Effect of the Abdominal Drawing–in Maneuver and
Self–Stretching the Tensor Fasciae Latae–Iliotibial
Band on Lumbopelvic Kinematics in Subjects With
Lumbar Extension Rotation Syndrome
Onebin Lim
The Graduate School
Yonsei University
Effect of the Abdominal Drawing–in Maneuver and
Self–Stretching the Tensor Fasciae Latae–Iliotibial
Band on Lumbopelvic Kinematics in Subjects With
Lumbar Extension Rotation Syndrome
Onebin Lim
The Graduate School
Yonsei University
Effect of the Abdominal Drawing–in Maneuver and
Self–Stretching the Tensor Fasciae Latae–Iliotibial
Band on Lumbopelvic Kinematics in Subjects With
Lumbar Extension Rotation Syndrome
A Masters Thesis
Submitted to the Department of Physical Therapy
and the Graduate School of Yonsei University
in partial fulfillment of the
requirements for the degree of
Master of Science
This certifies that the masters thesis of
Onebin Lim is approved.
Thesis Supervisor: Chunghwi Yi
Ohyun Kwon: Thesis Committee Member #1
Heonseock Cynn: Thesis Committee Member #2
The Graduate School
Yonsei University
Acknowledgements
Writing my thesis was a greater challenge than I initially expected, and had it not been for the help of many people around me, this thesis would have never been completed. My thesis committee provided me with outstanding mentoring, and the time, energy, and expertise they devoted to ensuring that my research was meaningful is gratefully appreciated. I would like to acknowledge each of them for their contribution to my thesis.
First of all, I would like to express my deepest gratitude to Professor Chunghwi Yi for his great support during this thesis, and the heartfelt encouragement he provided throughout my graduate study. Whenever I had doubts and worries, he was there for me and sincerely wished for my success. I would also like to convey my respect and appreciation to Professor Ohyun Kwon for his enormous help. He taught me how to question my thoughts and express ideas, his insightful advice helped me overcome many crises and finish this thesis. I am also grateful to Professor Heonseock Cynn for his smile, kindness, and intelligent advice. His continual attention and detailed comments on my research helped me focus my ideas. I also sincerely thank Professors Sanghyun Cho, Hyeseon Jeon, and Seunghyun Yoo, who helped
I am indebted to Professor Soyeon Park for her constant encouragement, guidance, and insight. I am truly grateful to Minhee Kim, Dohheon Jung, and Jia Hong for providing continual support, constructive feedback, and encouragement through the joys and sorrows of graduate student life. I thank Silah Choi, Jeongah Kim, Woosuk Lim, and Jaeik Sohn for helping me with laboratory work and providing valuable support.
I would like to thank all of the members in the Graduate School Department of Physical Therapy. They have provided me with tremendous mental support and friendship during my school years.
More than anybody, I wish to express my deepest love and gratitude to my parents who have provided tremendous mental and physical support. Without their strong belief in me and endless encouragement, I could never have finished my graduate study. Thus, I would like to dedicate this thesis to my parents.
Table of Contents
List of Figures ··· iii
List of Tables ··· iv Abstract ··· v Introduction ··· 1 Methods ··· 4 1. Subjects ··· 4 2. Clinical Measurements ··· 7
2.1 Visual Analogue Scale ··· 7
2.2 Tensor Fasciae Latae–Iliotibial Band Length Test ··· 7
3. Experimental Equipment ··· 9
3.1 Three–Dimensional Motion Analysis System ··· 9
4. Outcome Measurements ··· 10 4.1 Kinematic Data ··· 10 5. Procedures ··· 11 6. Interventions ··· 13 7. Statistical Analysis ··· 15 Results ··· 16
1. General Characteristics of Subjects ··· 16
– ii –
4. Tensor Fasciae Latae–Iliotibial Band Length ··· 18
5. Pain Intensity ··· 19
Discussion ··· 22
Conclusion ··· 26
References ··· 27
List of Figures
Figure 1. Hip lateral rotation position ··· 12 Figure 2. Abdominal drawing–in maneuver training using a pressure
biofeedback unit ··· 14 Figure 3. Self–stretching the tensor fasciae latae–iliotibial band ··· 14
Figure 4. Lumbopelvic rotation angle between–group differences ··· 20 Figure 5. Lumbopelvic rotation movement onset between–group
differences ··· 20 Figure 6. Tensor fasciae latae–iliotibial band length between–group
differences ··· 21 Figure 7. Pain intensity between–group differences ··· 21
– iv –
List of Tables
Table 1. Movement system impairment–based lumbar extension rotation classification criteria ··· 6
ABSTRACT
Effect of the Abdominal Drawing–in Maneuver and
Self–Stretching the Tensor Fasciae Latae–Iliotibial
Band on Lumbopelvic Kinematics in Subjects With
Lumbar Extension Rotation Syndrome
Onebin Lim
Dept. of Physical Therapy
The Graduate School Yonsei University
The purpose of this study was to compare the effect of a 2–week period of the abdominal drawing–in maneuver (ADIM) and tensor fasciae latae–iliotibial band
(TFL–ITB) self–stretching on lumbopelvic rotation angle, lumbopelvic rotation movement onset, TFL–ITB length, and pain intensity during active prone hip lateral rotation. Twenty–two subjects with lumbar extension rotation syndrome
– vi –
plus TFL–ITB self–stretching program at home for a 2–week period. A three–
dimensional ultrasonic motion analysis system was used to measure the lumbopelvic
rotation angle and lumbopelvic rotation movement onset. An independent t–test was used to determine between–group differences for each outcome measure
(lumbopelvic rotation angle, lumbopelvic rotation movement onset, TFL–ITB length, and pain intensity). The level of significance was set as α = 0.05. The results showed
that ADIM training plus TFL–ITB self–stretching decreased the lumbopelvic rotation angle, delayed the lumbopelvic rotation movement onset, and elongated the TFL–ITB
significantly more than did ADIM training alone. Pain intensity was lower in the ADIM training plus TFL–ITB self–stretching group than the ADIM training alone
group; however, the difference was not significant. In conclusion, ADIM training plus TFL–ITB self–stretching performed for a 2–week period at home may be an effective treatment for modifying lumbopelvic motion and reducing low back pain.
