Different Hip Rotations Influence Hip
Abductor Muscles Activity During Side-lying
Isometric Hip Abduction in Subjects With
Gluteus Medius Weakness
Jihyun Lee
The Graduate School
Yonsei University
Different Hip Rotations Influence Hip
Abductor Muscles Activity During Side-lying
Isometric Hip Abduction in Subjects With
Gluteus Medius Weakness
Jihyun Lee
The Graduate School
Yonsei University
Different Hip Rotations Influence Hip
Abductor Muscles Activity During Side-lying
Isometric Hip Abduction in Subjects With
Gluteus Medius Weakness
A Masters Thesis
Submitted to the Department of Physical Therapy
and the Graduate School of Yonsei University
in partial fulfillment of the requirements
for the degree of Master of Science
Jihyun Lee
June 2013
This certifies that the master’s thesis of
Jihyun Lee is approved.
Thesis Supervisor: Heonseock Cynn
Chunghwi Yi: Thesis Committee Member #1
Ohyun Kwon: Thesis Committee Member #2
The Graduate School
Yonsei University
Acknowledgements
First of all, I would like to thank supervisor Professor Heonseock Cynn. He fully trusted me and gave me an opportunity to restart studying in the master’s course. His advice was a great encouragement to me academically and socially. I feel honored to have met him and learnt from him. He is an eternal teacher and a mentor to me. I wish to thank Professor Chungwhi Yi, he provided prudent comments that helped improve the quality of my thesis. I also would like to express my gratitude to Professor Ohyun Kwon, he gave me an opportunity to study about orthopedic field academically and clinically. I was able to expand my knowledge through his lesson and advice. I gladly express my gratitude to Professor Sanghyun Cho, he taught me how to use valuable technical skills to improve my thesis and presentation. I deeply thank Professor Hyeseon Jeon, who gave me warm advice and encouragement. I was able to treat children effectively in my working field. I sincerely thank Professor Sunghyun Yoo for providing encouragement. I express my deepest gratitude for all your teachings.
I would like to thank all members of the applied kinesiology and ergonomic technology laboratory. Especially, my senior, Taelim Yoon, I was able to finish the articles with his intellectual support and guide. Kyungmi Park, she helped me adapt to school life in the beginning of the course and she motivated me to research continuously. Sila Choi, she carried out many experiments with me and supported me. I was able to learn how to write academic articles through the experiments and articles. Woojung Chol, she always
greeted me with a friendly smile in the lap and helped me to perform experiments for the thesis, Hyojeong Jung, who tried to help experiments in the lap and truly looked for subjects for the thesis. I wish to give my appreciation to all students of the graduate school department of Physical Therapy. Especially, Kyunghoon Yu and Namgi Lee, who supported me and gave me encouragement and advice honestly, Yoonkyum Shin was always with me for the school life and she prayed for me even though she left the school earlier. I did not feel alone in the school with you. Thank you so much my sister. I wish you achieve a great work.
I would like to thank Eunkyung Park, Yoonmi Lee, and all members of cell church. They supported me and imparted spiritualized wisdom. They hold me whenever I displayed considerable irresolution. I deeply thank to my best friend, Unju Lee, she was always with me in a difficult situation, especially when I could not find subjects for an experiment in the beginning of the master’s course. She was considerate of my feelings all the time
I deeply thank to my family, Haengman Lee, Youngae Lee, Jungjin Lee, Ahram Park, Soonhee Jung, Pyoungho Gug, and my husband Yunjai Gug. They had patient and understood me for a long time and supported me emotionally and financially. Their affection is beyond word. I love you so much. I will reward you with my good results.
Finally, I thank and praise God. I was very glad for his guidance and support that has enabled me to finish my master’s course. I was able to study in a settled frame of mind
through Isaiah 41:10 which “So do not fear, for I am with you; do not be dismayed, for I am your God. I will strengthen you and help you. I will uphold you with my righteous right hand.”
Table of Contents
List of Figures ··· iii
List of Tables ··· iv Abstract ··· v Introduction ··· 1 Methods ··· 4 1. Subjects ··· 4 2. Instrumentation ··· 6 2.1 Surface Electromyography ··· 6
2.2 Three-dimensional Ultrasonic Motion Analysis System ··· 9
2.3 Hand Held Dynamometer ··· 10
3. Experimental Procedures ··· 11
3.1 Side-lying Hip Abduction With Neutral Hip ··· 14
3.2 Side-lying Hip Abduction With Hip Medial Rotation ··· 15
3.3 Side-lying Hip Abduction With Hip Lateral Rotation ··· 16
4. Statistical Analysis ··· 17
Results ··· 18
1. Subjects ··· 18
2. Electromyographic Data ··· 20 2.1 Gluteus Maximus, Gluteus medius, and Tensor Fasciae Latae
Muscle Activity ··· 20
2.2. Gluteus Maximus/Tensor Fasciae Latae, Gluteus medius/Tensor Fasciae Latae, and Gluteus medius/Gluteus Maximus Muscle Activity Ratios ··· 21
Discussion ··· 25
Conclusion ··· 29
References ··· 30
- iii -
List of Figures
Figure 1. Location of Vertical Plastic Guides ··· 13
Figure 2. Hip Abduction Exercise With Neutral Hip in Side-lying ··· 14
Figure 3. Hip Abduction Exercise With Hip Medial Rotation in Side-lying ··· 15
Figure 4. Hip Abduction Exercise With Hip Lateral Rotation in Side-lying ··· 16
Figure 5. Comparison of Muscle Activity in the Gluteus Maximus, Gluteus Medius, and the Tensor Fasciae Latae Among Different Hip Rotations During Side-lying Hip Abduction Exercises ··· 23
Figure 6. Comparison of Muscle Activity Ratio in the Gluteus Maximus, Gluteus Medius, and the Tensor Fasciae latae Among Different Hip Rotations During Side-lying Hip Abduction Exercises ··· 24
- iv -
List of Tables
Table 1. Demographic Characteristics of Subjects ··· 19 Table 2. Comparison of Muscle Activity in the Gluteus Maximus, Gluteus Medius, and Tensor Fasciae Latae Among Different Hip Abduction Exercises · 22
- v -
ABSTRACT
Different Hip Rotations Influence Hip Abductor Muscles
Activity During Side-lying Isometric Hip Abduction in
Subjects With Gluteus Medius Weakness
Jihyun Lee
Dept. of Physical Therapy The Graduate School Yonsei University
Gluteus medius (Gmed) weakness is related to several lower extremity injuries. People with Gmed weakness often compensate by activating the tensor fasciae latae (TFL). A dominant TFL can force hip medial rotation and lateral patellar displacement, which can cause related patellofemoral pain. Meanwhile, the Gmed and gluteus maximus (Gmax) control excessive hip medial rotation and adduction of the hip during a gait. Different hip rotations in the transverse plane may affect Gmax, Gmed, and TFL muscle activity through side-lying hip abduction (SHA). The aim of this study was to establish the effects of different hip rotations on Gmax, Gmed, and
- vi -
TFL muscle activity and the muscle activity ratio of the Gmax/TFL, Gmed/TFL, and Gmed/Gmax during isometric SHA in subjects with Gmed weakness.
