저작자표시-동일조건변경허락 2.0 대한민국 이용자는 아래의 조건을 따르는 경우에 한하여 자유롭게 l 이 저작물을 복제, 배포, 전송, 전시, 공연 및 방송할 수 있습니다. l 이차적 저작물을 작성할 수 있습니다. l 이 저작물을 영리 목적으로 이용할 수 있습니다. 다음과 같은 조건을 따라야 합니다: l 귀하는, 이 저작물의 재이용이나 배포의 경우, 이 저작물에 적용된 이용허락조건 을 명확하게 나타내어야 합니다. l 저작권자로부터 별도의 허가를 받으면 이러한 조건들은 적용되지 않습니다. 저작권법에 따른 이용자의 권리는 위의 내용에 의하여 영향을 받지 않습니다. 이것은 이용허락규약(Legal Code)을 이해하기 쉽게 요약한 것입니다. Disclaimer 저작자표시. 귀하는 원저작자를 표시하여야 합니다. 동일조건변경허락. 귀하가 이 저작물을 개작, 변형 또는 가공했을 경우 에는, 이 저작물과 동일한 이용허락조건하에서만 배포할 수 있습니다.
Genetic Association Study of Osteoporotic
Vertebral Compression Fractures in
Postmenopausal Women
by
Young Sun Chung
Major in Medicine
Department of Medical Sciences
The Graduate School, Ajou University
Genetic Association Study of Osteoporotic
Vertebral Compression Fractures in
Postmenopausal Women
by
Young Sun Chung
A Dissertation Submitted to The Graduate School of Ajou University
in Partial Fulfillment of the Requirements for the Degree of
Ph. D. in Medicine
Supervised by
Ki Hong Cho, M.D., Ph.D.
Major in Medicine
Department of Medical Sciences
The Graduate School, Ajou University
This certifies that the dissertation
of Young Sun Chung is approved.
SUPERVISORY COMMITTEE
Young Hwan Ahn
Kyung Gi Cho
Ki Hong Cho
Se Hyuk Kim
Nam Keun Kim
The Graduate School, Ajou University
June, 23rd, 2011
ABSTRACT
-Genet
i
cAssoci
at
i
on St
udy ofOst
eopor
ot
i
cVer
t
ebr
al
Compr
essi
on Fr
act
ur
esi
n Post
menopausalWomen
Vascularendothelialgrowth factor(VEGF)is involved in bone formation throughitsrolein angiogenesis.VEGF isalsoknown topromotethehealing offracturesand hyperhomocysteinemiaisassociated with therisk ofskeletal healthproblems,suchasosteoporosis,low body mineraldensity,andfracture. 5,10-Methylenetetrahydrofolatereductase(MTHFR)andthymidylatesynthase (TS)areinvolvedin homocysteinemetabolism.Thus,wedeterminedwhether or not VEGF, MTHFR, and TS polymorphisms are associated with osteoporotic vertebral compression fractures in postmenopausal Korean women. The study subjects consisted of 82 patients with osteoporotic vertebral compression fractures and 117 control postmenopausal Korean women.PCR-RFLP and real-time PCR assay were used to analyze VEGF, MTHFR,andTS polymorphisms.Homocysteinelevelswerealsomeasuredto determine whether or not polymorphisms of the VEGF gene affect homocysteine/folate metabolism. The AA genotype of the -2578C>A polymorphism were significantly different between the stroke and control groups;no significantdifferences in the -1154G>A,-634G>C,and 936C>T genotype frequencies existed. However, the A-G-G-C haplotype had a tendency tobeassociatedwithosteoporoticvertebralcompressionfracturesin postmenopausalKorean women.Associations between the VEGF -2578C>A polymorphism and homocysteine levels were also noted. There was not
significantassociation ofMTHFR and TS polymorphisms with osteoporotic vertebralcompression fractures.In summary,these results suggestthatthe VEGF -2578C>A polymorphisms and VEGF haplotypes may play an importantrolein theetiology ofosteoporotic vertebralcompression fractures inpostmenopausalKoreanwomen.
_____________________________________________________________
Key words:vascularendothelialgrowthfactor(VEGF),osteoporoticvertebral compression fracture (OVCF), postmenopausal women, polymorphism, homocysteine
TABLE OF CONTENTS
ABSTRACT ··· i
TABLE OF CONTENTS ···iii LIST OF FIGURES ···ⅳ LIST OF TABLES ···ⅴ Ⅰ.INTRODUCTION ···1
Ⅱ.MATERIALS AND METHODS ···4
A.Patients ···4
B.Measurementofhomocysteinelevels ···5
C.GenotypingoftheVEGF polymorphisms ···5
D.GenotypingoftheMTHFR andTS polymorphisms ···6
E.Stasticalanalysis ···10 Ⅲ.RESULTS ···11 Ⅳ.DISCUSSION ···24 Ⅴ.CONCLUSION ···27 REFERENCES ···28 국문요약 ··· 36
LI
ST OF FI
GURES
Figure1.PCR-RFLP analysisofVEGF -2578C>A (A)and
-1154G>A (B)polymorphisms···13
Figure2.PCR-RFLP analysisofVEGF -634G>C (A)and
936C>T (B)polymorphisms···14
Figure3.PCR-RFLP analysisofMTHFR 677C>T (A)and
1298A>C (B)polymorphisms···15
Figure4.PCR-RFLP analysisofTSER (A)and
LI
ST OF TABLES
Table1.Primersandrestrictionenzymesforeachpolymorphism
analysis···9 Table2.Baselinecharacteristicinvertebralcompressionfracture
patientsandcontrolsubjects···17 Table3.Oddsratios(OR)and95% confidenceintervals(CI)of
theVEGF-2578C>A,-1154G>A,-634G>C and936C>T polymorphismsinpatientswithosteoporoticvertebral
compressionfractureinpostmenopausalwomen···18 Table4.FrequenciesoftheVEGF -2578C>A,-1154G>A,
-634G>C and936C>T haplotypesinpatientswith osteoporoticvertebralcompressionfracturein
postmenopausalwomen···19 Table5.ComparisonofhomocysteinelevelsaccordingtoVEGF
-2578C>A polymorphism inthecaseandcontrols···20 Table6.Relativerisksofthepatientswithosteoporoticvertebral
compressionfracturebyquartileofplasma
homocysteinelevel···21
Table7.Oddsratios(OR)and95% confidenceintervals(CI) oftheMTHFR andTS polymorphismsinpatientswith osteoporoticvertebralcompressionfracturein
Table8.CombinationgenotypefrequenciesofMTHFR andTS polymorphismsinpatientswithosteoporoticvertebral
Ⅰ.I
NTRODUCTI
ON
Osteoporosis is a common metabolic bone disordercharacterized by reduced bone mass,increased skeletalfragility and microarchitecturaldeterioration,and asaconsequence,increased bonefractures.Osteoporoticfracturesarealeading causeofdisability and indirectly,death in theelderly (Centeretal.,1999;NIH ConsensusDevelopmentPanel,2001).Approximately 30% ofwomen and12% of men are affected by osteoporosis atsome point;thus,osteoporosis imposes a major economic burden on society (Costa etal.,2009).Menopause results in accelerated bonelossas a consequenceofestrogen deficiency superimposed on age-related,linearboneloss(Pouillèsetal.,1994).
Osteoporosis is a disease caused by several factors, including metabolic abnormalities ofhomocysteine (Hcy)/folate.Thymidylate synthase (TS)is one enzyme involved in Hcy/folate metabolism (Liu etal.,2002),as itis a critical enzyme in thymidylate and DNA synthesis.5,10-methylenetetrahydrofolate is required forthisprocess(McLean etal.,2004).TS polymorphismsinfluencethe conversion of Hcy to methionine because TS competes with 5, 10-methylenetetrahydrofolatereductase(MTHFR)for5,10-methylenetetrahydrofolate as a substrate (Trinh etal.,2002;Kim etal.,2006).However,osteoporosis is more strongly influenced by genetic factors than by environmentalinfluences. Twinandpedigreestudieshavedemonstratedthatgeneticinfluencesaccountfor 50-80% of the interindividualvariability of bone mineraldensity (BMD) in youngadults(Dequeckeretal.,1987;Pococketal.,1987;Slemendaetal.,1991). Vascularendothelialgrowth factor(VEGF)performsan importantfunction in angiogenesis, and is an important regulator of endothelial cell proliferation (Senger et al.,1993; Iruela-Arispe and Dvorak,1997).There is convincing
evidence that VEGF plays a major role in enhancing bone formation and fracture healing through its role in angiogenesis (Akeno etal.,2001;Streetet al.,2002;Uchida etal.,2003;Komatsu and Hadjiargyrou,2004;Geigeretal., 2005,2007;Daiand Rabie,2007).In addition,VEGF is also involved in the developmentofdiseases with a putativeangiogenicbasis,including cancerand cerebrovascular or cardiovascular diseases (Ladouxand Frelin, 1993). Under physiologicandpathologicconditions,VEGF overexpression hasbeen notedina varietyoftissues(LadouxandFrelin,1993).