Key Words: Abdominal drawing–in maneuver, Lumbar extension rotation syndrome,
Introduction
Low back pain (LBP) is a common musculoskeletal problem that affects 70–85% of the population at some point in their lifetime (Hartvigsen et al. 2000; O’Sullivan
2005; Walker, Muller, and Grant 2004). Several investigators have proposed that repeated lumbopelvic motion plays a role in the development and course of LBP
symptoms (Adams et al. 2002; McGill 1997; Sahrmann 2002). LBP symptoms associated with increased lumbopelvic motion, particularly early in the range of trunk
and lower extremity movements during daily activities (Gombatto et al. 2006; Hoffman et al. 2011; Luomajoki et al. 2008; Roussel et al. 2009; Shum GL, Crosbie J,
and Lee RY 2005). Sahrmann (2002) reported that hip lateral rotation (HLR) was impaired in individuals who had LBP symptoms. Specifically, people with LBP
symptoms showed a coupled movement pattern that moved the lumbopelvic region and hip joint simultaneously in the early part of the HLR test (Gombatto et al. 2006).
Manually restricting lumbopelvic motion during the HLR test has been reported to
decrease LBP symptoms (Van Dillen et al. 2009).
Sahrmann (2002) found an increase in lumbopelvic rotation during the active HLR
test in the prone position in people with lumbar extension rotation syndrome. The Movement System Impairment (MSI) classification system for low back pain
categorizes patients with mechanical LBP into five subgroups according to alignment, movements, and symptoms associated with LBP (Sahrmann 2002). The relationship
- 2 -
compensatory lumbopelvic rotation which exerts force on the lumbar region (Ellison
JB, Rose SJ, and Sahrmann SA 1990; Mellin 1990; Vad et al. 2004). This force results
in low magnitude loading, cumulative microtrauma, increased tissue stress in the lumbopelvic region and, eventually, LBP (McGill 1997; Sahrmann 2002).
The abdominal drawing–in maneuver (ADIM), a method of lumbar stabilization training (Akuthota, and Nadler 2004; Hodges, and Richardson 1996), is an effective
neuromuscular intervention for lumbar instability associated with LBP (Akuthota, and Nadler 2004; Macedo et al. 2009; von Garnier et al. 2009). ADIM can be achieved by
the co–contraction of the transversus abdominis (TrA), internal oblique (IO), and multifidus muscles, together with minimal contraction of other superficial abdominal
(external oblique; EO) and paraspinal muscles (Cynn et al. 2006; Hides et al. 2006). Co–contraction of the TrA and multifidus muscles restricts rotation or returns the lumbar spine to the neutral position from a rotated position by tensioning the lateral
attachment of the thoracolumbar fascia (Hodges, and Richardson 1999). Previous studies have shown that ADIM training using a pressure biofeedback unit can prevent
unwanted lumbopelvic motion and enhance training effect of lumbar stability (Cynn et al. 2006; Park et al. 2011; von Garnier et al. 2009).
Limited HLR range is associated with shortened tensor fasciae latae–iliotibial band (TFL–ITB) (Sahrmann 2002). The TFL–ITB acts as a flexor, abductor, and medial
rotator of the hip joint and extensor and lateral rotator of the knee joint (Kendall et al. 2005). The altered TFL–ITB length gives rise to compensatory hip joint motion and
and increases lumbopelvic motion in the transverse plane in patients with LBP
(Sahrmann 2002). Fredericson et al. (2002) reported that the TFL–ITB standing
stretch with arms extended overhead effectively increased TFL–ITB length.
Previous studies have reported using verbal instruction, tactile feedback, and
manual stabilization during HLR to modify excessive lumbopelvic motion and decrease LBP (Hoffman et al. 2011; Scholtes et al. 2010). However, a home exercise
program is necessary to successfully modify lumbopelvic motion and reduce LBP. To our knowledge, no study of the effect of ADIM training and ADIM training plus self–
stretching the TFL–ITB on lumbopelvic motion during active prone HLR has been published previously.
The purpose of the present study was to compare the effect of a 2–week intervention consisting of ADIM training or ADIM training plus self–stretching of the TFL–ITB on lumbopelvic rotation angle, lumbopelvic rotation movement onset,
TFL–ITB length and pain intensity during active prone HLR in people with lumbar extension rotation syndrome accompanying shortened TFL–ITB.
We hypothesized that ADIM training plus self–stretching of the TFL–ITB would decrease the lumbopelvic rotation angle, delay the lumbopelvic rotation movement
onset, increase TFL–ITB length, and decrease pain intensity more than ADIM training alone.
- 4 -
Methods
1. Subjects
Prior to recruiting study subjects, we performed a power analysis to determine the number of subjects required to achieve the effect size of 2.28, the alpha level of 5%, and the power of 80% based on the pilot study performed on subjects with lumbar extension rotation syndrome accompanying shortened TFL– ITB. The results of the power analysis showed that this study would require 10 subjects.
Twenty-two subjects (16 male and 6 female) with lumbar extension rotation syndrome accompanying shortened TFL–ITB participated in this study. Inclusion
criteria included a limited hip adduction range (< 10°) caused by a shortened TFL– ITB (Kendall et al. 2005) and reported LBP for more than 6 months (Von Korff 1994).
Twenty–two subjects were randomly allocated into one of two intervention groups: ADIM training, or ADIM training plus TFL–ITB self–stretching. Subjects were
screened by an examiner who has completed an academic course on the MSI classification system. The examiner selected 22 subjects from 100 subjects based on
the MSI classification criteria for lumbar extension rotation syndrome (Sahrmann 2002; Trudelle–Jackson, Sarvaiya–Shah, and Wang 2008; Van Dillen et al. 1998). Of
the 100 subjects examined, 78 subjects were excluded from the study because they did not meet the selection criteria for lumbar extension rotation syndrome. The
classification criteria for lumbar extension rotation syndrome are shown in Table 1.
These classification criteria consist of alignment and movement tests. Primary tests
are provocation tests that are designed to assess movements or stresses in extension and rotation motion. Secondary tests are confirming tests that are designed to correct
or inhibit the extension and rotation motion. If the primary test is positive, the secondary test is performed. When movement or symptom reduced in the secondary
test, finally it is confirmed as positive. A previous study reported that the percentages of agreement were 98–100% with the kappa values ranging 0.87–1.00 for the
symptom behavior items, and the percentages of agreement were 65–100% with the kappa values ranging 0.00–0.78 for the alignment and movement items (Van Dillen et
al. 1998).
