graduate School, Ajou University
The Graduate School, Ajou University
The Graduate School, Ajou University
February, 200
February, 200
February, 200
February, 2008
8
8
8
박효석의
의학
석사학위
논문을
인준함
.
심사위원장 정 민 석
인심사위원 김 재 근
인심사위원 박 래 웅
인아 주 대 학 교 대 학 원
2007
년 12월 21일
- ABSTRACT -
Surface Models of the Gastrointestinal Tract and Neighboring
Structures Made from the Visible Korean Human
Surface models of the gastrointestinal (GI) tract and neighboring abdominal structures can be opened and rotated in a real time, which is helpful to understanding anatomy of digestive system. However, we could not find objective surface models made from the serially sectioned images. In order to make the surface models, whole length of the GI tract was outlined in the serially sectioned images of the Visible Korean Human; the outlining was supported by the enhanced technique of filtering and interpolation. Subsequently, highly curved GI tract was divided into several parts, and each part was surface reconstructed and united with one another to acquire a surface model of GI tract. Likewise, about 100 surface models of other neighboring structures were prepared. The surface models are expected to encourage other investigators to develop medical training systems such as virtual abdominal operation. Additionally, the improved technique of outlining and surface reconstruction is expected to inspire other investigators to easily make their own surface models from other serial images.
Key words: Surface models, Gastrointestinal tract, Visible Korean Human, Outlining, Surface reconstruction, Abdominal structures
TABLE OF CONTENTS
ABSTRACT ··· 1 TABLE OF CONTENTS ···2 LIST OF FIGURES ··· 3 LIST OF TABLES ··· 5 Ⅰ. INTRODUCTION ··· 6 . Ⅱ MATERIALS AND METHODS ··· 9. Ⅲ RESULTS ··· 19 . Ⅳ DISCUSSION ··· 21 . Ⅴ CONCLUSION ··· 26 REFERENCES ··· 27 국문요약 ···29
LIST OF FIGURES
Fig. 1. Both mural and luminal outlines of stomach (left), mural outline of
large intestine (center), and luminal outline of common bile duct (right)---9 Fig. 2. Gastrointestinal tract on paper, which is denoted with direction signs ---11 Fig. 3. A serially sectioned image (top left), which was filtered by
‘sharpen’ filter to clarify mural outline of small intestine (top right), and an another one (bottom left), which was filtered by ‘median’ filter to clarify
outline of bone (bottom right) ---12 Fig. 4. Segmented images with the outlines manually drawn (left, right) and
with the outlines interpolated (two centers) ---13 Fig. 5. Schematic showing that gastrointestinal tract is divided into
descending parts (red), ascending parts (blue), inferiorly curved parts (yellow), superiorly curved parts (green), and horizontal parts (light blue) (left).
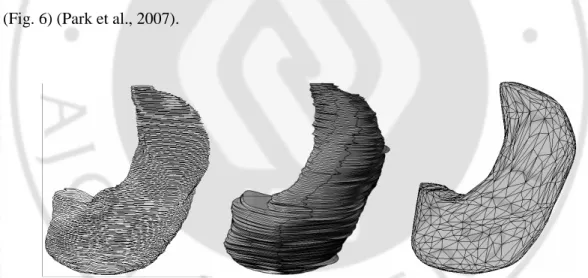
The divided parts were united (right) ---14 Fig. 6. Stacked outlines of stomach (left), surface model with the stacked outlines
Fig. 7. Surface models of gastrointestinal tract, stomach, duodenum, jejunum,
ileum, large intestine, and assembled gastrointestinal tract (from left to right) ---16 Fig. 8. Assembled surface models of the gastrointestinal tract and neighboring
structures, which are selected to display by layer window on Maya ---17 Fig. 9. Volume model of the gastrointestinal tract, which is rotated ---18 Fig. 10. Surface model of the stomach, superimposed upon the serially sectioned images --22
LIST OF TABLES
Table 1. Gastrointestinal tract and neighboring abdominal structures, which are
Ⅰ
Ⅰ
Ⅰ
Ⅰ. INTRODUCTION
Surface models, are empty three-dimensional images consisting of only surfaces, and have much smaller file size than volume models. Therefore, the surface model of the gastrointestinal (GI) tract accompanied by those of neighboring abdominal structures can be opened and rotated on the computer in a real time, and would be helpful in understanding the anatomy of digestive system. Moreover, the surface model of the GI tract can be used as the source for medical training such as virtual abdominal operation. The surface models have been stereoscopically drawn from the artistic skill accompanied by anatomy knowledge. However, it would be better to make the objective surface models from the scientific data as follows: Structures are outlined in the serial images of abdomen, and after stacking the outlines, gaps between the outlines are filled with polygons, which is the surface reconstruction.