Severalhormones that influence skeletalhomeostasis have been shown to regulatetheproduction ofVEGF locally (Esbritetal.,2000;Hyderetal.,2000), although theeffectoftheseendocrineregulatorson circulating levelsofVEGF remains unknown. Estrogen has been shown to regulate VEGF gene transcription(Hyderetal.,2000).Previousstudieshavedemonstratedaprofound geneticeffectonthevariationincirculatinglevelsofVEGF (Renneretal.,2000; Pantsulaiaetal.,2004).Severalpolymorphismsin thepromoteranduntranslated regions (UTRs)ofthe VEGF gene have been reported.These polymorphisms are associated with a variety of diseases, including recurrent spontaneous abortion, pre-eclampsia, colon cancer, stomach cancer, and breast cancer (Papazoglouetal.,2005;Jacobsetal.,2005;Jinetal.,2005;Chapuisetal.2006; Park et al., 2007; Bae et al., 2008; Lee et al., 2010). In particular, the VEGF-2578A,-1154A,-634G,and 936T alleles are associated with reduced VEGF expression (Shahbazietal.,2002;Lambrechts etal.,2003).The -1154A allele,whichislinkedwithlowerVEGF levelshasbeenshowntobeassociated with an increased risk ofrecurrentspontaneous abortions (Lee etal.,2010). RecentdataindicatethatHcy and folateaffectsbonemetabolism,bonequality, andfractureriskinhumans.Becausecirculating Hcy dependsonfolate,vitamin B6,and vitamin B12,Hcy may prove to be an appropriate risk indicator for
micronutrient deficiency-related osteoporotic fractures (Herrmannetal., 2005; Cagnaccietal.,2008).
Even though VEGF and Hcy have been shown to play roles in bone metabolism, there have been a few polymorphism studies conducted with patientssuffering from osteoporoticcompression fractures.Therefore,theauthor investigated the VEGF,MTHFR,and TS polymorphisms and Hcy levels in postmenopausalKoreanwomenwithosteoporoticvertebralcompressionfractures.
Ⅱ.MATERI
ALS AND METHODS
A.Patients
One hundred ninety-nine Korean women who were atleast12 months past theirlastmenstrualperiodwererecruitedatrandom from theNeurosurgicaland Orthopedic Departments at Bundang CHA Medical Center in South Korea betweenNovember2002andDecember2004.
Eighty-two subjects (70.10 ± 1.04 years [mean ± SEM]) suffering from osteoporotic vertebralcompression fractures were selected forinclusion in the patientgroup.Bone mineraldensitometry (BMD)atthe lumbarspine (L2-L4) was measured using dual-energy X-ray absorptiometry (Hologic Discovery W, Waltham,MA,USA).An osteoporoticfracturewasdefinedby at-score< -2.5 (n=46) and/or at least one non-traumatic fracture of the spine (n=36).The control group consisted of 117 postmenopausal women (66.18 ± 0.79 years [mean±SD])withoutvertebralfracturesora previousdiagnosisofosteoporosis. A fracturewasdefinedasareductionof20% ormoreintheanterior,posterior, orcentralheightofthevertebra.Allexaminationswereconducted according to the methods described previously by a trained neurosurgeon and orthopedic surgeon (Villadsen etal.,2005).This study was approved by the Institutional Review Board(IRB)ofCHA University in SouthKorea.Allofthepatientsand controls were Koreans, and they all provided informed consent prior to enrollmentinthestudy.
B.Measurementofhomocysteinelevels
Venousblood samplesfrom individualswho had been fasting for8-12hours were obtained in tubes containing potassium ethylenediaminetetraacetic acid (EDTA).Fasting Hcy levels were measured in patients and controls (IMx; AbbottLaboratories,Chicago,IL,USA).Plasma Hcy levels were measured as totalHcybyfluorescencepolarizationimmunoassay(FPIA).
C.Genotyping oftheVEGF polymorphisms
Genomic DNA was extracted from whole blood and purified via high-salt buffermethods.Itwasthendilutedto100ng/μL with1X TE buffer.A volume of 1 μL from each sample was used in the amplification of VEGF polymorphisms.VEGF -2578C>A,-1154G>A,-634G>C,and 936C>T genotypes were analyzed via the polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP)method.
PCR oftheVEGF -2578C>A polymorphism wascarriedoutusing primersto generate a 308 bp (C allele)- or 326 (A allele)-bp product:forward 5’-GGA TGG GGC TGA CTA GGT AAG-3’andreverse5’-AGC CCC CTT TTC CTC CAA C-3’.FortheVEGF -1154G>A polymorphism,thefollowing primerswere employed togeneratea173-bp product:forward 5’-CGC GTG TCT CTG GAC AGA GTT TCC-3’andreverse5’-CGG GGA CAG GCG AGC TTC AG-3.For the VEGF -634G>C polymorphism,the following primers were employed to generate a 204-bp product:forward 5’-CAG GTC ACT CAC TTT GCC CCG GTC-3’andreverse5’-GCT TGC CAT TCC CCA CTT GAA TCG-3’.Forthe VEGF 936C>T polymorphism,thefollowingprimerswereempolyedtoamplifya
208-bp fragment:forward 5’-AAG GAA GAG GAG ACT CTG CGC AGA GC-3’and reverse5’-TAA ATG TAT GTA TGT GGG TGG GTG TGT CTA CAG G-3’.
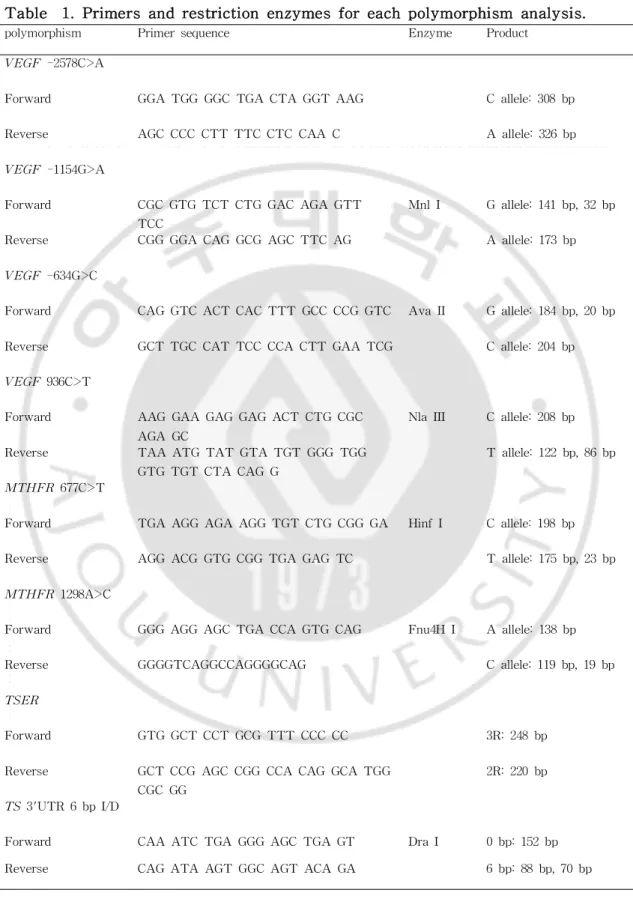
TheVEGF -2578C>A istightlylinkedwiththedeletion/insertionofthe18bp fragment at -2549 region.The -2578C>A was genotyped according to an amplified fragmentsize;-2578C (18 bp deletion)corresponded to 308 bp and -2578A (18 bp insertion) corresponded to 326 bp. The VEGF -1154G>A polymorphism was analyzed via digestion of the PCR product with the restriction endonuclease MnlⅠ (New England Biolabs) at37°C for 16 hours. The-1154G allelecontaining the173bpfragmentwasdigestedinto141and32 bp fragments while the -1154A allele was notdigested.The VEGF -634G>C polymorphisms were identified by digesting the PCR productwith restriction endonucleaseAvaⅡ (New England Biolabs,Beverly,MA,USA)at37°C for16 hours.The-634G allelecontaining the204 bp fragmentwasdigested into 180 and 24 bp fragments,whereas the -634C allele was notdigested.The VEGF 936C>T polymorphism wasanalyzed viadigestion ofthePCR productwith the restriction endonuclease NlaⅢ (New England Biolabs) at37°C for 16 hours. The936T allelecontainingthe208bpfragmentwasdigestedinto122and86bp fragments, whereas the 936C allele was not digested. The primers and restriction enzymesfortheVEGF polymorphism analysesareprovidedin Table 1.