The study recruited nineteen subjects with Gmed weakness. Subjects performed isometric SHA: frontal SHA with neutral hip (SHA-N), frontal SHA with hip medial rotation (SHA-MR), and frontal SHA with hip lateral rotation (SHA-LR). Surface electromyography measured the activity of the Gmax, Gmed, and TFL. A one-way repeated-measures analysis of variance (ANOVA) assessed the statistical significance of Gmax, Gmed, and TFL muscle activity. A significant difference prompted a Bonferroni adjustment.
Gmed muscle activity was significantly greater in SHA-MR than in SHA-N. TFL muscle activity was significantly greater in SHA-LR than in SHA-N. The Gmed/TFL and Gmed/Gmax muscle activity ratios were also significantly greater in SHA-MR than in SHA-N or SHA-LR.
SHA-MR is the most effective exercise for greater Gmed muscle activation and a higher Gmed/TFL muscle activity ratio among three SHA exercises.
Key Words: Gluteus maximus, Gluteus medius, Hip rotation, Side-lying hip abduction, Tensor fasciae latae.
- 1 -
Introduction
Abnormal hip kinematics and impaired hip muscle performance have been associated with various musculoskeletal disorders (Selkowitz, Beneck, and Powers 2013). In particular, gluteus medius (Gmed) weakness has been related to patellofemoral pain syndrome and iliotibial-band friction syndrome (Cichanowski et al. 2007; Fredericson et al. 2002; Lee, Souza, and Powers 2012; Robinson and Nee 2007). Therefore, many therapeutic exercise protocols have focused on Gmed activity for prevention and rehabilitation in clinical and athletic training settings.
A side-lying hip abduction (SHA) exercise is recommended as an effective way to improve the Gmed muscles. Previous studies have reported using SHA to generate proper neuromuscular control early in a rehabilitation program, as an open-chain exercise, and to target Gmed muscle activity effectively (Distefano et al. 2009; McBeth et al. 2012). Selkowitz et al. (2013) demonstrated that only the Gmed exhibited significantly greater normalized electromyographic (EMG) amplitude than the tensor fasciae latae (TFL) during various exercises, such as clam, sidestep, and unilateral bridge.
When prescribing strengthening exercise for hip abductors, one should consider the relative activation of all muscles. The three primary hip abductors are well known. The Gmed is an abductor and lateral rotator and the TFL is an abductor and medial rotator at the hip (Gottschalk, Kourosh, Leveau 1989; Neumann 2010; Selkowitz,
- 2 -
Beneck, and Powers 2013). In addition, the upper portion of the gluteus maximus (Gmax) also acts as a hip abductor and lateral rotator in a gait (Blandine 1993; Lyons et al. 1983; Neumann 2010). Thus, the Gmax and Gmed control excessive hip medial rotation and adduction in ambulation (Delp et al. 1999: Lyons et al. 1983). However, the TFL is an abductor and medial rotator of the hip. Consequently, when a gait exhibits a movement pattern with excessive medial rotation, the TFL may be dominant or over-active as a hip abductor, compared to the Gmed (Sahrmann 2003). Over-active TFL can also put lateral force on the patella (Kwak et al. 2000; Merican and Amis 2009). This movement pattern has been associated with patellofemoral pain (Powers 2010). Atrophy of the Gmax muscle relative to the TFL has been detected in degenerative hip joint pathology (Grimaldi et al. 2009). Previous study reported the TFL was more active than the Gmed and Gmax during SHA with hip laterally rotated even when the researcher advocated the rationale that hip lateral rotation activated the Gmed and reduced the TFL as a medial rotator (McBeth et al. 2012).
A limitation of previous studies was that they evaluated Gmax, Gmed, and TFL muscle activity during SHA in healthy subjects; they did not investigate these muscle activities during SHA with different hip rotations in subjects with Gmed weakness. Therefore, examination of Gmax, Gmed, and TFL activation with different hip rotations during SHA in subjects with Gmed weakness will provide valuable, new information.
The purpose of this research was to establish the effects of SHA with different hip rotations in the frontal plane (frontal SHA with neutral hip, SHA-N; SHA with MR,
- 3 -
SHA-MR; and SHA with hip LR, SHA-LR) on Gmax, Gmed, and TFL muscle activity, and the muscle activity ratio of Gmax/TFL, Gmed/TFL, and Gmed/Gmax during isometric SHA in subjects with Gmed weakness. The hypothesis was that Gmax and Gmed muscle activity and the muscle activity ratios of the Gmax/TFL, Gmed/TFL, and Gmed/Gmax would increase and that TFL muscle activity would decrease in SHA-MR, compared with the other SHA exercises, in subjects with Gmed weakness.
- 4 -
Method
1. Subjects
G-power software provided power analyses. The necessary sample size of seven subjects was calculated from data obtained from a pilot study of seven subjects to achieve a power of 0.80 and an effect size of 0.40 (calculated by partial η2 of 0.14 from the pilot study), with an α level of 0.05. The current study had 19 subjects. A soccer-ball-kicking exercise established the dominant leg for each participant (Bolgla and Uhl 2005; McBeth et al. 2012).
Subjects were between 18 and 30 years of age. Inclusion criteria included being free from past or current inflammatory arthritis and lower-extremity or back dysfunction, and being able to maintain 5 seconds of isometric hip abduction in the side-lying position (Kim et al. 2011). Gmed weakness was confirmed by performing manual muscle testing with a hand-held dynamometer. Muscle grading was based on the method described by Florence Kendall (2005). Strength was graded as 0, 1, 2, 3, 4, or 5/5, then grouped as either ‘weak’ (3/5 or less) or ‘strong’ (4 or 5/5) (Bewyer et al. 2009). The study measured Gmed weakness twice and used the average measurement to qualify Gmed strength.
The study excluded subjects with past or present musculoskeletal, neurological, or cardiopulmonary diseases that could interfere with SHA. Additionally, using Craig’s
- 5 -
test, those with excessive femoral anteversion above 42° were excluded (Nyland et al. 2004). Overweight or obese subjects were also excluded, as fatty tissue, acting as a low-pass filter, could interfere with EMG signals (Wong 1999).‘Overweight’ and ‘obese’ were identified as a Body Mass Index >25 (Flegal et al. 1998).
