서 론
인체에 의료 방사선의 피폭을 예방하고, 불필요한 방사선 을 최소화하기 위해 차폐물질을 사용하고 있으며, 방사선을 차폐하는 이유는 생식선을 보호하고, 피폭선량을 최소화시 켜야 하기 때문이다. 임상에서 엑스선 및 방사선을 이용하 는 영상의학과 전문의나 방사선사 그리고 환자에게 방사선 의 피폭이 잠재적인 위험 요소로 인식되어 있으며 국제방 사선방어위원회(ICRP, International Committee for Radio activity Prevention)는 불필요한 방사선 피폭을 최소화하 도록 권고하고 있다(Selmaier et al. 1994). 방사선을 이용 한 검사에서 방사선 피폭을 예방하기 위해 납 소재의 차폐복과 갑상샘 보호대, 납 안경을 착용하여 방어를 하고 있다
(Strzelczyk et al. 2006; Jang et al. 2011).
방사선을 취급하는 시설에서 방사선을 차폐하기 위해서 납, 철, 콘크리트가 사용되고 있다. 검사실의 실내에서 납유
엑스선의 관전압에 따른 납유리의 방사선 선량 차폐 측정
최 지 원1· 이 선 화2· 권 대 철3,* 1전주대학교 방사선학과, 2고려대학교 대학원 바이오융합공학과, 3신한대학교 방사선학과Radiation Dose Shielding of Pb-based Glass
according to Different Tube Voltage of X-ray
Jiwon Choi
1, Seonhwa Lee
2and Dae Cheol Kweon
3,*
1Department of Radiological Science, Jeonju University2Department of Bio-convergence Engineering, Graduate School, Korea University 3Department of Radiological Science, Shinhan University
Abstract - We measure the dose of lead glass according to the change of tube voltage of X-ray and compare the shielding ability to confirm the shielding rate. The lead glass used for the X-ray shielding material was 6.5mm in thickness and 1.5mmPb in the lead equivalent. The tube voltage was measured at 60, 70, 80, 90, 100, 110, 120kVp and tube current of 10mAs. At the tube voltage of 60kVp, the dose was shielded by 90.3% and the dose rate was shielded by 89.9%. At the tube voltage of 120kVp, the dose was blocked by 31.6% and the dose rate was blocked by 34.7%. As the tube voltage increased, the shielding rate decreased. At the tube voltage of 60kVp, the dose shielding rate was as high as 90.3%, but as the tube voltage increased to 120kVp, the shielding rate decreased to 31.6%. There is a significant difference in dose depending on the use of lead glass (p-value <.05). By measuring the shielding ability of the lead glass according to the change of the tube voltage of the X-ray, the dose shielding rate was 31.6~90.3% and the dose shielding rate was 34.7~89.9%. We could confirm the shielding effect of lead glass according to the investigation of X-ray. We should make efforts to reduce the exposure by using the characteristics of lead glass by referring to these results.
Key words : Lead glass, Tube voltage, Shielding, X-ray
─ 75 ─
Technical Paper
* Corresponding author: Dae Cheol Kweon, Tel. +82318703411, Fax. +82318703419, Email. [email protected]
리 창을 통해 의사 또는 방사선사가 환자의 상태를 관찰할 때에 방사선의 피폭을 방지하기 위해 납유리가 필요하다. 이러한 의료방사선을 방어하는 차폐체의 재료는 주로 원 자번호가 높은 납, 비스무트가 이용되고 있으며, 차폐물질 은 방사선 피폭선량을 낮추기 위해 적절하게 선택하여 이용 해야 한다. 의료 방사선의 차폐체는 대표적으로 납을 사용 하는데 납유리를 사용하면 차폐가 되면서 치료받는 환자의 상태를 볼 수 있다는 장점이 있어 차폐 내부 관찰수단으로 서 차폐 벽의 창으로 사용한다. 납유리는 일반적으로 SiO2, PbO, K2O, Na2O로 구성되어 다른 원료와 함께 융해해서 제 조한다. 납유리는 저온에서 가공하여 투명도가 뛰어나고, 굴 절률이 높고, 납 함량이 높은 경우에는 방사선 차폐능력으 로 인하여 투명 차폐창으로 사용되고 있다(Lee et al. 2003). 납유리의 밀도와 두께, 사용하는 방사선의 종류와 방사선 의 에너지를 알면 차폐효율을 평가할 수 있고, 납유리의 화 학조성과 기하학적 구조 형태 등을 이용하면 정확한 평가 를 할 수 있다. 이러한 납유리는 조사된 엑스레이가 납유리 를 통과하여 감소를 일으켜 차폐효과는 통상적으로 재질의 차폐능력은 납을 기준으로 하고 있고, 납의 차폐효과를 연 당량(lead equivalent)으로 나타내고 있으며 이러한 납유리 는 차폐능력의 연당량을 확인하여야 한다. 납유리의 두께에 따라 다르지만 60kVp 이하의 방사선은 99% 이상 차폐할 수 있는 능력이 있다. 일반적으로 투과력이 큰 엑스선이나 감마선의 차폐에는 원자번호가 높고 밀도가 높을수록 방사 선의 감약이 커지므로 밀도가 큰 납, 철, 텅스텐이 사용된다 (UNSEAR 1988; Tuner 1995). 의료기관의 방사선 시설이 증가하고 있고, 방어시설 및 원격조작시스템이 투명한 납유리의 필요성이 증가하고 있 다. 차폐시설에 이용되는 납유리의 차폐능력을 평가할 필요 가 있다. 이에 본 연구에서는 엑스선의 관전압이 변화하여 조사에 따른 납유리의 방사선량을 측정하고 비교하여 차폐 율을 확인하고자 한다. 측정된 실험결과를 바탕으로 투과에 따른 차폐율을 계산하여 납유리의 차폐능력을 측정하였다.