The exclusion criteria were: having (1) rectus femoris muscle shortness determined using Ely’s test, (2) iliopsoas muscle shortness determined using Thomas test, (3)
femoral torsion (antetorsion or retrotorsion) determined using Craig’s test, (4) significant weakness in the hip lateral rotator muscles lower than grade 3 (fair)
determined using the manual muscle testing, and (5) a history of spinal fracture or surgery, disc herniation, spinal deformity, pain or parasthesia below the knee,
systemic inflammatory problem, or other serious musculoskeletal problem that could interfere with HLR in the prone position. The present study was approved by the
Yonsei University Wonju Campus Human Studies Committee, and the subjects were given details of the experiment and provided written informed consent prior to their
- 6 -
Table 1. Movement system impairment–based lumbar extension rotation
classifica-tion criteria
Test
position Primary test Secondary test
Standing
Standing Forward bending Return from bending
Lateral flexion Trunk rotation Single–leg standing
Corrected standing None
Corrected return from bending Corrected lateral flexion
None None
Supine
Hip flexor length Unilateral hip and knee flexion
Hip abduction/lateral rotation
Straight leg raise Shoulder flexion to 180 degrees
None
Corrected unilateral hip and knee flexion
Corrected hip abduction/lateral rotation
Corrected straight leg raise None
Side–lying
Hip lateral rotation Hip abduction with lateral
pelvic tilt Hip adduction None None None Prone Knee flexion Hip rotation Hip extension
Corrected knee flexion Corrected hip rotation Corrected hip extension
Quadruped Quadruped Rocking backward Rocking forward Shoulder flexion Corrected quadruped Corrected rocking backward
None
Corrected shoulder flexion
Sitting
Sitting Knee extension
None
2. Clinical Measurements
2.1 Visual Analogue Scale
Pain intensity was measured using a visual analogue scale (VAS). A 100–mm
VAS was used to assess pain intensity in the low back (Huskisson 1974). The subjects were asked to rate their level of pain on a VAS consisting of a 100–mm line with 0
(no pain) at one end and 100 (the worst pain) at the other end. The VAS has been commonly used in studies evaluating the changes in pain intensity associated with
rehabilitation for LBP (Niemisto et al. 2003)
2.2 Tensor Fasciae Latae–Iliotibial Band Length Test
TFL–ITB length was evaluated by two examiners using the modified Ober’s test
(Kendall et al. 2005). An inclinometer (Johnson Magnetic Angle Locator, Johnson, Mequon, WI, USA) was used to measure TFL–ITB length. The subject was instructed
to lie on their side with the bottom leg flexed at the hip and knee to straighten the lower back. One examiner placed the inclinometer on the distal lateral thigh and held
a subject’s leg at the knee throughout the test with the horizontal position defined as 0° before passive adduction was performed (Herrington, Rivett, and Munro 2006).
The other examiner stabilized the subject’s pelvis to prevent downward lateral pelvic tilt on the tested side. The subject was instructed to raise the top leg keeping it aligned
with the trunk and then allowed it to drop toward the bottom leg (adduction). The test was performed until the subject could feel resistance in the stretched TFL–ITB. At
- 8 -
that point, the examiner recorded the degree of adduction from the horizontal position.
The modified Ober’s test was positive if the subject’s leg remained abducted and did
not fall to the examination table. In other words, if the subject’s leg dropped less than 10° below horizontal, it was recorded as a positive test (Kendall et al. 2005).
Melchione and Sullivan (1993) reported good intra– and inter–rater reliability (ICC 0.94 and 0.73, respectively) using the modified Ober’s test.
3. Experimental Equipment
3.1 Three–Dimensional Motion Analysis System
A three–dimensional ultrasonic motion analysis system (CMS–HS, Zebris, Medizintechnik, Isny, Germany) was used to measure the kinematic parameters of
lumbopelvic and hip joint. The motion analysis system operates with high measure-ment accuracy according to the travelling time measuremeasure-ment of ultrasound pulses. We
used the intraclass correlation coefficient (ICC 3,1) to calculate the intra–rater relia-bility of active HLR and lumbopelvic rotation in the pre–intervention session and
- 10 -
4. Outcome Measurements
4.1 Kinematic Data
The kinematic data obtained from the three–dimensional ultrasonic motion analysis system were used to measure the lumbopelvic rotation angle and lumbopelvic rotation
movement onset during active HLR. Two sets of ultrasound triple markers were used: one was placed on the midline of the pelvis by fastening a strap around the pelvis at
the level of the posterior superior iliac spines to measure lumbopelvic kinematics (lumbopelvic rotation angle and lumbopelvic rotation movement onset) (Cynn et al.
2006; Oh et al. 2007; Park et al. 2011). The second set of triple markers was placed under on the distal 1/3 of the fibula to measure HLR. The measuring sensor, which consisted of three microphones to record the ultrasound signals from the markers, was
positioned lateral to the subject on the side being tested. Angles were calibrated to 0° relative to the prone position with the knee flexed at 90°. The sampling rate was 20 ㎐, and the kinematic data were analyzed using the Win–data ver. 2.19 software
(Zebris, Medizintechnik, Isny, Germany).
The lumbopelvic rotation movement onset was defined as the time at which the angle of the lumbopelvic motion exceeded a threshold of 1° (Gombatto et al. 2006). The mean value of the lumbopelvic rotation angle was calculated from the last 5 s of
isometric contraction during HLR. The mean value of three trials was calculated to determine the lumbopelvic rotation angle and the lumbopelvic rotation movement
5. Procedures
The procedures included clinical measurements involved in subject recruitment and laboratory measurements during the active HLR test. Subjects first completed the
following clinical tests: 1) the VAS, 2) the modified Ober’s test. Following comple-tion of the clinical tests, laboratory measurements were made. Each subject was
in-structed to lie prone position (Figure 1). The starting position was prone with knee flexed at 90° on the side with the shortened TFL–ITB and the other knee extended
(Gombatto et al. 2006). If the TFL–ITB was tight in both legs, the tighter of the two was designated as the test side. Before the HLR test, a thermoplastic splint
(KLARITY Elastic, Klarity Medical & Equipment (GZ) Co. Ltd., Lan Yu, China) was placed on the knee joint to minimize excessive tibial movement caused by the knee joint laxity (Figure 1). Different thermoplastic splints were made for the males
and females to accommodate gender differences in the circumference and width of the knee joint.