D.Genotyping oftheMTHFR andTS polymorphisms
MTHFR and TS polymorphism analyses were conducted using PCR and PCR-RFLP methods.The primers and PCR conditions for each polymorphism
analysis were described previously (Kim et al.,2006;Yim et al.,2010).All reactions were conducted using a HotStartPCR premix kit(Bioneer,Daejeon, Korea)ina20μL volumeincluding 0.5μM ofeachprimer.Amplifiedfragments wereconfirmedon3% agarosegelviaelectrophoresis.
MTHFR 677C>T polymorphism was distinguished via PCR using forward primer5'-TGA AGG AGA AGG TGT CTG CGG GA-3'and reverse primer 5'-AGG ACG GTG CGG TGA GAG TC-3'.Amplifiedfragmentsweredigested by HinfⅠ (New England BioLabs).The 677T allele containing the 198 bp fragmentwasdigestedinto175and23bpfragmentswhilethe677C allelewas notdigested.
MTHFR 1298A>C polymorphism was distinguished via PCR using the forward primer5'-GGG AGG AGC TGA CCA GTG CAG-3'and the reverse primer 5'-GGG GTC AGG CCA GGG GCA G-3'.Amplified fragments were digestedwithFnu4HⅠ (New England BioLabs).The1298C allelecontaining the 138bpfragmentwasdigestedinto119and19bpfragments,whereasthe1298A allelewasnotdigested.
Thymidylate synthase enhancer region (TSER)28 bp tandem repeats were distinguishedviaPCR usingforwardprimer5'-GTG GCT CCT GCG TTT CCC CC-3'andreverseprimer5'-GCT CCG AGC CGG CCA CAG GCA TGG CGC GG-3'.TheTSER 2R and 3R polymorphismsweregenotyped according to an amplified fragmentsize;2R correspondedto220bpand3R correspondedto248 bp.
TS 3'-UTR 1494 6 bp insertion/deletion polymorphism was PCR amplified using forward primer5'-CAA ATC TGA GGG AGC TGA GT-3'and reverse primer5'-CAG ATA AGT GGC AGT ACA GA-3'.Amplified fragmentswere digested with DraⅠ (New England BioLabs).The 6 bp containing 158 bp fragmentwas digested into 70 and 88 bp fragments and the 152 bp fragment
without the 6 bp insertion was not digested. The primers and restriction enzymesfortheMTHFR andTSpolymorphism analysesareshowninTable1.
Table 1.Primersandrestriction enzymesforeach polymorphism analysis.
polymorphism Primersequence Enzyme Product
VEGF -2578C>A
Forward GGA TGG GGC TGA CTA GGT AAG C allele:308bp Reverse AGC CCC CTT TTC CTC CAA C A allele:326bp
VEGF -1154G>A
Forward CGC GTG TCT CTG GAC AGA GTT TCC
MnlI G allele:141bp,32bp Reverse CGG GGA CAG GCG AGC TTC AG A allele:173bp
VEGF -634G>C
Forward CAG GTC ACT CAC TTT GCC CCG GTC AvaII G allele:184bp,20bp Reverse GCT TGC CAT TCC CCA CTT GAA TCG C allele:204bp
VEGF 936C>T
Forward AAG GAA GAG GAG ACT CTG CGC AGA GC
NlaIII C allele:208bp Reverse TAA ATG TAT GTA TGT GGG TGG
GTG TGT CTA CAG G
T allele:122bp,86bp
MTHFR 677C>T
Forward TGA AGG AGA AGG TGT CTG CGG GA HinfI C allele:198bp Reverse AGG ACG GTG CGG TGA GAG TC T allele:175bp,23bp
MTHFR 1298A>C
Forward GGG AGG AGC TGA CCA GTG CAG Fnu4H I A allele:138bp Reverse GGGGTCAGGCCAGGGGCAG C allele:119bp,19bp
TSER
Forward GTG GCT CCT GCG TTT CCC CC 3R:248bp Reverse GCT CCG AGC CGG CCA CAG GCA TGG
CGC GG
2R:220bp
TS 3'UTR 6bpI/D
Forward CAA ATC TGA GGG AGC TGA GT DraI 0bp:152bp Reverse CAG ATA AGT GGC AGT ACA GA 6bp:88bp,70bp
E.Statisticalanalysis
The 2-test was used to evaluate the Hardy-Weinberg equilibrium.Odds ratios (ORs) and 95% confidence intervals (CI) were estimated in order to assessthestrength oftheassociation between genotypefrequenciesand cases. Statisticalsignificance was accepted atthe p < 0.05 level.Statisticalanalyses werecarried outwith GraphPad Prism4.0 (GraphPad Software,Inc.,San Diego, CA,USA) and SNPAlyzeTM (version 5.10;DYNACOM Co.,Ltd.,Yokohama, Japan).
Ⅲ.RESULTS
The examples of PCR-RFLP assays for VEGF -2578C>A, -1154G>A, -634G>C,936C>T,MTHFR 677C>T,1298A>C,TSER,andTS 3'-UTR ins/del 6bppolymorphismsareshowninFigure1-4.