재료 및 방법
1. 납유리 엑스선 발생장치의 납유리의 차폐율을 측정하기 위해 차 폐재에 사용한 납유리(RC, Kyungil Glass, Seoul, Korea)는 두께 6.5mm, 연당량 1.5mmPb를 사용하였다(Fig. 1). 무색투명 유리판으로 투명성을 높이고, 유리원석과 산화 연처리를 정량적으로 하여 내방사선을 유지한 납유리는 합 성과정, 두께공정, 연삭과정, 연마 후 처리 과정의 방법으로 제작한다. 엑스선의 차폐능력에 사용된 납유리의 구체적인 제원으로는 가시광선투과율 84.4%로 시험분석방법은 KS L 2514 기준을 적용하였다(Table 1). 2. 선량 측정 실험에 사용된 엑스선 발생장치는 AccuRay650R(DK Medical Systems, Seoul, Korea)로 고주파 inverter 형식의 3상 엑스선 발생장치로, 초점 크기 0.6mm, 고유여과 0.9 mmAl, 부과여과 1.5mmAl로 제조되어있다(Kweon 2017). 엑스선의 관전압을 60, 70, 80, 90, 100, 110, 120kVp, 관전 류 10mAs로 조사하여 측정하였다.엑스선의 방사선 선량은 선량계 Xi R/F(Unfors RaySafe AB, Billdal, Sweden)를 납유리 아래 테이블 위에 위치하고 엑스선을 조사하여 선량을 측정하였다(Fig. 2).
선원과 선량계 및 계측기는 45cm이고, 지면에서는 95
Fig. 1. Lead glass of 6.5mm thickness was used in the experiment.
Table 1. Specification of lead glass
Specification Details Remarks
Light transmission(380~780nm) 84.4% KS L 2514
Thickness(mm) 6.5
Equivalent(mmPb) 1.5
Fig. 2. Dosimeter set up at the Xray source. Distance of 5cm Measurement position Interval Support fixture X-ray source Lead glass 45cm 90cm
cm로 하였으며 엑스선의 관전압을 60, 70, 80, 90, 100, 110, 120kVp로 10kVp 단계로 조절하였고, 관전류는 10mAs로 모두 동일한 조건으로 엑스선으로 조사하여 선량계를 이용 하여 선량 및 선량율을 측정하였다(Fig. 3). 3. 선량차폐율 및 통계 엑스선을 납유리에 조사하여 선량 및 선량율을 측정하고, 납유리의 차폐율(η) 공식은 아래 식(1)과 같이 계산하였다. (DA-DB) η=---×100 (1) DA
Where: DA is radiation dose and dose rate as measured at the
lead glass
DB is radiation dose and dose rate as measured at the
nonlead glass
엑스선의 선량과 선량률의 통계적 분석은 SPSS version 22.0(IBM, Chicago, IL, USA)을 이용하여 시행하였고 통계 처리의 검정을 위하여 연속 변수는 paired ttest를 사용하였 고 유의수준 p<0.05로 유의성을 검증하였다.