Unfortunately, however, whole length of the GI tract cannot be outlined in the computed tomographs (CTs) or magnetic resonance images (MRIs) of abdomen, even if a part of the lumen of GI tract can be outlined by the support of contrast medium or gas. Peritoneotomograph is not the solution for outlining the GI tract. Moreover in the clinical images of living persons, GI tract tends to be obscure because of its own movement and lung movement. Consequently, the serially sectioned images of cadavers such as the Visible Human Project data have to be used for outlining the GI tract. In order to outline the GI tract,
the serially sectioned images have definite advantage of high resolution and real color. A minor problem of the Visible Human Project is that its data have missing images in the upper abdomen because cadavers are divided by a saw prior to serial sectioning. Therefore, we considered the use of using the Visible Korean Human (VKH) data without missing images. The VKH data have another merit to include good quality of serially sectioned images with 0.2 mm pixel size, smaller than 0.33 mm pixel size of the Visible Human Project data (Spitzer et al., 1996; Park et al., 2005a; Park et al., 2006).
Even though VKH data are the good choice, it is extremely difficult to identify whole length of the GI tract without cease in the serially sectioned images. It is because the GI tract with irregular contours is dramatically curved many times, and the small intestinal wall is narrow without feces and compressed in many parts. Therefore, even medical experts with anatomy knowledge have to append time for the identification. In addition, there is time-consuming problem for outlining and technical difficulty for surface reconstruction of the complicated GI tract. In order to solve these problem, we improved the technique of the outlining and surface reconstruction on the commercial software, which had previously been developed (Park et al., 2007). The surface model of the GI tract would be more valuable if it was accompanied surface models by those of neighboring structures such as other digestive organs and portal triad. Therefore, we tried to make as many surface models of structures in abdomen as possible (Moore & Dalley, 2006). Of course, we must keep the original shape and proper location of the structures in the surface models.
Purposes of this research are to present the surface models of the GI tract and neighboring structures, which can be applied to medical training system of abdomen for medical students or doctors, and also to present the improved technique of outlining and surface reconstruction, which can be applied to making other surface models from serial images.
Ⅱ
Ⅱ
Ⅱ
Ⅱ. MATERIALS AND METHODS
Serially sectioned images of a male cadaver’s whole body had been acquired at 0.2 mm intervals (pixel size, 0.2 mm; resolution, 3,040 X 2,008) in our previous studies (Park et al., 2005a; Park et al., 2006). Among the serially sectioned images of whole body, 412 serially sectioned images of abdomen, pelvis, and perineum including GI tract were chosen at 1 mm intervals.
Sixty-eight structures, including GI tract and neighboring structures, were selected to segment. Pipe-like structures had two outlines, i.e. mural and luminal outlines. We decided to draw the mural outlines of whole GI tract, and additionally to draw the luminal outlines of esophagus, stomach, and duodenum for virtual endoscopy. We also made decision to draw the luminal outlines of pancreatic duct, bile duct, and blood vessels, which were more distinct than the mural outlines of those (Fig. 1) (Table 1).
Fig. 1. Both mural and luminal outlines of stomach (left), mural outline of large intestine (center), and luminal outline of common bile duct (right).