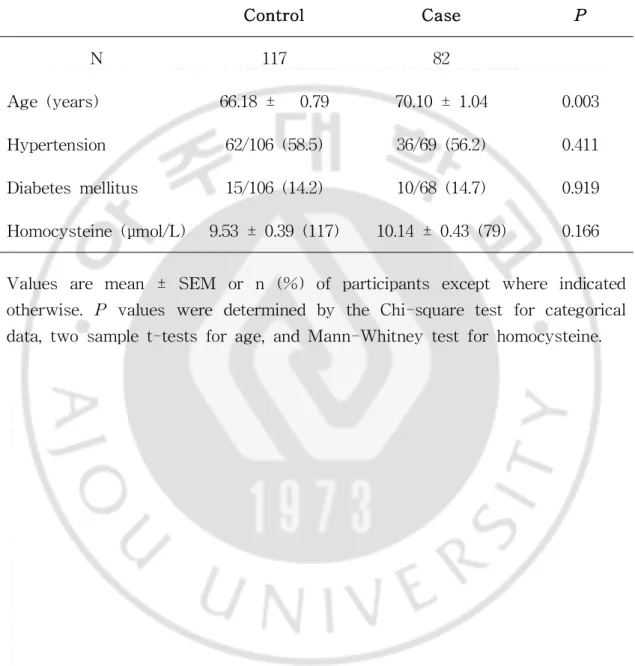
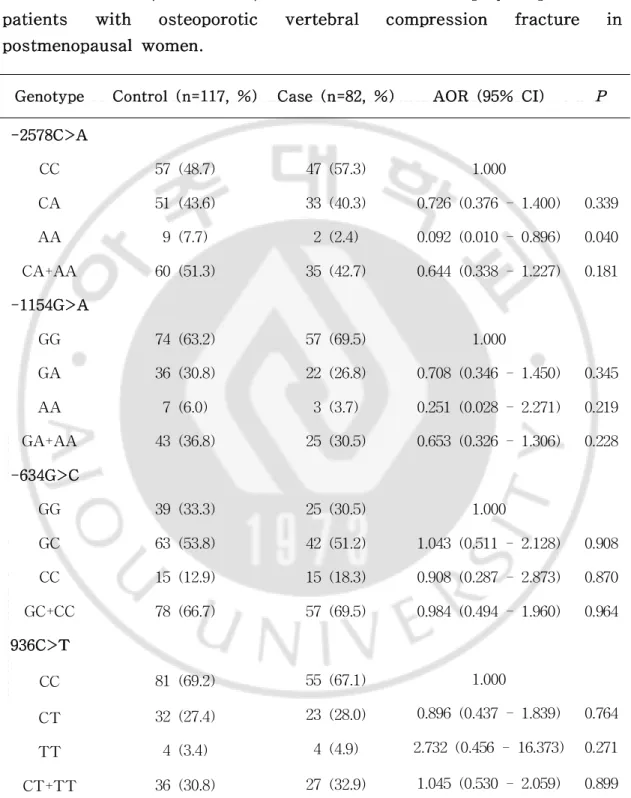
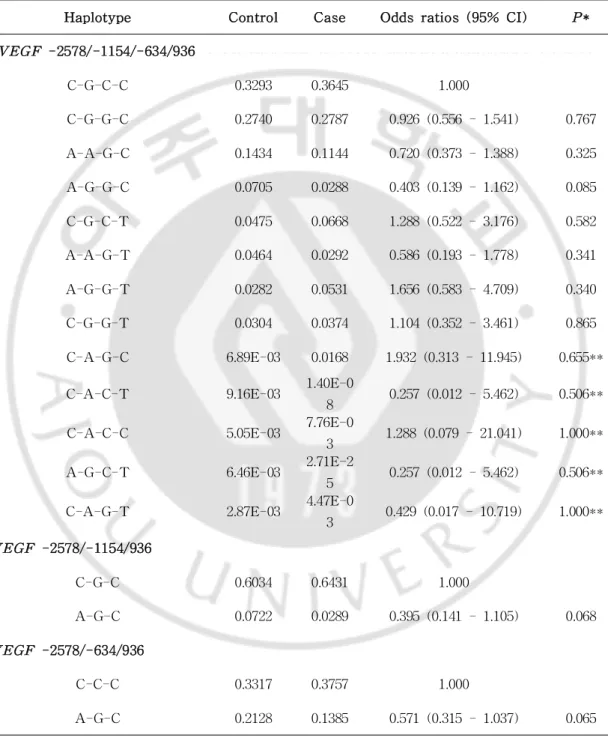
The baseline characteristics of the case and controlgroups are shown in Table2.Theagelevelsdifferedsignificantly betweenthetwogroups.TheHcy levels and the prevalence ofhypertension and diabetes mellitus did notdiffer significantly between the case and control groups.The comparison of the genotype frequencies of the VEGF -2578C>A, -1154G>A, -634G>C, and 936C>T polymorphisms between the cases and controls is shown in Table 3. TheAA genotypeofthe–2578C>A polymorphism differedsignificantlybetween the stroke and control groups.The overall genotype distributions for each polymorphism in the case and control groups were in Hardy-Weinberg equilibrium.TheA-G-G-C (-2578/-1154/-634/936)haplotypeshowedatendency to be associated with osteoporotic vertebral compression fractures in postmenopausal Korean women (p = 0.086; Table 4).Marginally significant differences were noted in the A-G-C (-2578/-1154/-634) and A-G-C (-2578/-634/936)haplotypefrequenciesoftheVEGF polymorphismsbetweenthe casesandcontrols(p=0.068andp=0.065,respectively;Table4).
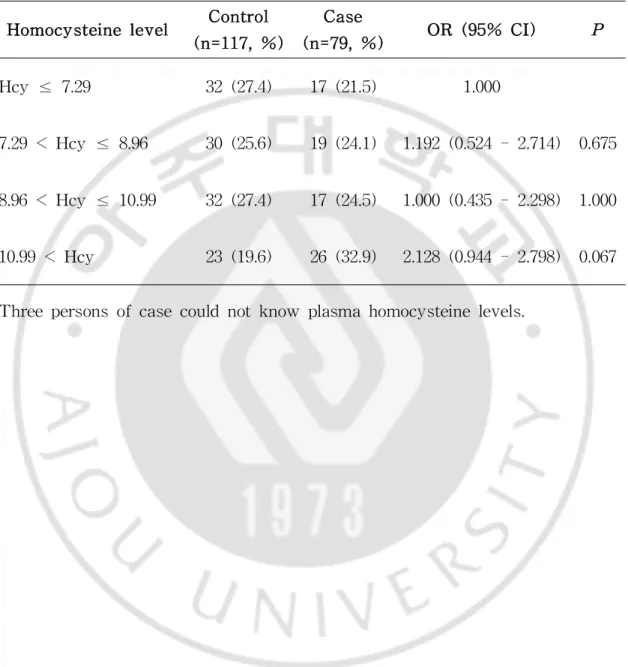
The author also attempted to determine whether or not the VEGF polymorphisms affected the levelof Hcy in the study subjects.The results demonstrated that the levels of Hcy were increased in cases with the CC genotypeoftheVEGF -2578C>A polymorphism andthatthereweresignificant differences in Hcy levels among the controls with the various genotypes (p = 0.020;Table5).When dividedby quartilesoftheplasmaHcy levelin thetotal sample,the quartile with the highest Hcy leveldid not differ significantly
betweenthecaseandcontrolgroups(p> 0.05;Table6).
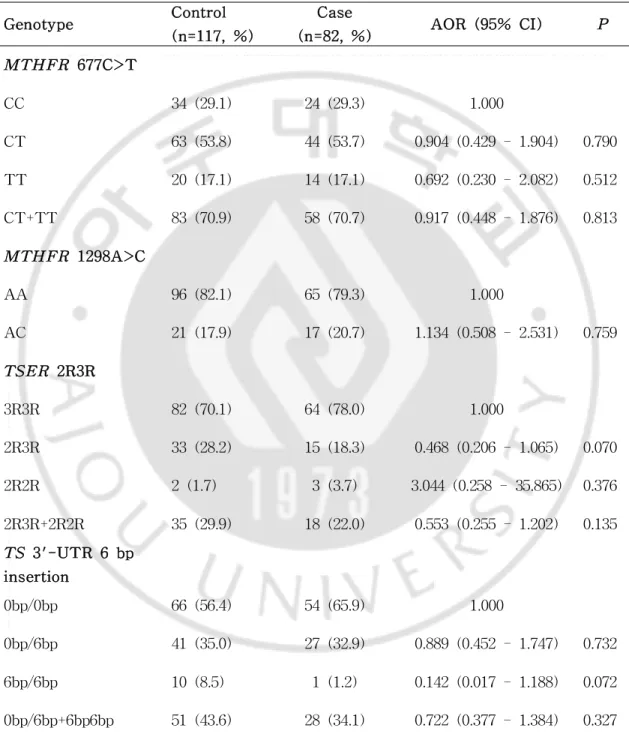
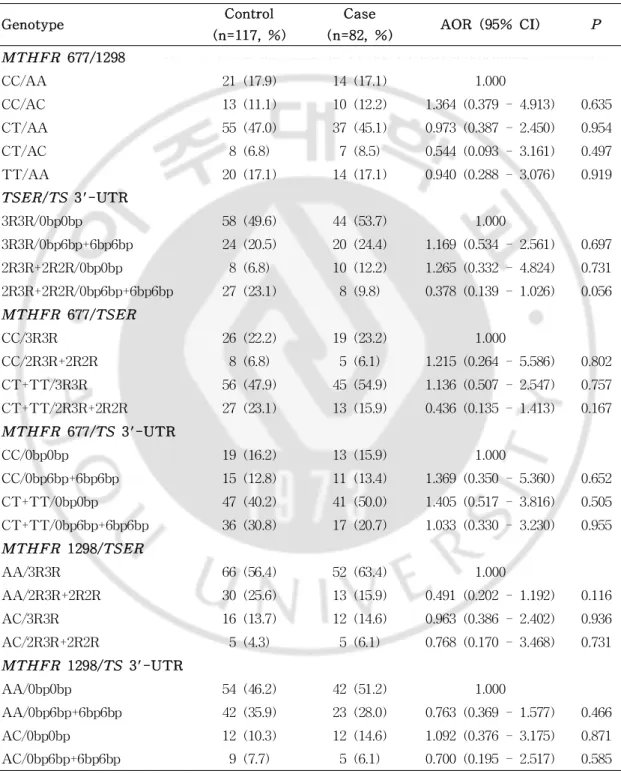
Thisstudy also attempted todeterminewhetherornottheMTHFR and TS polymorphisms affected the occurrence of osteoporotic vertebral compression fractures.However,MTHFR andTS werenotassociatedinanydetectableway withosteoporoticvertebralcompressionfractures(Table7,8).