The laboratory procedures were as follows: 1) The degree of active HLR was de-termined by asking the subject to laterally rotate the hip as far as possible; 2) A target
bar was positioned at 50% of the maximum active HLR to prevent excessive stretch-ing of the soft tissue of the hip and to provide tactile feedback to stop active HLR
when the medial aspect of the distal tibia touched the target bar. The subject per-formed HLR for 10 s, including a 5–s concentric contraction and a 5–s isometric
con-traction. A 1–min rest period was scheduled between trials. Movement speed and time were controlled using a metronome. The start signal was an auditory cue (beeper
- 12 -
sound) emitted by the Noraxon TeleMyo system (Park et al. 2011). All subjects were
familiarized with the experimental procedure for approximately 30 min prior to the
testing. The subjects were instructed to rest for 10 min after the familiarization period to minimize muscle fatigue.
6. Interventions
The interventions were ADIM training and ADIM training plus self–stretching the TFL–ITB. Subjects in the ADIM training group performed ADIM in the prone
posi-tion and were provided with visual feedback using a pressure biofeedback unit (Stabi-lizer, Chattanooga group Inc., Hixson, TN, USA; Figure 2). The 3–chamber pressure
cell of the pressure biofeedback unit was inflated to 70 mmHg. The subject was asked to reduce the level of pressure by approximately 10 mmHg based on visual feedback
from an analog pressure gauge during prone HLR. To perform the contraction cor-rectly, the subjects were instructed to “Pull your belly button up and in towards your
spine without pelvic movement during exhalation.” It is difficult for patients with LBP to maintain a 60 mmHg level using the pressure biofeedback unit. Thus, the sub-jects were instructed to perform ADIM training 20 min a day, 7 days per week for a
2–week period.
The subjects in the ADIM training plus TFL–ITB self–stretching group were
in-structed to first stretch the TFL–ITB and then ADIM. Subjects were told to perform TFL–ITB self–stretching 2 sets of 10 repetitions a day, 7 days per week, for a 2–week
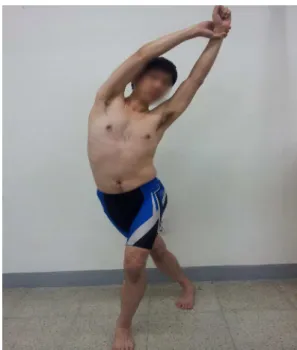
period (Figure 3). The TFL–ITB stretch was performed in the upright standing posi-tion with arms extended and hands clasped overhead. The leg to be stretched was
ex-tended, adducted, and externally rotated and then placed behind the non–tested leg. The subject was then instructed to exhale while slowly bending the trunk laterally in
the direction opposite the test leg (Fredericson et al. 2002). The subjects were in-structed to hold the stretched position for 10 s and rest for 2 min between sets. The
- 14 -
subjects were instructed to stop the exercise if it caused a sharp pain or discomfort in
the lumbopelvic region. Furthermore, the subjects were told that muscle fatigue and a
stretched–out feeling could be expected after each stretching session.
Figure 2. Abdominal drawing–in maneuver training using a pressure biofeedback unit.
Figure 3. Self–stretching the tensor fasciae latae–iliotibial band.
7. Statistical Analysis
Sample size and power calculations were performed using the statistical power analysis program, G*Power ver. 3.1.5 software (Franz Faul, University of Kiel,
Ger-many). Kolmogorov-Smirnov tests were performed to assess whether continuous data approximated a normal distribution. Subjects were randomly allocated to the
experi-mental groups using the Microsoft Excel 2007 software (Microsoft Corporation, Redmond, WA, USA); thus, we expected a homogenous distribution of variance and
did not anticipate significant pre–intervention between–group differences on any out-come measure. However, we conducted an independent t–test to analyze the pre–
intervention values between groups. A paired t–tests was used to determine within– group (before and after an intervention) changes and the independent t–test was used
to determine between–group differences for each outcome measure (lumbopelvic ro-tation angle, lumbopelvic roro-tation movement onset, TFL–ITB length, and pain inten-sity). Cohen’s d statistic was used to calculate the effect size for each outcome
com-parison and was calculated as the difference in the group means divided by the pooled standard deviation (Cohen 1988). All statistical analyses were performed using
PASW Statistics ver. 18.0 software (SPSS, Inc., Chicago, IL, USA). The level of sig-nificance was set as α = 0.05.
- 16 -
Results
1. General Characteristics of Subjects
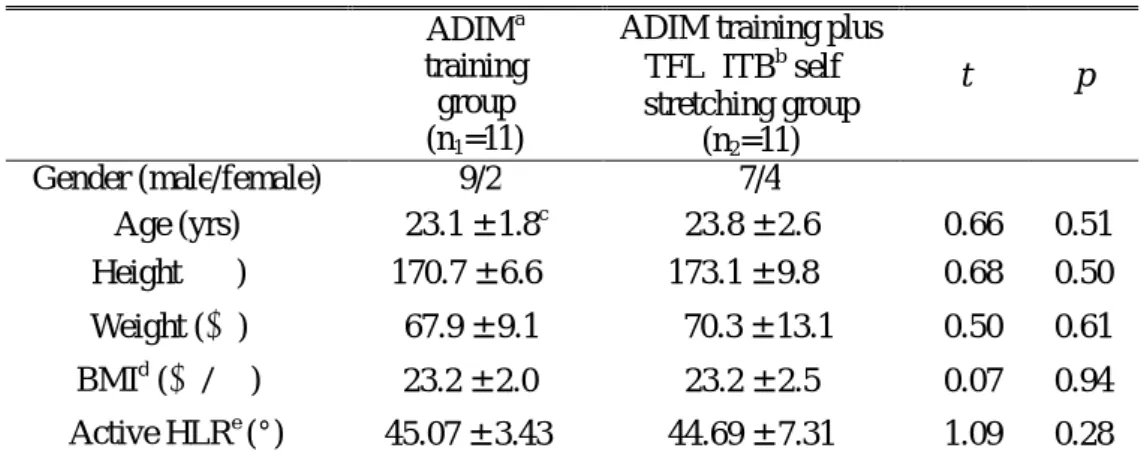
The general characteristics of the 22 subjects including gender, age, height, weight,
body mass index, and active HLR are shown in Table 2.