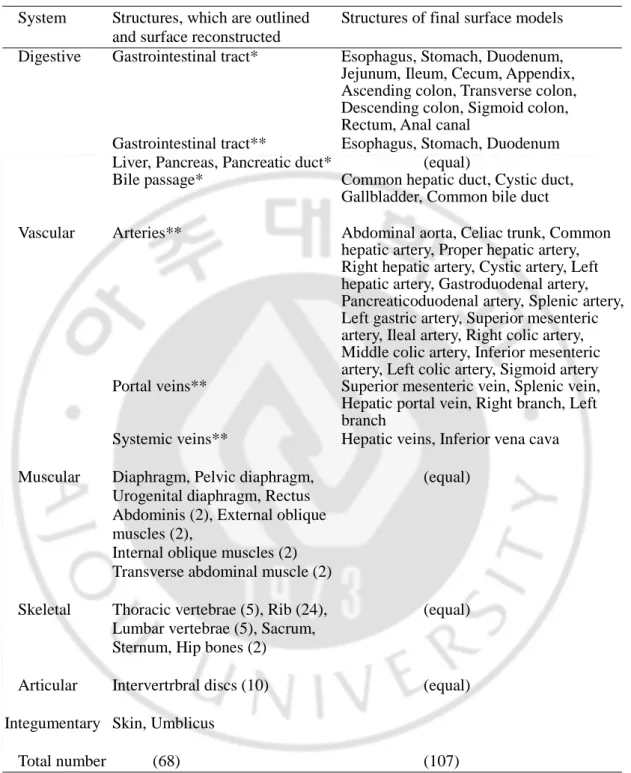
Table 1. Gastrointestinal tract and neighboring abdominal structures, which are outlined, surface reconstructed, and those in the final surface models.
System Structures, which are outlined Structures of final surface models and surface reconstructed
Digestive Gastrointestinal tract* Esophagus, Stomach, Duodenum, Jejunum, Ileum, Cecum, Appendix, Ascending colon, Transverse colon, Descending colon, Sigmoid colon, Rectum, Anal canal
Gastrointestinal tract** Esophagus, Stomach, Duodenum Liver, Pancreas, Pancreatic duct* (equal)
Bile passage* Common hepatic duct, Cystic duct, Gallbladder, Common bile duct
Vascular Arteries** Abdominal aorta, Celiac trunk, Common hepatic artery, Proper hepatic artery, Right hepatic artery, Cystic artery, Left hepatic artery, Gastroduodenal artery, Pancreaticoduodenal artery, Splenic artery, Left gastric artery, Superior mesenteric artery, Ileal artery, Right colic artery, Middle colic artery, Inferior mesenteric artery, Left colic artery, Sigmoid artery Portal veins** Superior mesenteric vein, Splenic vein, Hepatic portal vein, Right branch, Left branch
Systemic veins** Hepatic veins, Inferior vena cava Muscular Diaphragm, Pelvic diaphragm, (equal)
Urogenital diaphragm, Rectus Abdominis (2), External oblique muscles (2),
Internal oblique muscles (2) Transverse abdominal muscle (2)
Skeletal Thoracic vertebrae (5), Rib (24), (equal) Lumbar vertebrae (5), Sacrum,
Sternum, Hip bones (2)
Articular Intervertrbral discs (10) (equal)
Integumentary Skin, Umblicus
Total number (68) (107)
Mural outlines of the structures* are drawn while luminal outlines of the structures** are drawn.
First, GI tract, the main subject in this research, was outlined and surface reconstructed as follows.
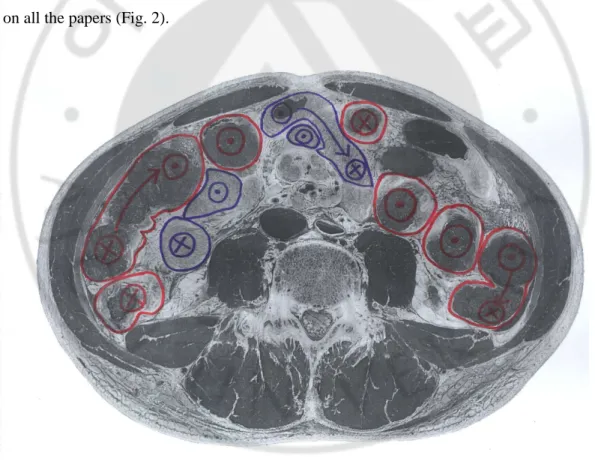
It was extremely difficult to identify complete length of GI tract in spite of high quality of the serially sectioned images with 0.2 mm pixel size and 24 bit color. Therefore, we had no choice but the following procedures: each serially sectioned image was printed out on paper. On the papers, GI tract was traced either from proximal to distal or reversely by referring to atlases of serially sectioned images (Spitzer et al., 1998; Dean et al., 2000). The every identified GI tract was denoted on the papers with signs, indicating the proximal to distal direction. It was performed with trials and errors until the entire GI tract was denoted on all the papers (Fig. 2).