결 과
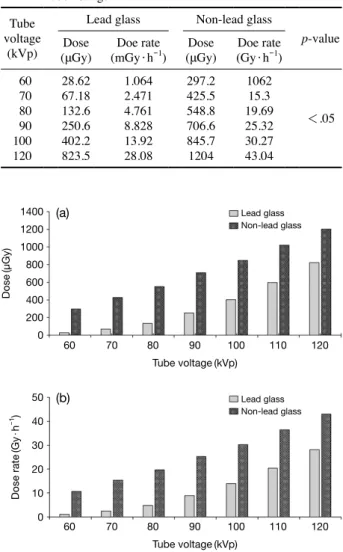
엑스선의 관전압의 변화에 따른 엑스선 조사에서 납유리 의 사용 여부에 따라 유리선량계의 선량측정 결과이다. 선 량은 관전압의 증가에 따라 선량이 증가하였으며, 납유리를 사용하면 선량이 감소하였다(Table 2). 납유리의 사용여부 에 따라 선량은 유의한 차이가 있다(pvalue <.05). 엑스선의 방사선 선량은 고정된 관전류(10mAs)와 관전 압의 10kVp 증가에 따라 납유리를 사용할 때와 사용하지 않을 때의 선량 및 선량율은 점진적으로 증가하였다(Fig. 4). 관전압의 조정에 따른 선량 및 선량율의 차폐율을 산출하 였다(Table 3). 관전압이 60kVp에서 선량은 90.3% 차폐하Fig. 3. Radiography unit and dosimeter.
Table 2. Radiation dose and dose rate according to the different tube voltage
Tube voltage
(kVp)
Lead glass Nonlead glass
pvalue
Dose
(μGy) (mGy·hDoe rate-1) (μGy)Dose (Gy·hDoe rate-1)
60 28.62 1.064 297.2 1062 <.05 70 67.18 2.471 425.5 15.3 80 132.6 4.761 548.8 19.69 90 250.6 8.828 706.6 25.32 100 402.2 13.92 845.7 30.27 120 823.5 28.08 1204 43.04
Table 3. Reduction rate of radiation dose using glass doimetry Tube voltage
(kVp) Ratio of shielding dose(%) Ratio of shielding dose rate(%)
60 90.3 89.9 70 84.2 83.4 80 75.8 75.8 90 64.5 65.1 100 52.4 54 110 41.5 44.2 120 31.6 34.7
Fig. 4. Results of radiation dose(a) and dose rate(b) using lead
glass and nonlead glass.
Dose (μGy) Tube voltage(kVp) Tube voltage(kVp) 60 70 80 90 100 110 120 60 70 80 90 100 110 120 Lead glass Non-lead glass Lead glass Non-lead glass Dose rate (Gy · h -1) 1400 1200 1000 800 600 400 200 0 50 40 30 20 10 0 (a) (b)
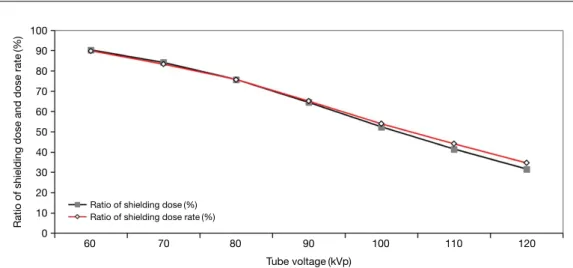
였고, 선량율은 89.9%가 차폐되었다. 관전압이 120kVp에 서 선량은 31.6% 차폐하였고, 선량율은 34.7%가 차폐되었 다. 관전압이 증가할수록 차폐율은 감소하였다. 관전압과 납 유리 사용 여부에 따른 차폐율을 나타낸 것이다. 관전압이 60kVp에서는 선량의 차폐율이 90.3%로 높게 나타났으나, 관전압이 120kVp로 증가함에 따라 차폐율이 31.6%로 감소하는 것을 볼 수 있다(Fig. 5).