Table 2. General characteristics of subjects (N=22) ADIMa
training group (n1=11)
ADIM training plus TFL–ITBb self– stretching group (n2=11) t p Gender (male/female) 9/2 7/4 Age (yrs) 23.1 ± 1.8c 23.8 ± 2.6 –0.66 0.51 Height (㎝) 170.7 ± 6.6 173.1 ± 9.8 –0.68 0.50 Weight (㎏) 67.9 ± 9.1 70.3 ± 13.1 –0.50 0.61 BMId (㎏/㎡) 23.2 ± 2.0 23.2 ± 2.5 –0.07 0.94 Active HLRe (°) 45.07 ± 3.43 44.69 ± 7.31 1.09 0.28 a
ADIM: Abdominal drawing–in maneuver.
b
TFL–ITB: Tensor fasciae latae–iliotibial band.
c
Mean ± standard deviation.
d
BMI: Body mass index.
e
HLR: Hip lateral rotation.
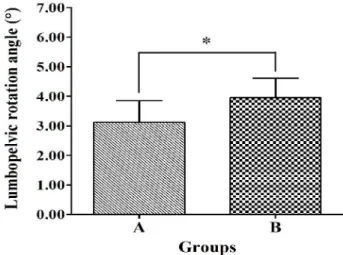
2. Lumbopelvic Rotation Angle
The lumbopelvic rotation angle decreased significantly under the post–intervention
compared with the pre–intervention (ADIM training: pre = 4.94 ± 1.18°, post = 1.82 ± 0.52°, t (10) = –2.76, p = 0.01, d = 4.22; ADIM training plus TFL–ITB self–
stretching: pre = 5.48 ± 0.92°, post = 1.53 ± 0.26°, t (10) = 19.71, p < 0.01, d = 5.95). The ADIM training plus TFL–ITB self–stretching decreased the lumbopelvic rotation
angle significantly more than the ADIM training alone (pre–intervention minus post– intervention, ADIM training: mean difference = 3.12 ± 0.73°; ADIM training plus
TFL–ITB self–stretching: mean difference = 3.95 ± 0.66°, t (20) = –2.76, p = 0.01, d = 1.19, Figure 4).
3. Lumbopelvic Rotation Movement Onset
The lumbopelvic rotation movement onset delayed significantly under the post–
intervention compared with the pre–intervention (ADIM training: pre = 1.53 ± 0.38 s, post = 2.85 ± 0.86 s, t (10) = –5.97, p < 0.01, d = 1.82; ADIM training plus TFL–ITB
self–stretching: pre = 1.58 ± 0.22 s, post = 3.56 ± 0.50 s, t (10) = –9.94, p < 0.01, d = 3.04). The ADIM training plus TFL–ITB self–stretching delayed the lumbopelvic
rotation angle significantly more than the ADIM training alone (ADIM training: mean difference = 1.31 ± 0.72 s; ADIM training plus TFL–ITB self–stretching: mean
- 18 -
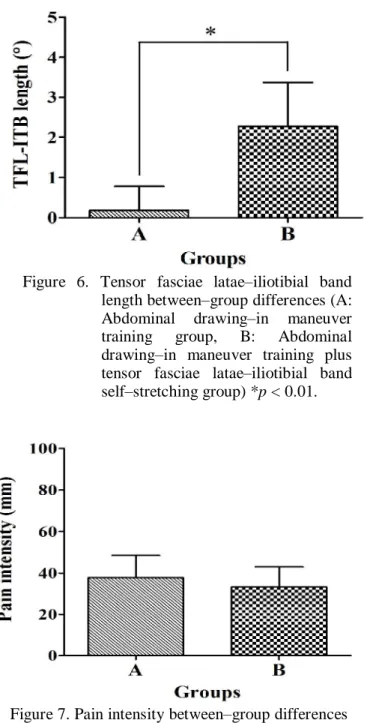
4. Tensor Fasciae Latae–Iliotibial Band Length
The TFL–ITB length was measured using the modified Ober’s test and was ex-pressed as the hip horizontal adduction angle. In the ADIM training, the TFL–ITB
length did not increase significantly under the post–intervention compared with the pre–intervention (ADIM training: pre = 8.09 ± 0.94°, post = 8.27 ± 1.00°, t (10) = –
1.00, p = 0.34, d = 0.29). In the ADIM training plus TFL–ITB self–stretching, the TFL–ITB length increased significantly under the post–intervention compared with
the pre–intervention (ADIM training plus TFL–ITB self–stretching: pre = 8.27 ± 0.90°, post = 10.54 ± 1.43°, t (10) = –6.82, p < 0.01, d = 2.06). The hip horizontal
adduction angle was significantly greater under the ADIM training plus TFL–ITB self–stretching compared with the ADIM training alone (ADIM training: mean
differ-ence = 0.18 ± 0.60°; ADIM training plus TFL–ITB self–stretching: mean differdiffer-ence = 2.27 ± 1.10°, t (20) = –5.51, p < 0.01, d = 2.35, Figure 6).
5. Pain Intensity
The pain intensity decreased significantly under the post–intervention compared
with the pre–intervention (ADIM training: pre = 55.90 ± 8.31 mm, post = 18.18 ± 6.03 mm, t (10) = 11.57, p < 0.01, d = 3.49; ADIM training plus TFL–ITB self–
stretching: pre = 54.54 ± 10.11 mm, post = 21.36 ± 9.51 mm, t (10) = 11.21, p < 0.01, d = 3.37). The pain intensity rating was lower in the ADIM training plus TFL–ITB self–stretching group than in the ADIM training group; however, the difference was not statistically significant (ADIM training: mean difference = 37.72 ± 10.80 mm;
ADIM training plus TFL–ITB self–stretching: mean difference = 33.18 ± 9.81 mm, t (20) = 1.03, p = 0.31, d = 0.44, Figure 7).