Prior to the study, subjects signed a written consent form to participate. Yonsei University Wonju Campus Institutional Review Board approved the protocol for this study, and each volunteer gave informed consent prior to participation.
- 6 -
2. Instrumentation
2.1 Surface Electromyography
EMG data were collected from a Tele-Myo DTS EMG instrument with a wireless telemetry system (Noraxon, Inc., Scottsdale, AZ, U.S.A.). The sampling rate was 1000 Hz. A digital band-pass filter (Lancosh FIR), which filtered the raw signals, was between 20 and 450 Hz. Root-mean-square values were calculated with a moving window of 50 ms and Myo-Research Master Edition 1.06 XP software analyzed the EMG data.
An investigator prepared the electrode sites by shaving the subjects’ hair from the immediate vicinity of the muscle belly and cleaning the skin, using isopropyl alcohol with a sterile gauze pad to diminish impedance to the EMG signal; then, the electrodes were fixed on the proper sites (Hermens et al. 2000). Electrodes were positioned over the midsection of the muscle bellies, as in previous studies determining the sites of gluteal muscles (Ayotte et al. 2007; Bolgla and Uhl 2005) and detailed by Rainoldi et al. (2004). For the Gmax, two active electrodes were placed half the distance between the sacral vertebrae and the greater trochanter in the middle belly on an oblique angle at the level of the trochanter or slightly above it. For the Gmed muscle, electrodes were placed directly superior to the greater trochanter of the femur, one-third of the distance between the iliac crest and the greater trochanter of the femur. For the TFL muscle, electrodes were placed 2 cm inferior, and slightly
- 7 -
lateral, to the anterosuperior iliac spine (Cram, Kasman, Holtz 1998). Proper placement of the electrodes was confirmed by viewing the subjects while completing five repetitions of SHA. Electrode contacts were checked before all contractions (Cram, Kasman, Holtz 1998).
Maximal voluntary isometric contraction (MVIC) in the standard manual muscle-test position was used to normalize the Gmax, Gmed, and TFL (Kendall, McCreary, Provance 2005). To obtain the MVIC for the Gmax, the investigator tested each participant’s resistance to hip extension by having the subject lie fully prone, with the knee flexed to 90°, and applying a downward force at the posterior thigh. To obtain the MVIC values for the Gmed, subjects assumed a side-lying position on the treatment table with the test leg up and the bottom hip and knee flexed for stability. The test leg was abducted to approximately 50% of hip abduction, and the hip was placed in extension and slightly laterally rotated. An investigator applied downward force at the ankle while maintaining the hip with the other hand. To obtain the MVIC for the TFL, the subjects assumed a supine position on the treatment table with the hip flexed and slightly medially rotated with the knee extended. The investigator applied downward force at the ankle in the direction of the hip extension. Subjects performed the MVIC twice for the Gmax, Gmed, and TFL muscles. The mean value from the two trials was used for data analysis. Subjects performed for 5 seconds at MVIC with a 10 second rest between contractions. Subjects had a 3 minute rest between muscles tested (Soderberg and Knutson 2000). The EMG amplitudes collected during each exercise were expressed as a percentage of the average MVIC (%MVIC).
- 8 -
The muscle activity of the Gmax, Gmed, and TFL was collected during the SHA exercises in the frontal plane (SHA-N, SHA-MR, and SHA-LR), in randomized order; subjects drew lots to avoid learning effects or fatigue.
Every SHA exercise speed was comfortable to each participant. EMG data were collected for 5 seconds during the isometric phase and calculated from the middle 3 seconds of each exercise to avoid any skin-electrode connecting element and possible starting or ending effects (Ayotte et al. 2007; Soderberg and Knutson 2000). Subjects performed three trials under each SHA condition, with a 3 minute rest between exercises (Sykes and Wong 2003). The mean value was used for data analysis (De Luca 1997).
- 9 -
2.2 Three-dimensional Ultrasonic Motion Analysis System
The three-dimensional ultrasonic motion analysis system (CHS-HS, Zebris Medizintechnik GmbH, Isny im Allgau, Germany) calculated the hip rotation range of motion (ROM) of each subject and monitored compensatory pelvic movement (pelvic tilting in the sagittal plane, pelvic rotation in the horizontal plane, pelvic obliquity in the frontal plane) during SHA exercises. One triple marker was placed above the lateral femoral epicondyle to measure amounts of hip rotation (Kiss and Illyés 2012). The other was located on the midline of the pelvis by fastening a strap around the pelvis at the level of both posterior superior iliac spines to monitor pelvic movement (Oh et al. 2007; Park et al. 2011).
The measurement sensor, consisting of three microphones, was positioned to the back of the subject so that it faced the markers. The side-lying position with neutral hip rotation was calibrated to zero as a reference position. The sampling rate was 20 Hz.
SHA-MR and SHA-LR were calculated using 50% of the maximal ROM for each MR and LR. If the angle of hip rotation and pelvic movement exceeded 5°, the data were regarded as deviations and discarded.
- 10 -
2.3 Hand Held Dynamometer
The isometric strength of the Gmed was evaluated with a hand held dynamometer (hand held dynamometer, Lafayette instrument company, North Lafayette, USA), which measures static force from 0-199.9kg, with reported accuracy to 0.1kg ± 2% (Bohannon 1988; Marino, Nicholas, Gleim 1982). Several researchers have reported that the hand held dynamometer has good to excellent test-retest reliability for muscle testing in the lower extremities (Intraclass correlation coefficient = 0.82 to 0.98) (Bohannon 1999; Fenter et al. 2003; Heinert et al. 2008; Kimura et al. 1996; Nadler et al. 2000; Wang, Olson, Protas 2002).
- 11 -
3. Experimental Procedures
Before testing, subjects jogged for 5 minutes at a sub-maximal speed to warm up and to decrease possible discomfort or pain while performing SHA exercises (Hunter et al. 2003). To obtain Gmed strength, subjects assumed a side-lying position on the treatment table. A strap placed proximal to the iliac crest and secured around the table stabilized the pelvis. The bottom leg was flexed for comfort and stability, and the test leg was aligned with the rest of the trunk. The participant abducted the leg toward the ceiling. The hip of the test limb was abducted to 50% of the hip abduction total ROM and the dynamometer pad was placed 10 cm proximal to the lateral femoral epicondyle (Khayambashi et al. 2012). An isometric hold was performed for 5 seconds against resistance. The principal investigator (JHL) provided verbal encouragement to facilitate maximal performance and gave instructions to avoid any medial rotation or flexion of the hip through recruitment of the TFL or any hip hiking through use of the quadratus lumborum (Fredericson et al. 2002). Subjects took a 1 minute rest between the two trials (Friel et al. 2006). Strength was normalized to body weight by dividing the force recorded by the dynamometer by body weight in kilograms [force kg/ body weight kg × 100] (Khayambashi et al. 2012).