Figure1.PCR-RFLP analysisofVEGF -2578C>A (A)and -1154G>A (B) polymorphisms.
Figure 2.PCR-RFLP analysis ofVEGF -634G>C (A) and 936C>T (B) polymorphisms.
Figure3.PCR-RFLP analysisofM THFR 677C>T (A)and1298A>C (B) polymorphisms.
Figure 4. PCR-RFLP analysis of TSER (A) and TS 3'-UTR (B) polymorphisms.
Table 2. Baseline characteristic in vertebral compression fracture patientsandcontrolsubjects.
Control Case P
N 117 82
Age(years) 66.18± 0.79 70.10± 1.04 0.003 Hypertension 62/106(58.5) 36/69(56.2) 0.411 Diabetesmellitus 15/106(14.2) 10/68(14.7) 0.919 Homocysteine(μmol/L) 9.53± 0.39(117) 10.14± 0.43(79) 0.166 Values are mean ± SEM or n (%)ofparticipants exceptwhere indicated otherwise.P values were determined by the Chi-square testforcategorical data,twosamplet-testsforage,andMann-Whitneytestforhomocysteine.
Table 3.Odds ratios (OR) and 95% confidence intervals (CI) of the VEGF -2578C>A,-1154G>A,-634G>C and 936C>T polymorphisms in patients with osteoporotic vertebral compression fracture in postmenopausalwomen.
Genotype Control(n=117,%) Case(n=82,%) AOR (95% CI) P
-2578C>A CC 57(48.7) 47(57.3) 1.000 CA 51(43.6) 33(40.3) 0.726(0.376-1.400) 0.339 AA 9(7.7) 2(2.4) 0.092(0.010-0.896) 0.040 CA+AA 60(51.3) 35(42.7) 0.644(0.338-1.227) 0.181 -1154G>A GG 74(63.2) 57(69.5) 1.000 GA 36(30.8) 22(26.8) 0.708(0.346-1.450) 0.345 AA 7(6.0) 3(3.7) 0.251(0.028-2.271) 0.219 GA+AA 43(36.8) 25(30.5) 0.653(0.326-1.306) 0.228 -634G>C GG 39(33.3) 25(30.5) 1.000 GC 63(53.8) 42(51.2) 1.043(0.511-2.128) 0.908 CC 15(12.9) 15(18.3) 0.908(0.287-2.873) 0.870 GC+CC 78(66.7) 57(69.5) 0.984(0.494-1.960) 0.964 936C>T CC 81(69.2) 55(67.1) 1.000 0.896(0.437-1.839) 0.764 23(28.0) 32(27.4) CT 2.732(0.456-16.373) 0.271 4(4.9) 4(3.4) TT 1.045(0.530-2.059) 0.899 27(32.9) 36(30.8) CT+TT
Table4.FrequenciesoftheVEGF -2578C>A,-1154G>A,-634G>C and 936C>T haplotypes in patients with osteoporotic vertebralcompression fracturein postmenopausalwomen.
Haplotype Control Case Oddsratios(95% CI) P*
VEGF -2578/-1154/-634/936 C-G-C-C 0.3293 0.3645 1.000 C-G-G-C 0.2740 0.2787 0.926(0.556-1.541) 0.767 A-A-G-C 0.1434 0.1144 0.720(0.373-1.388) 0.325 A-G-G-C 0.0705 0.0288 0.403(0.139-1.162) 0.085 C-G-C-T 0.0475 0.0668 1.288(0.522-3.176) 0.582 A-A-G-T 0.0464 0.0292 0.586(0.193-1.778) 0.341 A-G-G-T 0.0282 0.0531 1.656(0.583-4.709) 0.340 C-G-G-T 0.0304 0.0374 1.104(0.352-3.461) 0.865 C-A-G-C 6.89E-03 0.0168 1.932(0.313-11.945) 0.655**
C-A-C-T 9.16E-03 1.40E-0
8 0.257(0.012-5.462) 0.506**
C-A-C-C 5.05E-03 7.76E-0
3 1.288(0.079-21.041) 1.000**
A-G-C-T 6.46E-03 2.71E-2
5 0.257(0.012-5.462) 0.506**
C-A-G-T 2.87E-03 4.47E-0
3 0.429(0.017-10.719) 1.000** VEGF -2578/-1154/936 C-G-C 0.6034 0.6431 1.000 A-G-C 0.0722 0.0289 0.395(0.141-1.105) 0.068 VEGF -2578/-634/936 C-C-C 0.3317 0.3757 1.000 A-G-C 0.2128 0.1385 0.571(0.315-1.037) 0.065
Table 5. Comparison of homocysteine levels according to VEGF -2578C>A polymorphism in thecaseandcontrols.
Genotype Control(n=117,%) Case(n=79,%) P** -2578C>A
CC 8.64± 0.39(57) 10.33± 0.63(45) 0.020 CA 10.49± 0.74(51) 9.82± 0.57(32) 0.936† AA 9.71± 1.16(9) 10.93± 1.85(2) 0.658
P* 0.325 0.765
HomocysteinelevelswerenotsignificantlydifferentintheVEGF –1154,-634 and936polymorphismsbetweencasesandcontrols,respectively.
*one-wayANOVA test **t-test †Mann-Whitneytest
Table 6. Relative risks of the patients with osteoporotic vertebral compression fractureby quartileofplasmahomocysteinelevel.
Homocysteinelevel Control (n=117,%) Case (n=79,%) OR (95% CI) P Hcy≤ 7.29 32(27.4) 17(21.5) 1.000 7.29< Hcy≤ 8.96 30(25.6) 19(24.1) 1.192(0.524-2.714) 0.675 8.96< Hcy≤ 10.99 32(27.4) 17(24.5) 1.000(0.435-2.298) 1.000 10.99< Hcy 23(19.6) 26(32.9) 2.128(0.944-2.798) 0.067 Threepersonsofcasecouldnotknow plasmahomocysteinelevels.
Table 7.Odds ratios (OR) and 95% confidence intervals (CI) of the M THFR and TS polymorphisms in patients with osteoporotic vertebral compression fracturein postmenopausalwomen.
Genotype Control (n=117,%) Case (n=82,%) AOR (95% CI) P M THFR 677C>T CC 34(29.1) 24(29.3) 1.000 CT 63(53.8) 44(53.7) 0.904(0.429-1.904) 0.790 TT 20(17.1) 14(17.1) 0.692(0.230-2.082) 0.512 CT+TT 83(70.9) 58(70.7) 0.917(0.448-1.876) 0.813 M THFR 1298A>C AA 96(82.1) 65(79.3) 1.000 AC 21(17.9) 17(20.7) 1.134(0.508-2.531) 0.759 TSER 2R3R 3R3R 82(70.1) 64(78.0) 1.000 2R3R 33(28.2) 15(18.3) 0.468(0.206-1.065) 0.070 2R2R 2(1.7) 3(3.7) 3.044(0.258-35.865) 0.376 2R3R+2R2R 35(29.9) 18(22.0) 0.553(0.255-1.202) 0.135 TS 3'-UTR 6bp insertion 0bp/0bp 66(56.4) 54(65.9) 1.000 0bp/6bp 41(35.0) 27(32.9) 0.889(0.452-1.747) 0.732 6bp/6bp 10(8.5) 1(1.2) 0.142(0.017-1.188) 0.072 0bp/6bp+6bp6bp 51(43.6) 28(34.1) 0.722(0.377-1.384) 0.327 Adjustedbyage,hypertension,diabetesmellitusandhomocysteine.
Table 8. Combination genotype frequencies of MTHFR and TS polymorphisms in patients with osteoporotic vertebral compression fracturein postmenopausalwomen.