- 20 -
Figure 4. Lumbopelvic rotation angle between– group differences (A: Abdominal drawing–in maneuver training group, B: Abdominal drawing–in maneuver training plus tensor fasciae latae– iliotibial band self–stretching group) *p = 0.01.
Figure 5. Lumbopelvic rotation movement onset between–group differences (A: Ab-dominal drawing–in maneuver train-ing group, B: Abdominal drawtrain-ing–in maneuver training plus tensor fasciae latae–iliotibial band self–stretching group) *p = 0.03.
Figure 6. Tensor fasciae latae–iliotibial band length between–group differences (A: Abdominal drawing–in maneuver training group, B: Abdominal drawing–in maneuver training plus tensor fasciae latae–iliotibial band self–stretching group) *p < 0.01.
Figure 7. Pain intensity between–group differences (A: Abdominal drawing–in maneuver training group, B: Abdominal drawing– in maneuver training plus tensor fasciae latae–iliotibial band self–stretching group).
- 22 -
Discussion
The purpose of the present study was to compare the effect of a 2–week intervention with ADIM training or ADIM training plus TFL–ITB self–stretching on
lumbopelvic rotation angle, lumbopelvic rotation movement onset, TFL–ITB length, and pain intensity during active prone HLR in people with lumbar extension rotation
syndrome accompanying shortened TFL–ITB.
The pre–intervention lumbopelvic rotation angle during HLR was 4.94 ± 1.18° in
the ADIM training group and 5.48 ± 0.92° in the ADIM training plus TFL–ITB self– stretching group. These results agree with previous reports of excessive lumbopelvic
motion in people with lumbar extension rotation syndrome (Gombatto et al. 2006;
Harris–Hayes, Van Dillen, and Sahrmann 2005; Hoffman et al. 2011; Scholtes et al. 2010; Van Dillen et al. 2007). Following the intervention in our study, lumbopelvic
rotation was reduced to 1.82 ± 0.52° and 1.53 ± 0.26° in the ADIM training and ADIM training plus TFL–ITB self–stretching groups, respectively. Our results
indicate that the lumbopelvic rotation angle decreased significantly following both interventions. Lumbopelvic rotation angle between–group differences were 3.12 ±
0.73° in ADIM training and 3.95 ± 0.66° in ADIM training plus TFL–ITB self– stretching. Our results indicate that the ADIM training plus TFL–ITB self–stretching
decreased the lumbopelvic rotation angle significantly more than the ADIM training alone, although the difference was minimal. Our results suggest that an improved
the lumbopelvic rotation angle. Our findings are consistent with previous research
showing that insufficient abdominal control and shortened TFL–ITB could contribute
to increased lumbopelvic rotation during active HLR (Sahrmann 2002).
The pre–intervention lumbopelvic rotation movement onset during HLR was 1.53
± 0.38 s in the ADIM training group and 1.58 ± 0.22 s in the ADIM training plus TFL–ITB self–stretching group. This implies that the early lumbopelvic rotation
movement onset could be attributed to the lack of control by the abdominal muscles and the shortened TFL–ITB. This finding concurs with the results of previous studies
reporting that LBP is associated with early lumbopelvic rotation during active limb movement (Sahrmann 2002; Van Dillen et al. 2007; Van Dillen, Maluf, and
Sahrmann 2009; Van Dillen, and Sahrmann 2006). The results of the present study showed that the lumbopelvic rotation movement onset was significantly delayed following both interventions, suggesting that both abdominal control and stretching of
the TFL–ITB contribute to the delayed lumbopelvic rotation movement onset. Moreover, our results showed that ADIM training plus TFL–ITB self–stretching
delayed the lumbopelvic rotation movement onset significantly more than the ADIM training alone, although the difference was minimal. The current study suggests that
treatment may require not only training of the abdominal control, but also stretching of the TFL–ITB to delay the lumbopelvic rotation movement onset during the HLR.
The ADIM training plus TFL–ITB self–stretching group showed a significantly greater increase in the hip horizontal adduction angle than did the ADIM training
- 24 -
TFL–ITB elongated the TFL–ITB. Shortening of the TFL increases ITB tension
resulting in excessive lumbopelvic movement to compensate. Our results are
consistent with those of a previous study showing that stretching in an upright standing position with arms extended overhead is an effective method for increasing
TFL–ITB length (Fredericson et al. 2002).
The level of pain intensity determined using a VAS was significantly reduced
following both interventions. The level of pain intensity was lower in the ADIM training plus TFL–ITB self–stretching group than in the ADIM training group;
however, the difference was not statistically significant. Our results suggest that the reduction in pain may be associated with a reduction compressive stress induced by
restricted lumbopelvic rotation during HLR. Previous studies reported that people with lumbar extension rotation syndrome have a tendency to extend and rotate the lumbar spine during lower–extremity movements. Furthemore, repetitive movement
in a specific direction contributes to cumulative microtrauma of the lumbar tissue and eventually results in LBP (Maluf, Sahrmann, and Van Dillen 2000; Mueller, and
Maluf, 2002).
The present study has several limitations. First, we studied the effect of the ADIM
training and self–stretching the TFL–ITB using a standardized movement test, and it is not clear whether our results can be generalized to other functional activities in
subjects with lumbar extension rotation syndrome. Second, in our measurement of the lumbopelvic rotation motion, the angle was calculated based on movement of the
upper trunk that may have contributed to lumbopelvic rotation. Third, the present
study used surface markers to index bone movement; thus, artifacts resulting from
skin movement were present. Because the lumbopelvic rotation movement was small, skin movement artifacts may have had an impact on our outcome measure. Finally,
the 2–week test period was a short–term intervention. Further research is needed to determine the long–term effect of ADIM training and self–stretching the TFL–ITB on
lumbopelvic kinematics during HLR in subjects with lumbar extension rotation syndrome.
- 26 -
Conclusion
The present study compared the effect of a 2–week intervention with ADIM training or ADIM training plus TFL–ITB self–stretching on lumbopelvic rotation
angle, lumbopelvic rotation movement onset, TFL–ITB length, and pain intensity during active prone HLR in people with lumbar extension rotation syndrome
accompanying shortened TFL–ITB. The results indicate that compared with ADIM training alone, ADIM training plus TFL–ITB self–stretching significantly decreased
the lumbopelvic rotation angle, delayed the lumbopelvic rotation movement onset, and elongated the TFL–ITB. The reported decrease in pain intensity was greater in
the ADIM training plus TFL–ITB self–stretching group than in the ADIM training group; however, the difference was not significant. In conclusion, ADIM training plus
TFL–ITB self–stretching performed for a period of 2 weeks may be an effective treatment for modifying lumbopelvic motion and reducing LBP.