A modified Ober test measured the shortness of the iliotibial band. A normal iliotibial band would stretch when the hip adducted beyond 10°. If the iliotibial band was short, it did not allow the test leg to drop in adduction toward the table beyond 10°
- 12 -
(Kendall, McCreary, Provance 2005). The modified Ober test recorded hip adduction below the horizontal plane as a negative number and abduction above the horizontal plane as a positive number.
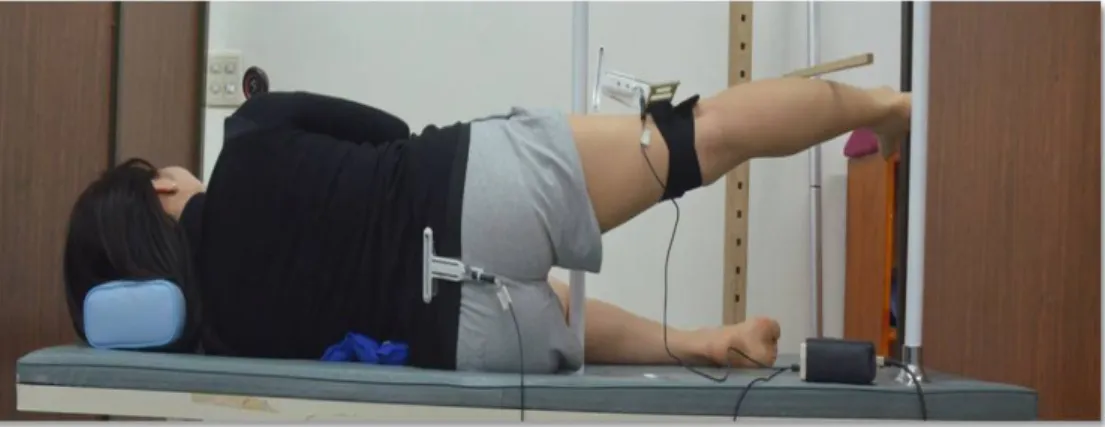
Plastic guides were aligned near the mid-thigh and heel to maintain the frontal plane during the SHA. If the anterior mid-thigh or the posterior heel touched the vertical plastic guides, the position was regarded as a deviation from frontal SHA, and the data were discarded (Figure 1).
The pressure biofeedback unit was placed between each participant’s lumbar spine and the treatment table with the participant in the side-lying position. The unit presented visual feedback to avoid unwanted changes in body position during SHA exercises. Using the pressure biofeedback unit can decrease compensation from the quadratus lumborum and prevent excessive lateral tilt of the lumbopelvic region in the frontal plane (Cynn et al. 2006). A familiarization period was necessary to use the pressure biofeedback unit effectively during SHA exercises. The principal investigator (JHL) explained how to use a pressure biofeedback unit with verbal cues. The participant had to maintain the pressure biofeedback unit until the pressure reached 40 mmHg during the SHA exercises, and the principal investigator (JHL) monitored pressure changes to ensure the maintenance of pressure between 35 and 45 mmHg (Cynn et al. 2006; McBeth et al. 2012). Each participant was pain free and comfortable with use of the pressure biofeedback unit after the familiarization period.
- 13 -
- 14 -
3.1 Side-lying Hip Abduction With Neutral Hip
Subjects lay on their sides with the upper trunk and pelvis aligned in a straight line on the treatment table. The bottom side hip joint could be flexed at 45° and knee joints were flexed at 90° for stabilization (Selkowitz, Beneck, and Powers 2013). A wooden target bar was placed at 50% of the hip abduction ROM, accommodating the ROM of each participant. Thus, the test leg was abducted to 50% of the maximal ROM with knee extension until the lateral aspect of the distal one-third of the fibula touched the target bar, maintained in the position for 5 seconds, and then, slowly returned to the starting position. The pressure biofeedback unit monitored the quadratus lumborum and the three-dimensional ultrasonic motion analysis system monitored compensatory pelvic movement during the 5 seconds period (Figure 2).
- 15 -
3.2 Side-lying Hip Abduction With Hip Medial Rotation
Subjects performed in the same way as in the SHA-N, excluding the hip medial rotation. The hip was rotated medially 50% of the total ROM. Subjects performed SHA-MR until the posterolateral aspect of the distal one-third of the fibula touched the target bar. The principal investigator monitored the ROM of MR during a 5 seconds period through the three-dimensional ultrasonic motion analysis system (Figure 3).
- 16 -
3.3 Side-lying Hip Abduction With Hip Lateral Rotation
Subjects performed the same way as in the SHA-N, except for the hip lateral rotation. The hip was rotated laterally 50% of the total ROM. The participant was asked to perform the SHA-LR until the anterolateral aspect of the distal one-third of the fibula touched the target bar. The principal investigator monitored the ROM of LR during a 5 seconds period through the three-dimensional ultrasonic motion analysis system (Figure 4).
- 17 -
4. Statistical Analysis
The PASW Statistics 18 software (SPSS, Chicago, IL, U.S.A.) performed all statistical analyses. Kolmogorov–Smirnov Z-tests assessed the normality of the distribution. A one-way, repeated-measures analysis of variance (ANOVA) assessed the statistical significance of the Gmax, Gmed, and TFL muscle activity and the Gmax/TFL, Gmed/TFL, and Gmed/Gmax muscle activity ratios during SHA exercises with three different hip rotations (SHA-N, SHA-MR, and SHA-LR). Statistical significance was set at 0.05. If a significant difference was found, a Bonferroni adjustment was performed (with α = 0.05 / 3 = 0.017).
- 18 -
Results
1. Subjects
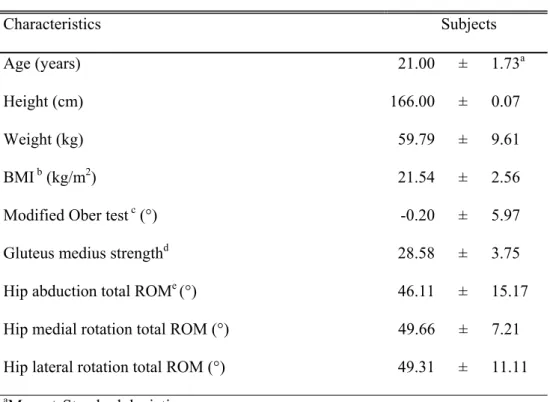
Table 1 shows the demographic characteristics of subjects, including height, weight, age, BMI, Gmed strength, and ROMs for hip abduction and medial and lateral rotations.