Referring to the denoted papers, mural outlines of GI tract had to be drawn on the computer. Even though some mural outlines were distinct in the serially sectioned images especially thanks to visceral peritoneum, mural outlines could not be drawn to high automation extent. To enhance automation, the serially sectioned images were filtered on Autodesk Combustion version 4 (Combustion) with ‘sharpen’ filter to make the mural contours more distinct. It was found that the ‘sharpen’ filtering was good for outlining GI tract and muscles, while ‘median’ filtering was good for outlining bones, ducts, blood vessels, and skin (Fig. 3).
Fig. 3. A serially sectioned image (top left), which was filtered by ‘sharpen’ filter to clarify mural outline of small intestine (top right), and an another one (bottom left), which was filtered by ‘median’ filter to clarify outline of bone (bottom right).
Morphological feature of the GI tract gradually change along the neighboring serially sectioned images with 1 mm intervals. Therefore, in order to reduce tedious work for outlining the GI tract, we interpolated. For example, a part of GI tract was outlined in two serially sectioned images with 10 mm intervals; the outlining was done with enhanced automation by the preprocess of ‘sharpen’ filtering (Figs. 1, 3). On Combustion, interpolation was performed to create nine intervening outlines with 1 mm intervals by using ‘animate’ tool (Fig. 4). In cases where the created outlines were not fit for the GI tract in the serially sectioned images, the outlines were manually revised. Unfortunately, the outlines created could not be saved as Photoshop data (PSD) file format, which was necessary for the next procedure; surface reconstruction. Therefore, inside and outside of each outline was filled with black and white, respectively, and saved as tag image file format (TIFF). On Adobe Photoshop CS3 version 10 (Photoshop), the outline was revived using ‘magic wand’ tool.
Fig. 4. Segmented images with the outlines manually drawn (left, right) and with the outlines interpolated (two centers).
The GI tract, which in curved too often, could not be surface reconstructed at once. Therefore, the GI tract was divided into several parts; descending parts, ascending parts, inferiorly curved parts, superiorly curved parts, and horizontal parts, and each part should not have dividing region. Outlines of the GI tract were grouped by parts in order to make surface model of each part in the next procedure (Fig. 5).
Fig. 5. Schematic showing that gastrointestinal tract is divided into descending parts (red), ascending parts (blue), inferiorly curved parts (yellow), superiorly curved parts (green), and horizontal parts (light blue) (left). The divided parts were united (right).
Surface reconstruction of stomach, the first descending part of GI tract, was done as follows: On Photoshop, only outlines of the stomach were kept and converted from bitmap outlines to vector outlines; the vector outlines were saved as Adobe Illustrator (AI) file format. On Alias Maya version 7 (Maya), the vectorized outlines of the stomach were stacked using Maya script, while its proper location and horizontal-vertical proportion were kept. On Rhinoceros Rhino version 4 (Rhino), gaps between the stacked outlines were filled with polygons using ‘loft’ command to make surface model of the stomach. On Maya again, stacked outlines of the surface model were deleted using ‘smooth’ command; polygons of the surface model were reduced in number using ‘reduce’ command to refine the surface model. Incorrect portions of the surface model, which were caused by incorrect segmentation, were manually revised until the surface model corresponded to anatomy knowledge of stomach (Fig. 6) (Park et al., 2007).
Fig. 6. Stacked outlines of stomach (left), surface model with the stacked outlines preserved (center), and surface model with the stacked outlines deleted (right).