References
Adams MA, Bogduk N, Burton K, and Dolan P. The Biomechanics of Back Pain. 1st ed. Edinburgh: Churchill Livingstone, 2002.
Akuthota V, and Nadler SF. Core strengthening. Arch Phys Med Rehabil. 2004;85(3
suppl 1):S86–S92.
Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd ed. Hillsdale, NJ: Lawrence Erlbaum Associates, 1988.
Cynn HS, Oh JS, Kwon OY, and Yi CH. Effects of lumbar stabilization using a
pres-sure biofeedback unit on muscle activity and lateral pelvic tilt during hip abduction in sidelying. Arch Phys Med Rehabil. 2006;87(11):1454–1458.
Dankaerts W, O’Sullivan PB, Burnett AF, Straker LM, and Danneels LA. Reliability of EMG measurements for trunk muscles during maximal and sub–maximal
volun-tary isometric contractions in healthy controls and CLBP patients. J Electromyogr Kinesiol. 2004;14(3):333–342.
- 28 -
Ellison JB, Rose SJ, and Sahrmann SA. Patterns of hip rotation range of motion: A
comparison between healthy subjects and patients with low back pain. Phys Ther.
1990;70(9):537–541.
Escamilla RF, Babb E, DeWitt R, Jew P, Kelleher P, Burnham T, Busch J, D’Anna K, Mowbray R, and Imamura RT. Electromyographic analysis of traditional and
non-traditional abdominal exercises: Implications for rehabilitation and training. Phys Ther. 2006;86(5):656–671.
Fredericson M, White JJ, Macmahon JM, and Andriacchi TP. Quantitative analysis of
the relative effectiveness of 3 iliotibial band stretches. Arch Phys Med Rehabil. 2002;83(5):589–592.
Gombatto SP, Collins DR, Sahrmann SA, Engsberg JR, and Van Dillen LR. Gender differences in pattern of hip and lumbopelvic rotation in people with low back pain.
Clin Biomech (Bristol, Avon). 2006;21(3):263–271.
Harris–Hayes M, Van Dillen LR, and Sahrmann SA. Classification, treatment and outcomes of a patient with lumbar extension syndrome. Physiother Theory Pract.
Hartvigsen J, Leboeuf–Yde C, Lings S, and Corder EH. Is sitting–while–at–work
as-sociated with low back pain? A systematic, critical literature review. Scand J
Pub-lic Health. 2000;28(3):230–239.
Herrington L, Rivett N, and Munro S. The relationship between patella position and length of the iliotibial band as assessed using Ober’s test. Man Ther.
2006;11(3):182–186.
Hides J, Wilson S, Stanton W, McMahon S, Keto H, McMahon K, Bryant M, and Richardson C. An MRI investigation into the function of the transversus abdominis
muscle during “drawing–in” of the abdominal wall. Spine (Phila Pa 1976). 2006;31(6):E175–E178.
Hodges PW, and Richardson CA. Inefficient muscular stabilization of the lumbar spine associated with low back pain: A motor control evaluation of transverses
abdominis. Spine (Phila Pa 1976). 1996;21(22):2640–2650.
Hodges PW, and Richardson CA. Transversus abdominis and the superficial ab-dominal muscles are controlled independently in a postural task. Neurosci let.
- 30 -
Hoffman SL, Johnson MB, Zou D, Harris–Hayes M, and Van Dillen LR. Effect of
classification–specific treatment on lumbopelvic motion during hip rotation in
people with low back pain. Man Ther. 2011;16(4):344–350.
Huskisson EL. Measurement of pain. Lancet. 1974;9:1127–1131.
Kendall FP, McCreary EK, Provance PG, Rodgers MM, and Romani WA. Muscles: Testing and Function With Posture and Pain. 5th ed. Baltimore: Lippincott Wil-liams & Wilkins, 2005.
Luomajoki H, Kool J, de Bruin ED, and Airaksinen O. Movement control tests of the low back: Evaluation of the difference between patients with low back pain and healthy controls. BMC Musculoskelet Disord. 2008;9:170.
Macedo LG, Maher CG, Latimer J, and McAuley JH. Motor control exercise for
per-sistent, nonspecific low back pain: A systematic review. Phys Ther. 2009;89(1):9– 25.
Maluf KS, Sahrmann SA, and Van Dillen LR. Use of a classification system to guide
nonsurgical management of a patient with chronic low back pain. Phys Ther.
2000;80(11):1097–1111.
Marshall P, and Murphy B. The validity and reliability of surface EMG to assess the neuromuscular response of the abdominal muscles to rapid limb movement. J
Electromyogr Kinesiol. 2003;13(5):477–489.
McClure PW, Esola M, Schreier R, and Siegler S. Kinematic analysis of lumbar and hip motion while rising from a forward, flexed position in patients with and
with-out a history of low back pain. Spine (Phila Pa 1976). 1997;22(5):552–558.
McGill SM. The biomechanics of low back injury: Implications on current practice in
industry and the clinic. J Biomech. 1997;30(5):465–475.
Melchione WE, and Sullivan MS. Reliability of measurements obtained by use of an instrument designed to indirectly measure iliotibial band length. J Orthop Sports
Phys Ther. 1993;18(3):511–515.
Mueller MJ, and Maluf KS. Tissue adaptation to physical stress: A proposed “physi-cal stress theory” to guide physi“physi-cal therapist practice, education, and research. Phys
- 32 -
Niemistö L, Lahtinen–Suopanki T, Rissanen P, Lindgren KA, Sarna S, and Hurri H.
A randomized trial of combined manipulation, stabilizing exercises, and physician
consultation compared to physician consultation alone for chronic low back pain. Spine (Phila Pa 1976). 2003;28(19):2185–2191.
Oh JS, Cynn HS, Won JH, Kwon OY, and Yi CH. Effects of performing an
ab-dominal drawing–in maneuver during prone hip extension exercises on hip and back extensor muscle activity and amount of anterior pelvic tilt. J Orthop Sports
Phys Ther. 2007;37(6):320–324.