- 19 -
Table 1. Demographic characteristics of subjects (N = 19)
Characteristics Subjects
Age (years) 21.00 ± 1.73a
Height (cm) 166.00 ± 0.07
Weight (kg) 59.79 ± 9.61
BMI b (kg/m2) 21.54 ± 2.56
Modified Ober test c (°) -0.20 ± 5.97
Gluteus medius strengthd 28.58 ± 3.75
Hip abduction total ROMe (°) 46.11 ± 15.17
Hip medial rotation total ROM (°) 49.66 ± 7.21 Hip lateral rotation total ROM (°) 49.31 ± 11.11 aMean ± Standard deviation.
bBMI: Body mass index.
cHip adduction (below horizontal plane) was recorded as a negative number and abduction was recorded as a positive number.
dStrength data are kilogram of force divided by body weight (force kg/body weight kg × 100).
- 20 -
2. Electromyographic Data
2.1 Gmax, Gmed and TFL Muscle Activity
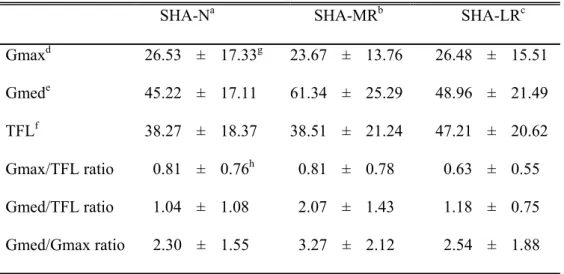
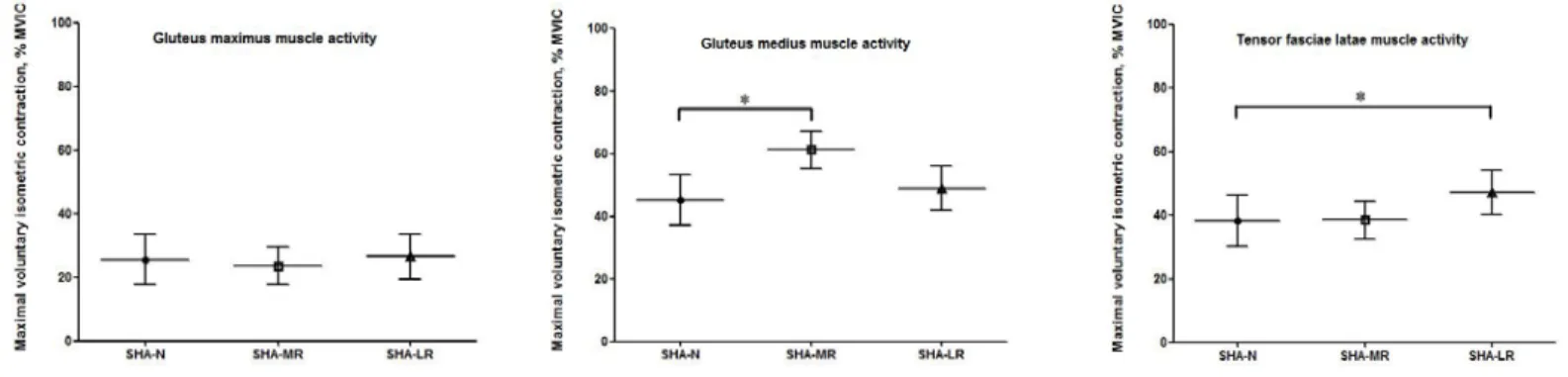
There was no significant difference in Gmax muscle activity among SHA-N, MR, and LR (F2, 17 = 2.286, p = 0.132). However, the study found significant differences in Gmed muscle activity (F2, 17 = 6.455, p = 0.009) and TFL muscle activity (F2, 17 = 3.965, p = 0.039) among the three hip abduction exercises. SHA-MR showed significantly greater Gmed muscle activity than SHA-N did (p = 0.003). SHA-LR produced significantly greater TFL muscle activity than SHA-N did (p = 0.010) (Table 2, Figure 5).
- 21 -
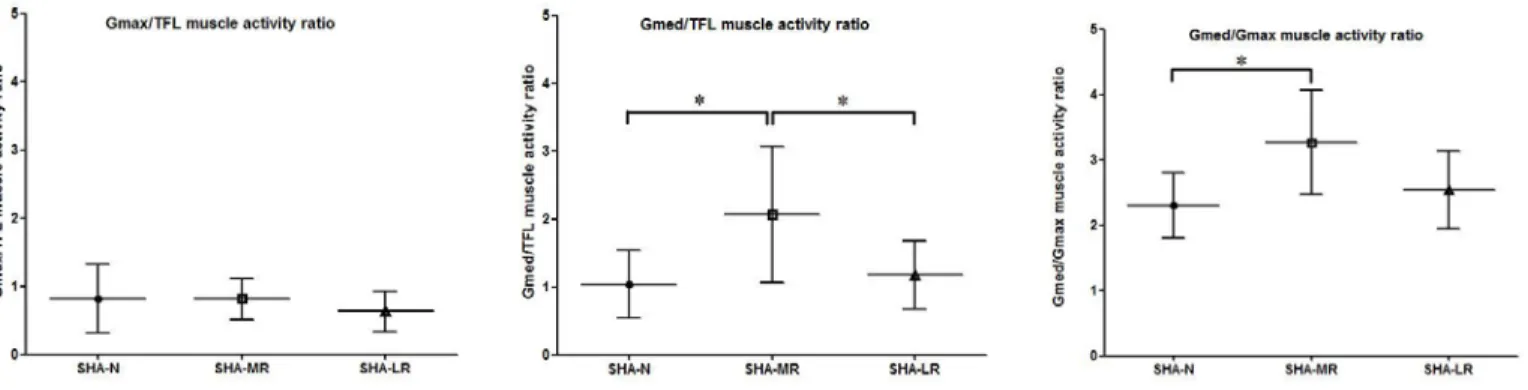
2.2 Gmax/TFL and Gmed/TFL Muscle Activity Ratios
There was no significant difference in the Gmax/TFL muscle activity ratio among SHA-N, MR, and LR (F2, 17 = 3.206, p = 0.066). However, there were significant differences in the Gmed/TFL muscle activity ratio (F2, 17 = 6.925, p = 0.006) and the Gmed/Gmax muscle activity ratio (F2, 17 = 6.769, p = 0.007) among the three hip abduction exercises. SHA-MR produced a significantly greater Gmed/TFL muscle activity ratio than did SHA-N (p = 0.001) and SHA-LR (p = 0.010). SHA-MR also resulted in a significantly greater Gmed/Gmax muscle activity ratio than did SHA-N (p = 0.002) (Table 2, Figure 6).