In the same manner, the surface models of the other parts of GI tract were made. On Maya, surface models of all parts, which kept their proper locations, were united using ‘union’ command to make a surface model of the whole GI tract (Figs. 5, 7).
Fig. 7. Surface models of gastrointestinal tract, stomach, duodenum, jejunum, ileum, large intestine, and assembled gastrointestinal tract (from left to right).
On Maya, the surface model of the whole GI tract was divided into thirteen surface models of named structures; i.e., esophagus, stomach, duodenum, jejunum, ileum, cecum, appendix, ascending colon, transverse colon, descending colon, sigmoid colon, rectum, and anal canal by using ‘cut faces’ tool (Fig. 7; Table 1).
We just described above the procedures for outlining and surface reconstruction of the GI tract. Using the same procedures, luminal surface models of the esophagus, stomach, and duodenum were made. Furthermore, surface models of the all other structures were also made. For an example, all identifiable bile passages were outlined and surface was reconstructed to make a surface model; the surface model was divided into four surface models of the common hepatic duct, cystic duct, gallbladder, and common bile duct (Table 1).
In a Maya file, Maya binary (MB) file format, 107 layers were made and each layer was named according to the structures' names, which followed Terminologia Anatomica (Table 1) (FCAT, 1988; Moore & Dalley, 2006). Surface model of each structure was put into its own layer to make the assembled surface models (Fig. 8).
Fig. 8. Assembled surface models of the gastrointestinal tract and neighboring structures, which are selected to display by layer window on Maya.
As the preprocess of volume reconstruction, both intervals and pixel size of the serially sectioned images were increased from 0.2 mm to 1 mm, and outside of GI tract in the serially sectioned images was automatically erased on Photoshop using the segmented images. On 3D-Doctor software version 3.5, the serially sectioned images were stacked and reconstructed by volume modeling to acquire a volume model of GI tract with 1 mm voxel size and real color, and it was then rotated (Fig. 9).
Ⅲ
Ⅲ
Ⅲ
Ⅲ. RESULTS
GI tract from stomach to anal canal were traced without cease and denoted on papers. It was possible because we used the serially sectioned images of high quality with 0.2 mm pixel size and 24 bit color (Fig. 2).
Segmentation was performed more automatically by filtering. By ‘sharpen’ filtering, color difference of GI tract and muscles was increased. By ‘median’ filtering, color numbers of bones, ducts, blood vessels, and skin were reduced (Fig. 3). As a result, segmentation could be done rapidly and correctly.
Segmentation was performed more automatically by interpolation (Fig. 4). In case of the vertically running structures, which were slowly changing along the horizontal serial images, interpolation could be done even to create 19 intervening outlines. As a result, effort and time for outlining could greatly be reduced. On the other hand, in case of the horizontally running structures, which abruptly change along the horizontal serial images, interpolation was hardly possible.
One-hundred seven final surface models of GI tract and neighboring structures were prepared (Table 1). The surface model of the highly curved GI tract could be made by grouping outlines of parts (Fig. 5), surface reconstruction of the parts, and uniting surface models of the parts. Moreover, the surface model of the GI tract could be divided into surface models of meaningful parts (Fig. 7).
The surface models maintained original shape and proper position of structures, so that the stereoscopic morphology and locational relationship of the structures could be observed
and more branches than the right and intermediate hepatic veins. These surface models could be distributed, opened, rotated, and modified in a real time because of small file size (50 MBytes).
Ⅳ
Ⅳ
Ⅳ
Ⅳ. DISCUSSION
To our kept knowledge, this is the first trial to make objective surface models of the whole GI tract and neighboring abdominal structures from the serially sectioned images. With these procedures, we were able to identify the structures, particularly all length of the GI tract in the serially sectioned images after trials and errors. We outlined 68 structures in 412 serially sectioned images with 1 mm intervals. We also performed surface reconstruction of all the structures; we did unification and division of the surface models.