O’Sullivan P. Diagnosis and classification of chronic low back pain disorders: Mala-daptive movement and motor control impairments as underlying mechanism. Man Ther. 2005;10(4):242–255.
O’Sullivan PB, Twomey L, and Allison GT. Altered abdominal muscle recruitment in
patients with chronic back pain following a specific exercise intervention. J Orthop Sports Phys Ther. 1998;27(2):114–124.
Park KN, Cynn HS, Kwon OY, Lee WH, Ha SM, Kim SJ, and Weon JH. Effects of
the abdominal drawing–in maneuver on muscle activity, pelvic motions, and knee flexion during active prone knee flexion in patients with lumbar extension rotation
Roussel NA, Nijs J, Mottram S, Van Moorsel A, Truijen S, and Stassijns G. Altered
lumbopelvic movement control but not generalized joint hypermobility is
associat-ed with increasassociat-ed injury in dancers. A prospective study. Man Ther. 2009;14(6):630–635.
Sahrmann SA. Diagnosis and Treatment of Movement Impairment Syndrome. St.
Louis, MO: Mosby Inc, 2002.
Scholtes SA, Norton BJ, Lang CE, and Van Dillen LR. The effect of within–session instruction on lumbopelvic motion during a lower limb movement in people with
and people without low back pain. Man Ther. 2010;15(5):496–501.
Shum GL, Crosbie J, and Lee RY. Symptomatic and asymptomatic movement
coor-dination of the lumbar spine and hip during an everyday activity. Spine (Phila Pa 1976). 2005;30(23):E697–E702.
Trudelle–Jackson E, Sarvaiya–Shah SA, and Wang SS. Interrater reliability of a
movement impairment–based classification system for lumbar spine syndromes in patients with chronic low back pain. J Orthop Sports Phys Ther. 2008;38(6):371–
- 34 -
Van Dillen LR, Gombatto SP, Collins DR, Engsberg JR, and Sahrmann SA.
Sym-metry of timing of hip and lumbopelvic rotation motion in 2 different subgroups of
people with low back pain. Arch Phys Med Rehabil. 2007;88(3):351–360.
Van Dillen LR, Maluf KS, and Sahrmann SA. Further examination of modifying pa-tient–preferred movement and alignment strategies in patients with low back pain
during symptomatic tests. Man Ther. 2009;14(1):52–60.
Van Dillen LR, Sahrmann SA, Norton BJ, Caldwell CA, Fleming DA, McDonnell MK, and Woolsey NB. Reliability of physical examination items used for
classifi-cation of patients with low back pain. Phys Ther. 1998;78(9):979–988.
Van Dillen LR, and Sahrmann SA. Outcomes of classification–directed intervention
in people with chronic or recurrent low back pain. J Orthop Sports Phys Ther. 2006;36:A61–62.
Vad VB, Bhat AL, Basrai D, Gebeh A, Aspergren DD, and Andrews JR. Low back
pain in professional golfers: The role of associated hip and low back range–of– motion deficits. Am J Sports Med. 2004;32(2)494–497.
von Garnier K, Köveker K, Rackwitz B, Kober U, Wilke S, Ewert T, and Stucki G.
Reliablility of a test measuring transversus abdominis muscle recruitment with a
pressure biofeedback unit. Physiotherapy. 2009;95(1):8–14.
Von Korff M. Studying the natural history of back pain. Spine (Phila Pa 1976). 1994;19(18 Suppl):2041S–2046S.
Walker BF, Muller R, and Grant WD. Low back pain in Australian adults Health
pro-vider utilization and care seeking. J Manipulative Physiol Ther. 2004;27(5):327– 335.
- 36 -
국문 요약
요추 신전 회전 증후군을 가진 대상자에게 복부
당기기 방법과 대퇴 근막 긴장근-장경인대 자가신장
운동이 요추골반 운동형상학에 미치는 영향
연세대학교 대학원
물리치료학과
임 원 빈
본 연구의 목적은 대퇴 근막 긴장근-장경인대가 짧은 요추 신전 회전 증후군 대상자에게 엎드린 자세에서 능동 고관절 외회전 시 복부 당기기 방법과 대퇴 근막 긴장근-장경인대 자가신장 운동이 요추골반 회전 각도, 요추골반 회전 움직임 개시시간, 대퇴 근막 긴장근-장경인대 길이, 통증 강도에 미치는 영향을 비교하는 것이다. 본 연구를 위해 대퇴 근막 긴장근-장경인대가 짧은 요추 신전 회전 증후군이 있는 22명의 대상자(남자 16명과 여자 6명)가 참여하였다. 대상자들은 2주간 집에서수행될 복부 당기기 방법과 대퇴 근막 긴장근-장경인대 자가신장 운동 수행 방법을 교육받았다. 3차원 초음파 동작 분석기는 요추골반 회전 각도, 요추골반 회전 움직임 개시시간을 측정하는데 사용하였다. 독립 t-검정은 결과분석(요추골반 회전 각도, 요추골반 회전 움직임 개시시간, 대퇴 근막 긴장근-장경인대 길이, 통증 강도)에 대한 집단 간 차이를 알아보기 위해 사용하였다. 통계학적 유의수준 α = 0.05로 하였다. 연구 결과 복부 당기기 방법만 적용하였을 때보다 복부 당기기 방법과 대퇴 근막 긴장근-장경인대 자가신장 운동을 함께 적용하였을 때, 요추골반 회전 각도는 유의하게 감소하였고, 요추골반 회전 움직임 개시시간은 유의하게 지연되었으며, 대퇴 근막 긴장근-장경인대 길이는 유의하게 신장되었고, 통증 강도는 감소하였지만 유의미한 차이는 보이지 않았다. 결론적으로, 2주간 복부 당기기 방법과 대퇴 근막 긴장근-장경인대 자가신장 운동을 함께 적용한 중재방법이 요추골반 움직임을 교정하고 요통을 감소시키는데 효과적인 중재방법으로 사료된다. 핵심 되는 말: 대퇴 근막 긴장근-장경인대, 복부 당기기 방법, 요추 신전 회전 증후군, 요추골반 운동형상학.