- 22 -
Table 2. Comparison of muscle activity in the gluteus maximus, medius and the tensor fasciae latae among different hip abduction exercises
SHA-Na SHA-MRb SHA-LRc Gmaxd 26.53 ± 17.33g 23.67 ± 13.76 26.48 ± 15.51 Gmede 45.22 ± 17.11 61.34 ± 25.29 48.96 ± 21.49 TFLf 38.27 ± 18.37 38.51 ± 21.24 47.21 ± 20.62 Gmax/TFL ratio 0.81 ± 0.76h 0.81 ± 0.78 0.63 ± 0.55 Gmed/TFL ratio 1.04 ± 1.08 2.07 ± 1.43 1.18 ± 0.75 Gmed/Gmax ratio 2.30 ± 1.55 3.27 ± 2.12 2.54 ± 1.88 aSHA-N: Side-lying hip abduction with neutral hip.
bSHA-MR: Side-lying hip abduction with hip medial rotation. cSHA-LR: Side-lying hip abduction with hip lateral rotation. dGmax: Gluteus maximus.
eGmed: Gluteus medius. fTFL: Tensor fasciae latae.
gMean ± Standard deviation of % maximal voluntary isometric contraction. hMean ± Standard deviation
- 23 -
Figure 5. Comparison of muscle activity in the gluteus maximus, medius, and the tensor fasciae latae among different hip rotations during side-lying hip abduction exercises.
SHA-N: Side-lying hip abduction with neutral hip.
SHA-MR: Side-lying hip abduction with hip medial rotation. SHA-LR: Side-lying hip abduction with hip lateral rotation.
- 24 -
Figure 6. Comparison of muscle activity ratio in the gluteus maximus, medius, and the tensor fasciae latae among different hip rotations during side-lying hip abduction exercises.
Gmax, Gluteus maximus. Gmed, Gluteus medius. TFL, Tensor fasciae latae.
SHA-N: Side-lying hip abduction with neutral hip.
SHA-MR: Side-lying hip abduction with hip medial rotation. SHA-LR: Side-lying hip abduction with hip lateral rotation.
- 25 -
Discussion
The purpose of the current study was to investigate whether Gmax, Gmed, and TFL muscle activity and Gmax/TFL, Gmed/TFL, and Gmed/Gmax muscle activity ratios would be different in different hip rotations during SHA exercises (SHA-N, SHA-MR, and SHA-LR) in subjects with Gmed weakness. The study found that Gmed muscle activity and the Gmed/TFL and Gmed/Gmax muscle activity ratios were significantly greater in SHA-MR than in SHA-N or SHA-LR in subjects with Gmed weakness. To the authors’ knowledge, this study is the first to examine the effects of different hip rotations in SHA exercise on the muscle activity of the hip abductors in subjects with Gmed weakness.
Gmed muscle activity was significantly greater in SHA-MR, compared to SHA-N (by 16.12%). Gmed muscle activity in SHA-MR was also greater, by 12.38%, when compared to SHA-LR; however, this difference was not statistically significant. These findings partially support our research hypothesis that Gmed muscle activity would increase more in SHA-MR, compared to other SHA exercises. The results are in accordance with previous results (unpublished data). Earl (2004) also showed that Gmed muscle activity was significantly greater in hip abduction with MR exercise than in hip abduction with LR exercise during single-leg stance. Compared with previous studies (unpublished data) that recruited healthy subjects, subjects with weak Gmed muscles showed 16.04%
- 26 -
more activation (healthy vs. weak Gmed: 45.30% vs. 61.34% of MVIC) during SHA-MR. Additionally, the current study found that Gmed muscles (61.34% MVIC) were more active than all the other muscles (Gmax: 23.67%, TFL: 38.51% MVIC) during SHA-MR. The results indicate that this exercise is very effective in targeting Gmed weakness and in preferentially activating the Gmed muscles. The findings may have clinical relevance.
TFL muscle activity was significantly greater in SHA-LR than in SHA-N (8.94%). This finding is in agreement with data reported by McBeth et al. (2012), who reported that TFL activity (70.9 ± 17.2%MVIC) was significantly greater than Gmed muscle activity (53.0 ± 28.4%MVIC) during SHA-LR. The authors of this previous study explained that gravity on the lower extremity would pull the hip joint backward (hip extension); thus, the TFL would be challenged to maintain a neutral position during SHA-LR. The position difference of the hip joint in SHA-MR may also explain the increased Gmed muscle activity in the present study, compared to other exercises. The possible mechanism for these findings may be that the Gmed muscles counteract the anterior roll of the pelvis in the transverse plane during SHA-MR. To overcome the greater external torque, the Gmed would be likely to generate greater force. Another possible mechanism for these findings is the positioning of the Gmed in the highest position in the transverse plane of the upper thigh while sustaining SHA-MR. Thus, SHA-MR may become a preferable position to increase Gmed activation in the frontal plane. Compared with previous studies that recruited healthy subjects, the TFL was more
- 27 -
active in subjects with weak Gmed muscles by 7.87%, 5.91%, and 3.81% during SHA-N, MR, and LR, respectively. People with Gmed weakness might compensate by using the TFL muscles to perform the exercises (Fredericson and Wolf 2005).
The Gmed/TFL muscle activity ratio significantly increased in SHA-MR by 49.76% and 42.99%, compared with SHA-N and SHA-LR, respectively. These Gmed/TFL muscle activity ratio results support the research hypothesis. There is no previous study about the Gmed/TFL activity ratio during SHA; thus, comparison of the results to other work is not possible. However, by following the muscle activity ratio of the Gmed to the TFL during SHA, this study demonstrates that SHA-MR is the best exercise for increasing the Gmed/TFL muscle activity ratio among the three SHA exercises.
Gmax muscle activity and the Gmax/TFL muscle activity ratio were not significantly different among SHA-N, SHA-MR, and SHA-LR. However, the Gmed/Gmax muscle activity ratio was significantly greater in SHA-MR, compared to SHA-N (by 24.94%). Additionally, the Gmax was not activated to levels consistent with Gmed and TFL and no Gmax/TFL ratio was over 1 in this study, suggesting the muscle activity of the Gmax was less than that of the TFL. Previous studies (McBeth et al. 2012; Selkowitz, Beneck, and Powers 2013) also reported that TFL muscles had significantly greater activity that Gmax muscles during SHA. Gmed and TFL muscles are primary hip abductors (Neumann 2010). On the other hand, the Gmax is the primary hip lateral rotator (Neumann 2010)
- 28 -
and the Gmax may be a secondary hip abductor in SHA exercises compared to the Gmed and TFL (Selkowitz, Beneck, and Powers 2013). Thus, SHA is not effective for targeting the Gmax and Gmed synchronistically.