In medical imaging field, volume and surface models compensate with each other. Medical doctors usually prefer the volume models to the surface ones because the volume models involve much more information; the volume models can be sectioned in arbitrary directions to show the sectional planes (Fig. 9). For a clinical example, the volume models are made of for abdominal CTs to diagnose digestive diseases and to plan abdominal surgery. However, the volume models have a problem of too large file size to easily handle. In contrast, the surface models with small file size (MB file format) can be distributed, opened, rotated, and modified in a real time (Uhl et al., 2006); it can be done in a real time even on-line; and can be performed without functional restriction on the popular commercial software (Fig. 8). In general, the volume models, welcomed by medical experts, are fit for clinics, while the surface models, welcomed by common persons or medical beginners, are fit for medical education and surgical training.
Another advantage of the surface models is that the surface models can easily be divided into meaningful parts. For an example, it is hardly possible to distinguish the
in the volume model of small intestine (Fig. 9). On the other hand, the jejunum and ileum are easily distinguished in the surface model, where whole length of small intestine is continuous, on the basis of simple anatomy knowledge that length ratio of jejunum and ileum is 2:3. Then, surface models which distinguish jejunum and ileum can be acquired and also surface models of all named parts of the digestive tract can be obtained (Fig. 7). Likewise, after making a surface model of all arteries related with digestive tract, the surface model can be divided into those of several named arteries such as celiac trunk, superior and inferior mesenteric arteries (Table 1).
One more advantage of the surface models made in the present study is that the surface models can be superimposed either upon the serially sectioned images, the source of the surface models themselves (Fig. 10) or upon the volume models. This trial is valuable, especially when users need more information about the surface models.
Fig. 10. Surface model of the stomach, superimposed upon the serially sectioned images.
The surface models of the GI tract and neighboring structures, which will be distributed free of charge, are expected to promote the various kinds of medical training system, which must be equipped with high levels of software and hardware. On the medical training systems such as virtual diagnosis and treatment, users should follow every procedure
models. Three examples of the virtual diagnosis and treatment of abdomen are suggested as follows.
Virtual gastrojejunostomy can be done, based on the surface models of skin, abdominal muscles, stomach, jejunum, and arteries (Table 1). Skin and abdominal muscles are incised to approach peritoneal cavity. Stomach and jejunum are incised and anastomosed; at this time, branches of celiac trunk and superior mesenteric artery are minded.
Virtual laparoscopic cholecystectomy can be done, based on the surface models of skin, gallbladder, cystic duct, portal triad and its branches (Table 1). Skin is perforated to insert laparoscope into peritoneal cavity. Using the laparoscope's instruments, cystic duct and cystic artery are cut to resect gallbladder; at this time, portal triad is carefully preserved, particularly right hepatic artery.
Virtual endoscopic retrograde cholangiopancreatography (ERCP) can be done, based on the luminal surface models of esophagus, stomach, duodenum, bile duct, and pancreatic duct (Table 1). Endoscopic tip passes sequential lumina of esophagus, stomach, and duodenum to be placed on the major duodenal papilla. From the endoscopic tip, contrast medium is injected into bile and pancreatic ducts to take their radiograph.
Besides the medical training system, other educational tools could also be made with the surface models. An example is to show embryonic development of GI tract. We have already prepared the surface model of GI tract, which is the end of the development. However, we can easily make the surface model of midgut and hindgut, which is the start of the development. Based on the embryology knowledge and computer technique, we can make an educational tool to show the stereoscopic and gradual change from the start to the
On the present study, we improved the technique of outlining and surface reconstruction. The technique just effectively usage of commands of the commercial software: Combustion, Photoshop, Maya, and Rhino. Using the improved technique, other investigators may try to make other surface models from the serial images such as CTs and MRIs on the personal computer. The commercial software has a merit that any investigators can do the outlining and surface reconstruction without the help of computer programmer; the investigators can use powerful and user-friendly commands of the commercial software without bug; end users can open and modify the surface models of final results (50 MB file format) on the commercial software.
By using this technique, outlining and surface reconstruction are expected to be done more automatically without problem as follows.
Outlining can be done more automatically after filtering the serially sectioned images on Combustion. Unlike CTs and MRIs, serially sectioned images have real color of human body, which is good for identification of structures. However, the real color does not mean clear demarcation of the structures' contours, which is one of the reasons of time consuming for outlining (Park et al., 2005a). To enhance automatization of outlining, we tried various kinds of filtering of the serially sectioned images and we eventually found that different filtering is suitable for different structure in the serially sectioned images (Fig. 3). It would be valuable to kind other kinds of filtering as well as to modify brightness and contrast for highlighting the different kinds of structures in the color images.