Genotype Control
(n=117,%) Case (n=82,%) AOR (95% CI) P MTHFR 677/1298 CC/AA 21(17.9) 14(17.1) 1.000 CC/AC 13(11.1) 10(12.2) 1.364(0.379-4.913) 0.635 CT/AA 55(47.0) 37(45.1) 0.973(0.387-2.450) 0.954 CT/AC 8(6.8) 7(8.5) 0.544(0.093-3.161) 0.497 TT/AA 20(17.1) 14(17.1) 0.940(0.288-3.076) 0.919 TSER/TS 3'-UTR 3R3R/0bp0bp 58(49.6) 44(53.7) 1.000 3R3R/0bp6bp+6bp6bp 24(20.5) 20(24.4) 1.169(0.534-2.561) 0.697 2R3R+2R2R/0bp0bp 8(6.8) 10(12.2) 1.265(0.332-4.824) 0.731 2R3R+2R2R/0bp6bp+6bp6bp 27(23.1) 8(9.8) 0.378(0.139-1.026) 0.056 MTHFR 677/TSER CC/3R3R 26(22.2) 19(23.2) 1.000 CC/2R3R+2R2R 8(6.8) 5(6.1) 1.215(0.264-5.586) 0.802 CT+TT/3R3R 56(47.9) 45(54.9) 1.136(0.507-2.547) 0.757 CT+TT/2R3R+2R2R 27(23.1) 13(15.9) 0.436(0.135-1.413) 0.167 MTHFR 677/TS 3'-UTR CC/0bp0bp 19(16.2) 13(15.9) 1.000 CC/0bp6bp+6bp6bp 15(12.8) 11(13.4) 1.369(0.350-5.360) 0.652 CT+TT/0bp0bp 47(40.2) 41(50.0) 1.405(0.517-3.816) 0.505 CT+TT/0bp6bp+6bp6bp 36(30.8) 17(20.7) 1.033(0.330-3.230) 0.955 MTHFR 1298/TSER AA/3R3R 66(56.4) 52(63.4) 1.000 AA/2R3R+2R2R 30(25.6) 13(15.9) 0.491(0.202-1.192) 0.116 AC/3R3R 16(13.7) 12(14.6) 0.963(0.386-2.402) 0.936 AC/2R3R+2R2R 5(4.3) 5(6.1) 0.768(0.170-3.468) 0.731 MTHFR 1298/TS 3'-UTR AA/0bp0bp 54(46.2) 42(51.2) 1.000 AA/0bp6bp+6bp6bp 42(35.9) 23(28.0) 0.763(0.369-1.577) 0.466 AC/0bp0bp 12(10.3) 12(14.6) 1.092(0.376-3.175) 0.871 AC/0bp6bp+6bp6bp 9(7.7) 5(6.1) 0.700(0.195-2.517) 0.585
Ⅳ.DI
SCUSSI
ON
Angiogenesis is indispensable during fracture repair,and VEGF performs a criticalfunction in this process.Severalauthors havesuggested thatVEGF is involved in bonemetabolism (Akeno etal.,2001;Uchida etal.,2003;Komatsu and Hadjiargyrou,2004;Eckardtetal.,2005;Geigeretal.,2005,2007;Streetet al.,2007).Hypoxia induces VEGF gene transcription.The transcription factors forVEGF,hypoxiainduciblefactor-1 (HIF-1a),andHIF-2a,areknowntobe involved in bone regeneration.VEGF is expressed,along with its receptors, during thehealing processofboneand bonemarrow afterdrill-holeinjuriesin rats.Boneregeneration isenhanced by theVEGF-induced up-regulation ofthe CCN1andVEGF gene-activatedmatrix.
SequencechangesinthepromoterandUTR ofthegeneareimportantforthe regulation of gene transcription or translation. Previous studies have demonstrated thatpolymorphisms in the VEGF gene promoter are associated with production oftheVEGF protein (Brogan etal.,1999;Watson etal.,2000; Mohammadi et al., 2003). For example, the -2578C>A polymorphism may influence the level of transcription and may result in differences in the production ofthe VEGF protein between individuals.Thus,this polymorphism may contribute to differences in the susceptibility to and severity ofvertebral compressionfracturesbetweenindividuals.
The results ofthis study showed thatthe polymorphisms and haplotypes of the VEGF gene were associated with vertebral compression fractures.The VEGF -2578C>A,-1154G>A,-634G>C,and 936C>T polymorphic sites are locatedwithin thepromoterandUTR regions.Thehaplotypedatain thisstudy indicate that a low linkage disequilibrium between polymorphisms in the promoter and in the 3’-UTR of the VEGF gene.Haplotypes of the VEGF
polymorphisms may influence the susceptibility to diseases.For example,the C-C haplotype of the VEGF -2578C>A and -634G>C polymorphisms was associatedwithahighdegreeoftumoraggressiveness(Jinetal.,2005).Forthe -2578C>A,-1154G>A,and -634G>C polymorphisms,theC-A-C haplotypewas associatedwithlessadvancedmelanoma(Howelletal.,2002).
The study of an association between four SNPs (-2578C>A,-1154G>A, -634G>C,and 936C>T)ofthe VEGF gene and diseases have generally been thesubjectofcloseattentionasVEGF mutanttypesareusuallyassociatedwith decreased VEGF production. However, VEGF -2578AA exerts a protective effect. The reasons for the discrepancy in the research results may be multifarious,anddifferencesin allelefrequenciesbetween ethnicgroupsmay be oneoftheprincipalreasonsforthis.
Osteoporosis and low bone mineral density (BMD) commonly occur in postmenopausalwomen,and can resultin increased susceptibility to fractures. BMD and many otherfactorshavebeen shown tocontributetoskeletalhealth. One such factor,Hcy,influences osteoporosis,although this influence does not apply to all populations.For example,the level of plasma total Hcy was associated with the risk of hip fractures and BMD in the Hordaland Homocysteine Study (Gjesdalet al.,2006).Associations between Hcy levels, boneturnover,BMD,mortality,andfractureriskhavealsobeennotedinstudies ofelderly women (McLean etal.,2004;van Meurs etal.,2004;Morris etal., 2005;Gerdhem etal.,2007),and the results ofthis study corroborated these associations.Indeed,there were more cases than controls in the quartile with the highest Hcy levels; however, this was not a statistically significant difference.The mechanisms thus far suggested to explain the effectofHcy include impaired bone collagen formation by Hcy and increased osteoclast activity (Cagnaccietal.,2008).Severalstudies have identified levels ofHcy,
particularly those in the upper quartile, as an independent risk factor for osteoporoticfractures(van Meursetal.,2004;McLean etal.,2004;Satoetal., 2005).
Hcyinhibitsangiogenesisunderbothinvitroandinvivoconditions(Nagaiet al.,2001).Hcy also increases the expression of VEGF through endoplasmic reticulum stressand induction ofthetranscription factor,ATF4 (Roybaletal., 2004).Hcy hasalso been shown to increaseVEGF expression in differentiated THP-1 macrophages (Maeda etal.,2003).In the currentstudy,a significant differencein Hcy levelswasnotedbetween thecasesandcontrolswiththeCC genotypeoftheVEGF –2578C>A polymorphism;thisindicatesthattheVEGF –2578C>A polymorphism may affectthelevelofHcy.Thedifferencesin Hcy levelsamong ethnic populations may be caused by environmentalfactors,such asdietary habitsandlifestyle.However,in addition toenvironmentalinfluences, Hcy levels may also be controlled by genetic factors,including the genetic background.Baines etal.(2007)suggested thatthe MTHFR polymorphism is associated with Hcy levels in postmenopausal British women.However,no association ofMTHFR with osteoporoticfractureswasindicated in thedataof thecurrentstudy;theosteoporoticfracturepatientsmay havean unknown Hcy metabolism byVEGF.
Ⅴ.CONCLUSI
ON
In conclusion,thisstudy providesevidenceforan association between VEGF polymorphisms and the risk ofosteoporotic vertebralcompression fractures in postmenopausalwomen in the current study population.In particular,VEGF -2578AA was a protective marker in our study,because -2578CC induced a higherconcentration ofhomocysteinein thepatientgroup.In thepatientgroup, the TSER,2R3R+2R2R/TS,3'-UTR and 0bp6bp+6bp6bp combination genotype was found to be of marginal significance. Its significance may fluctuate according tosamplesize.Therefore,largeprospectiveandheterogeneousstudies willbenecessary tosupportthefindingsofthisstudy.Theauthoriscurrently testing this hypothesis and assessing the associations among VEGF gene polymorphisms,fractureriskanddietaryintakeormetabolicsyndrome.