This study has some limitations. First, this study was a cross-sectional study; thus, long-term effects of SHA-MR cannot be determined. Second, crosstalk might have occurred between the Gmed and TFL muscles, although the study took all safety measures to insure the reliability of the EMG signal. Further studies should investigate the long-term effects of SHA-MR on Gmed performance.
- 29 -
Conclusion
This study investigated the effects of different hip rotations on Gmax, Gmed, and TFL muscle activity and on the Gmax/TFL, Gmed/TFL, and Gmed/Gmax muscle activity ratios during SHA exercises in subjects with Gmed weakness. Gmed muscle activity was significantly greater in SHA-MR than in SHA-N. TFL muscle activity was significantly greater in SHA-LR than in SHA-N. The Gmed/TFL activity ratios in SHA-MR were significantly greater than were those in SHA-N and SHA-LR. The Gmed/Gmax activity ratios in MR were significantly greater than those in SHA-N. Thus, SHA-MR is the most effective exercise for greater Gmed muscle activation and for a higher Gmed/TFL muscle activity ratio among the three SHA exercises.
- 30 -
References
Ayotte NW, Stetts DM, Keenan G, and Greenway EH. Electromyographical analysis of selected lower extremity muscles during 5 unilateral weight-bearing exercises. J Orthop Sports Phys Ther. 2007;37:48-55.
Bewyer KJ, Bewyer DC, Messenger D, Kennedy CM. Pilot data: Association between gluteus medius weakness and low back pain during pregnancy. Iowa Orthop J. 2009;29:97-99.
Blandine CG. Anatomy of Movement. Seattle, Eastland Press, 1993.
Bohannon RW. Measurement of muscle performance. Post Grad Adv Phys Ther 1988;2:1–24.
Bohannon RW. Intertester reliability of hand-held dynamometry: A concise summary of published research. Percept Mot Skills. 1999;88:899–902.
Bolgla LA, Uhl TL. Electromyographic analysis of hip rehabilitation exercises in a group of healthy subjects. J Orthop Sports Phys Ther. 2005;35:487-494.
- 31 -
Cichanowski HR, Schmitt JS, Johnson RJ, and Niemuth PE. Hip strength in collegiate female athletes with patellofemoral pain. Med Sci Sports Exerc. 2007;39:1227-1232.
Cram JR, Kasman GS, Holtz J. Introduction to Surface Electromyography. Gaithersburg, Aspen, 1998.
Cynn HS, Oh JS, Kwon OY, Yi CH. Effects of lumbar stabilization using a pressure biofeedback unit on muscle activity and lateral pelvic tilt during hip abduction in sidelying. Arch Phys Med Rehabil. 2006;87:1454-1458.
Delp SL, Hess WE, Hungerford DS, Jones LC. Variation of rotation moment arms with hip flexion. J Biomech. 1999;32:493-501.
De Luca C, The use of surface electromyography in biomechanics. J Appl Biomech. 1997;13:135-163.
Distefano LJ, Blackburn JT, Marshall SW, Padua DA. Gluteal muscle activation during common therapeutic exercises. J Orthop Sports Phys Ther. 2009;39:532-540.
- 32 -
Sport Rehabil. 2004;13:1-11.
Fenter P, Bellew J, Pitts T, Kay R. Reliability of stabilized commercial dynamometers for measuring hip abduction strength: A pilot study. Br J Sports Med. 2003;37:331–334.
Flegal KM, Carroll MD, Kuczmarski RJ, Johnson CL. Overweight and obesity in the United States: Prevalence and trends, 1960-1994. Int J Obes Relat Metab Disord. 1998;22:39-47.
Fredericson M, Wolf C. lliotibial band syndrome in runners: Innovations in treatment. Sports Med. 2005;35:451-459.
Fredericson M, White JJ, Macmahon JM, Andriacchi TP. Quantitative analysis of the relative effectiveness of 3 iliotibial band stretches. Arch Phys Med Rehabil. 2002;83:589-592.
Friel K, McLean N, Myers C, Caceres M. Ipsilateral hip abductor weakness after inversion ankle sprain. J Athl Train. 2006;41:74-78.
Gottschalk F, Kourosh S, Leveau B. The functional anatomy of tensor fasciae latae and gluteus medius and minimus. J Anat. 1989;166:179-189.
- 33 -
Grimaldi A, Richardson C, Durbridge G, Donnelly W, Darnell R, Hides J. The association between degenerative hip joint pathology and size of the gluteus maximus and tensor fascia lata muscles. Man Ther. 2009;14:611-617.
Heinert BL, Kernozek TW, Greany JF, Fater DC. Hip abductor weakness and lower extremity kinematics during running. J Sport Rehabil. 2008;17:243-256.
Hermens HJ, Freriks B, Disselhorst-Klug C, Rau G. Development of recommendations for SEMG sensors and sensor placement procedures. J Electromyogr Kinesiol. 2000;10:361-374.
Hunter AM, St Clair Gibson A, Lambert MI, Nobbs L, Noakes TD. Effects of supramaximal exercise on the electromyographic signal. Br J Sports Med. 2003;37:296-299.
Kendall FP, McCreary EK, Provance PG. Muscles Testing and Function With Posture and Pain.5th ed. Baltimore, Williams & Wilkins, 2005.
Khayambashi K, Mohammadkhani Z, Ghaznavi K, Lyle MA, Powers CM. The effects of isolated hip abductor and external rotator muscle strengthening on pain, health status, and hip strength in females with patellofemoral pain: A randomized controlled trial. J Orthop Sports Phys Ther. 2012;42:22-29.
- 34 -
Kim SJ, Kwon OY, Yi CH, Jeon HS, Oh JS, Cynn HS, Weon JH. Comparison of abdominal muscle activity during a single-legged hold in the hook-lying position on the floor and on a round foam roll. J Athl Train. 2011;46:403-408.
Kimura IF, Jefferson LM, Gulick DT, and Coll RD. Intra- and intertester reliability of Chatillon and Microfet hand-held dynamometers in measuring force production. J Sport Rehabil. 1996;5:197-205.
Kiss RM, Illyés Á. Comparison of gait parameters in patients following total hip arthroplasty with a direct-lateral or antero-lateral surgical approach. Hum Mov Sci. 2012;31:1302-1316.