Outlining can be done more automatically by interpolation on Combustion. In this research, intervals of final segmented images were 1 mm, which is another reason of time
gradually along serially sectioned images. Therefore, we thought that the gradual changed can be covered by an image processing, interpolation. The interpolation can be executed on the commercial software without programming (Fig. 4). It would be a good change to continue the interpolation to create segmented images at 0.2 mm intervals, which are the same intervals of the serially sectioned images. These fine segmented images must have contributed to surface and volume models of good quality.
Surface reconstruction of whole GI tract can be done with no problem by dividing the GI tract into several parts on Maya and Rhino. Surface model of GI tract, which is curved too many times, cannot be made once at all. Therefore, before surface reconstruction, the GI tract is divided into several parts, including descending, ascending, inferiorly curved, superiorly curved, and horizontal parts. After surface reconstruction of each part with its outlines, surface models of all parts are united to make a surface model of whole length of GI tract. Successively, the surface model is divided into named parts; i.e., esophagus, stomach, and so on (Fig. 7). The technique for uniting and dividing of the surface models, tried in this research, would hopefully be utilized for many purposes in the medical imaging.
One-hundred seven surface models of the GI tract and neighboring structures, prepared in this research, will widely be presented to encourage other investigators to apply them in medical learning field. Concurrently, the presently improved technique of outlining and surface reconstruction, is expected to stimulate other investigators to easily make their own surface models from other serial images.
Ⅴ
Ⅴ
Ⅴ
Ⅴ. CONCLUSION
This research is One-hundred seven structures of digestive system were decided to segment in segmented images and including anatomical images. And one-hundred seven structures in digestive system were decided to semi-automatic surface reconstruction on the commercial software.
The segmentation techniques of this research can be used to segment many structures in other images quickly and correctly. These technical modifications of existing software will provide new solutions in medical education and research. Also, in this research, method of semi-automatic surface reconstruction on commercial software was developed. The method could enable other researchers to do surface reconstruction quickly and objectively for making 3D images.
REFERANCES
1.
Dean D, Herbener TE: Cross-Sectional Human Anatomy. Baltimore, MD:
Lippincott Williams & Wilkins, 2000
2.
FCAT (Federative Committee on Anatomical Terminology): Terminologia
Anatomica, International Anatomical Terminology, Tieme, Stuttgart, New
York, 1998
3.
Moore KL, Dalley AF: Clinically Oriented Anatomy, 5th ed., Lippincott
Williams & Wilkins, Philadelphia, 2006
4.
Park JS, Chung MS, Hwang SB, Lee YS, Har DH, Park HS: Visible Korean
Human. Improved serially sectioned images of the entire body. IEEE Trans
Med Imaging 24: 352-360, 2005a
5.
Park JS, Chung MS, Hwang SB, Lee YS, Har DH: Technical report on
semiautomatic segmentation by using the Adobe Photoshop. J Digit Imaging
18: 333-343, 2005b
6.
Park JS, Chung MS, Hwang SB, Shin BS, Park HS: Visible Korean Human.
Its techniques and applications. Clin Anat 19: 216-224, 2006
7.
Park JS, Shin DS, Chung MS, Hwang SB, Chung J: Technique of
semiautomatic surface reconstruction of the Visible Korean Human data by
using commercial software. Clin Anat 20: 871-879, 2007
8.
Spitzer VM, Ackerman MJ, Scherzinger AL, Whitlock DG: The Visible
Human male. A technical report. J Am Med Inform Assoc 3: 118-130, 1996
9.
Spitzer VM, Whitlock DG: Atlas of the Visible Human Male. Reverse
Engineering of the Human Body. Massachusetts: Jones and Bartlett
10.
Uhl JF, Park JS, Chung MS, Delmas V: Three-dimensional reconstruction of
urogenital tract from Visible Korean Human. Anat Rec Part A 288A: 893-899,
2006
- 국문요약 -