REFERENCES
1.Akeno N,Czyzyk-Krzeska MF,Gross TS,Clemens TL:Hypoxia induces vascular endothelial growth factor gene transcription in human osteoblast-like cells through the hypoxia-inducible factor-2⍺. Endocrinology142:959-962,2001
2.Bae SJ,Ahn DH,Hong SP,Kang H,Hwang SG,Oh D,Kim NK: Gender-specific association between polymorphism ofvascular endothelial growth factor (VEGF 936C>T) gene and patients with stomach cancer. YonseiMedJ49:783-791,2008
3.Baines M,Kredan MB,UsherJ,Davison A,Higgins G,TaylorW,West C,Fraser WD,Ranganath LR:The association ofhomocysteine and its determinants MTHFR genotype,folate,vitamin B12 and vitamin B6 with
bonemineraldensity in postmenopausalBritish women.Bone 40:739-736, 2007
4.Brogan IJ,Khan N,Isaac K,Hutchinson JA,Pravica V,Hutchinson IV: Novelpolymorphism in the promoterand 5’UTR regions ofthe human vascular endothelial growth factor gene.Hum Immunol 60: 1245-1249, 1999
5.CagnacciA,BagniB,ZiniA,CannolettaM,GeneraliaM,VolpeA:density change in postmenopausal women. A five-year longitudinal evaluation. Bone42:314-320,2008
6.Center JR, Nguyen TV, Schneider D, Sambrook PN, Elsaman JA: Mortality afterallmajortypesofosteoporoticfractureinmen andwomen: anobservationalstudy.Lancet353:878-882,1999
Mann D,LambertJC:Association study ofthevascularendothelialgrowth factor gene with the risk of developing Alzheimer disease. Neurobio Aging 27:1212-1215,2006
8.Costa N,Paramanathan S,MacDonald D,WierzbickiAS,Hampson G: Factors regulating circulating vascularendothelialgrowth factor (VEGF): Association with bone mineral density (BMD) in post-menopausal osteoporosis.Cytokine46:376-381,2009
9.DaiJ,Rabie AB VEGF:An essentialmediatorofboth angiogenesis and endochondralossification.JDentRes86:937-950,2007
10.Dequeker J, Nijs J, Verstraeten A, Geusens P, Gevers G: Genetic determinants of bone mineralcontentatthe spine and radius:a twin study.Bone8:207-209,1987
11.Eckardt H, Ding M, Lind M, Hansen ES, Christensen KS, Hvid I: Recombinant human vascular endothelial growth factor enhances bone healing in an experimental nonunion model. J Bone Joint Surg 87: 1434-1438,2005
12.Esbrit P,Alvarez-Arroyo VA,DeMiguel F,Martin O,Martinez ME, Caramelo C: C-terminal parathyroid hormone-related protein increases vascular endothelialgrowth factor in human osteoblastic cells.J Am SocNephrol11:1085-1092,2000
13.GeigerF,Bertram H,BergerI,Lorenz H,WallO,EckhardtC,Simank HG,RichterW:Vascularendothelialgrowth factorgene-activated matrix (VEGF165-GAM) enhances osteogenesis and angiogenesis in large
segmentalbonedefects.JBoneMinerRes20:2028-2035,2005
14.Geiger F,Lorenz H,Xu W,Szalay K,Kasten P,Claes L,Augat P, RichterW:VEGF producing bonemarrow stromalcells(BMSC)enhance vascularization andresorption ofanaturalcoralbonesubstitute.Bone41:
516-522,2007
15.Gerdhem P,IvaskaKK,Isaksson A,Pettersson K,Vaananen HK,Obrant KJ:Associations between homocysteine,bone turnover,BMD,mortality, andfractureriskinelderlywomen.JBoneMinerRes22:127-134,2007 16.GjesdalCG,VollsetSE,Ueland M,Refsum H,Drevon CA,Gjessing HK,
TellCG:Plasma totalhomocysteine leveland bone mineraldensity:the HordalandHomocysteineStudy.ArchInternMed166:88-94,2006
17.Herrmann M, Widmann T, Herrmann W: Homocysteine-a newly recognised risk factor for osteoporosis. Clin Chem Lab Med 43: 1111-1117,2005
18.Howell WM, Bateman AC, Turner SJ, Collins A, Theaker JM: Influence of vascular endothelial growth factor single nucleotide polymorphismson tumourdevelopmentin cutaneousmalignantmelanoma. GenesImmunol3:229-232,2002
19.HyderSM,NawazZ,ChiappttaC,StancelGM:Identificationoffunctional estrogen response elementsin thegene coding forthepotentangiogenic factorvascularendothelialgrowthfactor.CancerRes60:3183-3190,2000 20.Iruela-Arispe ML, Dvorak HF: Angiogenesis: a dynamic balance of
stimulatorsandinhibitors.ThrombHaemost78:672-677,1997
21.JacobsEJ,Feigelson HS,Bain EB,Brady KA,RodriguezC,StevensVL, PatelAV,Thun MJ,CalleEE:Polymorphismsin thevascularendothelial growth factorgene and breastcancerin the cancerprevention study II cohort.BreastCancerRes8:R22,2005
22.Jin Q,Hemminki K,Enquist K,Lenner P,Grzybowska E,Klaes R, Henriksson R, Chen B, Pamula J, Pekala W, Zientek H, Rogozinska-Szczepka J, Utracka-Hutka B, Hallmans G, Forsti A:
Vascular endothelialgrowth factor polymorphisms in relation to breast cancerdevelopmentandprognosis.ClinCancerRes11:3647-3653,2005 23.Kim NK,ChoiYK,Kang MS,ChoiDH,ChaSH,An MO,LeeS,Jeung
M, Ko JJ, Oh D: Influence of combined methylenetetrahydrofolate reductase (MTHFR) and thymidylate synthase enhancer region (TSER) polymorphisms to plasma homocysteine levels in Korean patients with recurrentspontaneousabortion.ThrombRes117:653-658,2006
24.KomatsuDE,HadjiargyrouM:ActivationofthetranscriptionfactorHIF-1 anditstargetgenes,VEGF,HO-1,iNOS,duringfracturerepair.Bone34: 680-688,2004
25.Ladoux A,Frelin C:Expression ofvascularendothelialgrowth factorby cultured endothelialcells from brain microvessels.Biochem Biophys Res Commun194:799-803,1993
26.Lambrechts D,Storkebaum E,Morimoto M,Del-Favero J,Desmet F, MarklundS,WynsS,ThijsV,AnderssonJ,vanMarionI,Al-ChalabiA, BornesS,Musson R,HansenV,BeckmanL,AdolfssonR,PallHS,Prats H, Vermeire S, Rutgeerts P, Katayama S, Awata T, Leigh N, Lang-Lazdunski L, Dewerchin M, Shaw C, Moons L, Vlietinck R, Morrison KE,RobberechtW,Van Broeckhoven C,Collen D,Andersen PM,CarmelietP.:VEGF isamodifierofamyotrophiclateralsclerosisin mice and humans and protects motoneurons againstischemic death.Nat Genet34:383-394,2003
27.LeeHH,Hong SH,Shin SJ,KoJJ,Oh D,Kim NK:Associationstudy of vascular endothelial growth factor polymorphisms with the risk of recurrentspontaneousabortion.FertilSteril93:1244-1247,2010
28.Liu J,SchmitzJC,Lin X,TaiN,Yan W,FarrellM,Bailly M,Chen T, Chu E:Thymidylatesynthaseasatranslationalregulatorofcellulargene expression.Biochim BiophysActa.1587:174-182,2002
29.Livak KJ: Allelic discrimination using fluorogenic probes and the 5’ nucleaseassay.GenetAnal1999:143-149,1999
30.MaedaM,YamamotoI,FujioY,AzumaJ:Homocysteineinducesvascular endothelialgrowth factorexpression in differentiatedTHP-1macrophages. Biochim BiophysActa1623:41-46,2003