Kwak SD, Ahmad CS, Gardner TR, Grelsamer RP, Henry JH, Blankevoort L, Ateshian GA, Mow VC. Hamstrings and iliotibial band forces affect knee kinematics and contact pattern. J Orthop Res. 2000;18:101-108.
Lee SP, Souza RB, Powers CM. The influence of hip abductor muscle performance on dynamic postural stability in females with patellofemoral pain. Gait Posture. 2012;36:425-429.
- 35 -
hip extensor and abductor muscle action during level and stair ambulation. An EMG study. Phys Ther. 1983;63:1597-1605.
Marino M, Nicholas JA, Gleim GW. The efficacy of manual assessment of muscle strength using a new device. Am J Sports Med 1982;10:360–364.
McBeth JM, Earl-Boehm JE, Cobb SC, Huddleston WE. Hip muscle activity during 3 side-lying hip-strengthening exercises in distance runners. J Athl Train. 2012;47:15-23.
Merican AM, Amis AA. Iliotibial band tension affects patellofemoral and tibiofemoral kinematics. J Biomech. 2009;42:1539-1546.
Nadler SF, De Prince ML, Hauesien N, Malanga GA, Stitik TP, Price E. Portable dynomometer anchoring station for measuring strength of hip abductors and extensors. Arch Phys Med Rehabil. 2000;81:1072–1076.
Neumann DA. Kinesiology of the hip: A focus on muscular actions. J Orthop Sports Phys Ther. 2010;40:82-94.
Nyland J, Kuzemchek S, Parks M, Caboru D. Femoral anteversion influences vastus medialis and gluteus medius EMG amplitude: Composite hip abductor EMG
- 36 -
amplitude ratios during isometric combined hip abduction-external rotation. J Electromyogr Kinesiol. 2004;14:255-261.
Oh JS, Cynn HS, Won JH, Kwon OY, Yi CH. Effects of performing an abdominal drawing-in maneuver during prone hip extension exercises on hip and back extensor muscle activity and amount of anterior pelvic tilt. J Orthop Sports Phys Ther. 2007;37:320-324.
Park KN, Cynn HS, Kwon OY, Lee WH, Ha SM, Kim SJ, Weon JH. Effects of the abdominal drawing-in maneuver on muscle activity, pelvic motions, and knee flexion during active prone knee flexion in patients with lumbar extension rotation syndrome. Arch Phys Med Rehabil. 2011;92:1477-1483.
Powers CM. The influence of abnormal hip mechanics on knee injury: A biomechanical perspective. J Orthop Sports Phys Ther. 2010;40:42-51.
Rainoldi A, Melchiorri G, Caruso I. A method for positioning electrodes during surface EMG recordings in lower limb muscles. J Neurosci Methods. 2004;134:37-43.
Robinson RL, Nee RJ. Analysis of hip strength in females seeking physical therapy treatment for unilateral patellofemoral pain syndrome. J Orthop Sports Phys Ther.
- 37 -
2007;37:232-238.
Sahrmann S. Diagnosis and Treatment of Movement Impairment Syndromes. St Louis, MO, Mosby, 2003.
Selkowitz DM, Beneck GJ, Powers CM. Which exercises target the gluteal muscles while minimizing activation of the tensor fascia lata? Electromyographic assessment using fine-wire electrodes. J Orthop Sports Phys Ther. 2013;43:54-64.
Soderberg GL, Knutson LM. A guide for use and interpretation of kinesiologic Electromyographic data. Phys Ther. 2000;80:485-498.
Sykes K, Wong YM. Electrical activity of vastus medialis oblique muscle in straight leg raise exercise with different angles of hip rotation. Physiotherapy. 2003;89:423–430.
Wang CY, Olson SL, Protas EJ. Test-retest strength reliability: Hand held dynamometry in community-dwelling elderly fallers. Arch Phys Med Rehabil. 2002;83:811-815.
Wong YM. Skin thickness and VMO:VL ratio. J Orthop Sports Phys Ther. 1999;29:686-686.
- 38 -
국문 요약
중둔근 약화가 있는 대상자의 고관절 외전 시 세 가지
다른 고관절 회전이 고관절 외전근 활성도에
미치는 영향
연세대학교 대학원
물리치료학과
이 지 현
중둔근의 약화는 하지 손상과 밀접한 관련이 있다. 특히 중둔근 약화가 있는 대상자는 일상생활에서 약화된 중둔근을 보상하기 위해 대퇴근막장근 을 이용할 가능성이 있다. 따라서 본 연구의 목적은 중둔근 약화가 있는 대상자에게 옆으로 누운 자세에서 외전 운동 시 고관절 회전을 달리 했을 때 고관절 외전근인 대둔근, 중둔근, 대퇴근막장근에 미치는 영향을 알아- 39 - 보았다. 본 연구를 위해 중둔근 약화가 있는 19명의 대상자가 참여하였고, 각 대상자는 고관절 중립 상태에서 고관절 외전 운동, 고관절 내회전 상태 에서 고관절 외전 운동, 그리고 고관절 외회전 상태에서 고관절 외전 운동 을 실시하였다. 대둔근, 중둔근, 대퇴근막장근의 근활성도는 표면 근전도 장비를 사용하여 측정하였고, 일방향 반복 측정 분산분석을 통해 대둔근, 중둔근, 대퇴근막장근의 세가지 고관절 외전 운동간의 유의성을 알아보았 다. 세 가지 외전 운동에서 유의한 차이가 있을 때 사후검정으로 본페로니 검정을 실시하였다. 통계학적 유의수준은 α = 0.05로 하였다. 연구 결과는 다음과 같다. 1) 중둔근의 근활성도는 고관절 내회전 상태 에서 고관절 외전 운동 시 고관절 중립 상태에서 고관절 외전 운동 시보다 유의하게 높았다. 그리고 대퇴근막장근의 근활성도는 고관절 외회전 상태 에서 고관절 외전 운동 시 고관절 중립 상태에서 고관절 외전 운동 시보다 유의하게 높았다. 2) 중둔근/대퇴근막장근 근활성도비와 중둔근/대둔근 근 활성도 비는 고관절 내회전 상태에서 고관절 외전 운동 시 고관절 중립상 태에서 고관절 외전운동 혹은 고관절 외회전 상태에서 고관절 외전 운동
- 40 - 시보다 유의하게 높았다. 그러므로, 고관절 회전을 달리하면서 고관절 외전 운동 시 중둔근 근활 성도를 증진시키는 운동방법으로는 고관절 내회전 상태에서 고관절 외전 운동을 하도록 추천한다. 핵심 되는 말: 고관절 외전, 고관절 회전, 대둔근, 대퇴근막장근, 중둔근.