31.McGuigan FE, Ralston SH: Single nucleotide polymorphism detection: allelicdiscriminationusingTaqMan.PsychiatricGenet12:133-136,2002 32.McLean RR,Jacques PF,Selhub J,TuckerKL,Samelson EJ,Broe KE,
Hannan MT,Cupples LA,KielDP:Homocysteine as a predictive factor forhipfractureinolderpersons.N Eng JMed350:2042-2049,2004 33.MohammadiM,OllierWE,Hutchinson IV:A functionalassociation study
of VEGF gene promoter polymorphism with VEGF expression by stimulatedpbm cells.Hum Immunol64(Suppl):S125,2003
34.Morris MS,Jacques PF,Selhub J:Relation between homocysteine and B-vitamin statusindicatorsand bonemineraldensity in olderAmericans. Bone37:234-242,2005
35.NagaiY,TasakiH,Takatsu H,NiheiS,Yamashita K,Toyokawa T, Nakashima Y:Homocysteine inhibits angiogenesis in vitro and in vivo. Biochem BiophysResCommun281:726-731,2001
36.NIH ConsensusDevelopmentPanelon OsteoporosisPrevention,Diagnosis, and Therapy:Osteoporosisprevention diagnosisand therapy.JAMA 285: 785-795,2001
37.Pantsulaia I, Trofimov S, Kobyliansky E, Livshits G: Heritability of circulating growth factorsinvolved in theangiogenesisin healthy human population.Cytokine27:152-158,2004
38.Papazoglou D, Galazios G, Papatheodorou K, Liberis V, Papanas N, Maltezos E, Maroulis GB: Vascular endothelial growth factor gene polymorphisms and idiopathic recurrentpregnancy loss.FertilSteril83: 959-963,2005
39.Park HM,Hong SH,Kim JW,Oh D,Hwang SG,An HJ,Kim UK,Kim NK:Gender-specificassociation oftheVEGF -2578C>A polymorphism in Koreanpatientswithcoloncancer.AnticancerRes27:2535-2540,2007 40.Pocock NA,Eisman JA,HopperJL,YeatesMG,Sambrook PN,EberlS:
Genetic determinants of bone mass in adults: A twin study.J Clin Invest80:706-710,1987
41.PouillèsJM,TrémollièresF,BonneuM,RibotC:Influenceofearlyageat menopauseonvertebralbonemass.JBoneMinerRes9:311-315,1994 42.RennerW,Kotschan S,Hoffmann C,Obermayer-Pietsch B,PilgerE: A
common 936 C/T mutation in the gene forvascular endothelialgrowth factorisassociatedwith vascularendothelialgrowth factorplasmalevels. JVascRes37:443-448,2000
43.Roybal CN,Yang S,Sun CW,Hurtado D,Jagt DLV,Townes TM, Abcouwer SF:Homocysteine increases the expression of VEGF by a mechanism involving endoplasmicreticulum stressandtranscription factor ATF4.JBiolChem 279:14844-14852,2004
44.Sato Y,Honda Y,Iwamoto J,Kanoko T,Satoh K:Homocysteine as a predictive factor for hip fracture in stroke patients.Bone 36:721-726, 2005
45.SengerDR,van de WaterL,Brown LF,Nagy JA,Yeo KT,Teo TK, Berse B,Jackman RW,Dvorak AM,Dvorak AF:Vascular permeability factor (VPF, VEGF) in tumor biology. Cancer Metastasis Rev 12: 303-324,1993
46.ShahbaziM,FryerAA,Pravica V,Brogan IJ,Ramsay HM,Hutchinson IV,Harden PN:Vascularendothelialgrowth factorgene polymorphisms are associated with acute renalallograftrejection.J Am Soc Nephrol 13:260-264,2002
47.Slemenda CW,Christian JC,Williams CJ,Norton JA,Johnson Jr CC: Genetic determinants ofbone mass in adults women:a reevaluation of thetwinmodelandpotentialimportanceofgeneinteractiononheritability estimates.JBoneMinerRes6:561-567,1991
48.Street J,Bao M,deGuzman L,Bunting S,Peale Jr FV,Ferrara N, Steinmetz K, Hoeffel J, Cleland JL, Daugherty A, van Bruggen N, Redmond HP, Carano RA, Filvaroff EH: Vascular endothelial growth factor stimulates bone repair by promoting angiogenesis and bone turnover.ProcNatlAcadSciUSA 99:9656-9661,2002
49.Trinh BN, Ong CN, Coetzee GA, Yu MC, Laird PW: Thymidylate synthase:a novelgeneticdeterminantofplasma homocysteineand folate levels.Hum Genet111:299-302,2002
50.Uchida S, Sakai A, Kudo H, Otomo H, Watanuki M, Tanaka M, Nagashima M, Nakamura T: Vascular endothelial growth factor is expressedalong withitsreceptorsduring thehealing processofboneand bonemarrow afterdrill-holeinjuryinrats.Bone32:491-501,2003
51.van MeursJBJ,Dhonukshe-Rutten RAM,Pluijm SMF,van derKliftM, de Jonge R,Lindemans J,de GrootLC,Hofman A,Witteman JC,van Leeuwen JP, Breteler MM, Lips P, Pols HA, Uitterlinden AG: Homocysteine levels and the risk of osteopototic fracture.N Eng J Med350:2033-2041,2004
52.Villadsen MM, Bunger MH, Carstens M, Stenkjaer L, Langdahl BL Methylene-tetrahydrofolate reductase (MTHFR) C677T polymorphism is associated with osteoporotic vertebralfractures,butis a weak predictor
ofBMD.OsteoporosInt16:411-416,2005
53.Watson CJ,Webb NJA,Bottomley MJ,Brenchley PEC: Identification of polymorphisms within the vascular endothelial growth factor gene: correlation with variation in VEGF protein production. Cytokine 12: 1232-1235,2000
54.Yim DJ,Kim OJ,An HJ,Kang H,Ahn DH,Hwang SG,Oh D,Kim NK Polymorphisms of thymidylate synthase gene 5'- and 3'-untranslated region and risk of gastric cancer in Koreans. Anticancer Res 30: 2325-2330,2010
국문요약
-폐경 후 골다공성 척추압박골절 환자의
유전자 다형 관련성
아주대학교 대학원 의학과 정 영 선 (지도교수:조 기 홍)혈관내피세포 성장인자 (Vascularendothelialgrowth factor;VEGF) 는 혈관신생 (angiogenesis)을 통한 골 형성에 관여하며 골절의 치유를 촉진한다.고 호모시스테인혈증 (hyperhomocysteinemia)은 골다공증,뼈 의 무기질 밀도의 저하 및 골절 등과 같은 골격계에 문제를 일으키는 위 험인자로 알려져 있다. 5, 10-methylenetetrahydrofolate reductase (MTHFR)와 thymidylatesynthase (TS)효소는 모두 호모시스테인 대 사과정에 관여한다.따라서 본 연구자는 VEGF,MTHFR 및 TS의 유전 자 다형 (polymorphism)이 한국여성의 폐경 후 골다공성 척추 압박골절 (osteoporotic vertebralcompression fracture;OVCF)과 관련이 있는지 알아보고자 하였다.한국여성의 폐경 후 골다공성 척추 압박골절 환자 82명과 골절이 없는 폐경 후 여성 117명을 대조군으로 하여 실시하였다. VEGF, MTHFR 및 TS 유전자 다형을 polymerase chain reaction -restriction fragmentlength polymorphism (PCR-RFLP)와 real-time PCR을 통하여 분석하였다.VEGF 유전자의 다형이 호모시스테인/엽산
(homocysteine/folate)대사에 영향을 주는지 여부를 혈중 호모시스테인 농도를 측정하여 확인하였다.VEGF -2578C>A 다형 중 -2578AA 유전 자형 (genotype)이 대조군에 비해 통계적으로 의미 있는 차이를 보였다. VEGF -1154G>A,-634G>C와 936C>T 유전자 다형에서는 별다른 차이 를 보이지 않았다.그런데 A-G-G-C 일배체유전자형 (haplotype)은 한 국여성의 폐경 후 골다공성 척추 압박골절의 발병에 관련된 경향을 발견 하였다.그리고 VEGF -2578C>A 유전자 다형은 혈중 호모시스테인 농 도와도 연관되어 있었다.그러나 MTHFR과 TS 유전자 다형은 골다공 성 척추 압박골절과의 관련성은 발견할 수 없었다.결론적으로,VEGF -2578C>A 유전자 다형과 일부 일배체 유전자 (A-G-G-C)은 한국여성 의 폐경 후 골다공성 척추 압박골절 발병 위험인자로 중요한 역할을 한 다고 할 수 있겠다. _____________________________________________________________ 핵심어:혈관내피성장인자,골다공성 척추 압박골절,폐경여성,유전자 다형,호모시스테인