고 찰
ICRP에서는 피폭선량 한도를 설정하고 ALARA(as low as reasonably achievable)의 방사선 방어의 세 가지 원칙으로 행위의 정당화(justification), 방어의 최적화(optimization), 개인 선량한도(limitation)로 방사선 방어를 최대한 합리적
으로 하여야 한다. 개인의 피폭 선량은 ICRP에서 권고하
는 개인 선량한도 내에서 작업이 이루어져야 한다. 따라서 결정적 영향(deterministic effect)과 확률적 영향(stochastic effect)이 있기 때문에 이 두 가지 경우에서 보면 threshold 값의 유무만 차이 날 뿐 결국 방사선에 노출이 될 경우 어 떤 형태로든 인체에 영향을 주기 때문에 방사선에 노출이 되지 않아야 하므로 차폐를 반드시 해야 한다. 이러한 차폐 및 선량감소를 위해 엑스선을 이용한 CT 검사에서는 선량 변동 프로그램을 개발하고 적용하여 임상에서 사용하고 있 고(Kweon et al. 2009) 또한 차폐기구를 검사에 이용하고 있 다(Park et al. 2017). 의료기관에서는 방사선을 이용한 검사에서 차폐를 위해 차폐율이 높고, 투명도(84.4%)를 최대한 유지하며 빛의 투 과율과 함께 차폐가 우수한 납유리가 많이 사용되고 있다. 이러한 투명도는 환자의 상태 및 시술자의 환자 관찰에 용 이한 환경을 제공한다. 납유리의 차폐재의 연당량은 0.8, 1.0, 1.5, 2.5mmPb의 종 류가 다양하게 있다. 현재 실험에 사용한 납유리의 연당량 은 1.5mmPb 제품을 사용하였다. 납유리는 엑스선관으로부 터 원천적 방어를 효과적으로 억제할 수 있는 방어 제품으 로 사용되고 있으며, Janssens(Janssens et al. 1998)의 보고 에 의하면 60keV, 0.985RF 조건에서 3.37 선흡수계수에서 3.00p·mm-1의 차폐능력을 보여주었다. 차폐재를 석고 보 드, 강판, 판유리 및 콘크리트의 엑스선 투과 특성을 측정 하여 엑스선으로부터 차폐 재료로 사용하는 결과를 제시하 고 엑스선은 50~125kVp에서 측정하여 보고하였다(Rossi et al. 2004). 진단영역 넓은 선속 엑스선 에너지에 대한 차 폐물질의 투과 특성에서 납유리의 관전압에 따른 선질을 표 시하는 반가층이 0.06mm(50kVp), 0.12mm(70kVp), 0.27 (100kVp), 0.28mm(125kVp)을 보고하였다(Archer et al. 1994). 본 실험에서는 납유리의 차폐능력을 투과에 의한 차폐 율을 산출하였다. 납유리의 차폐능력의 산출결과에서 관전 압 60kVp에서는 선량의 차폐율이 90.3%에서 관전압 120 kVp 31.6%로 차폐율이 관전압이 증가할수록 차폐율이 감 소하였고, 선량율은 관전압 60kVp에서는 선량의 차폐율이 89.9%에서 관전압 120kVp 34.7%로 차폐율이 감소하였다. 관전압이 증가할수록 차폐하는 능력이 감소하여 납유리는 고관전압 검사에서는 차폐에 유의하여야 한다. ICRP에서의 권고안은 직업상 피폭은 연간 50mSv에서 5 년간 100mSv를 초과하지 않는 범위 내에서 연간 최대 20 mSv의 선량 한계를 하향 조정하기를 권고하고 있다(ICRP 1990). 따라서 본 논문의 결과가 피폭감소의 측면에서 유의 한 결과가 있는 것으로 나타났다. 앞으로 피폭감소를 위한 방안과 노력은 계속적으로 요구되며 본 실험의 결과가 방사 선 차폐를 위한 참고자료로 사용할 수 있다. 연구의 제한점으로는 첫째, 방사선 선원과 납유리 및 선
Fig. 5. Relative ratio of shielding dose and dose rate of Xrays through the lead glass and nonlead glass for geometry the range of tube volt age are 60~120kVp.
Ratio of shielding dose and dose rate
(%)
60 70 80 90 100 110 120 Ratio of shielding dose(%)
Ratio of shielding dose rate(%) 100 90 80 70 60 50 40 30 20 10 0 Tube voltage(kVp)
량계의 거리의 역제곱 법칙에 따른 선량 및 선량율을 추가 적으로 실험할 필요가 있다. 둘째, 다양한 방사선 선량계를 이용하여 선량 및 선량율을 산출하여 비교할 필요가 있다. 셋째, 엑스선의 선질을 나타내는 반가층을 측정하여 관전압 과 납유리의 차폐 유무에 따라 비교할 필요가 있다. 넷째, 관전압에 따른 선량 비교와 함께 다양한 관전류를 적용하여 추가적인 연구가 필요하다.
결 론
엑스선의 관전압 변화에 따른 납유리의 차폐능력을 측정 하여 선량의 차폐율은 31.6~90.3%이었고, 선량율의 차폐율 은 34.7~89.9%로 산출되었다. 엑스선의 조사에 따른 납유 리의 차폐효과를 확인할 수 있었으며, 이와 같은 결과를 참 고하고 납유리의 특성을 잘 이용하여 피폭감소를 위한 노력 을 해야 할 것이다.참 고 문 헌
Archer BR, Fewell TR, Conway BJ and Quinn PW. 1994. Atte nuation properties of diagnostic Xray shielding materials. Med. Phys. 21(9):14991507.
International Commission on Radiological Protection. 1990 recommendations of the International Commission on Ra diological Protection: adopted by the Commission in Nov ember 1990. 1st ed. Oxford: Pergamon, 1991.
Jang YI, Song JN and Kim YJ. 2011. Efficacy of a protective glass shield in reduction of radiation exposure dose during interventional radiology. J. Korean Soc. Radiol. 5(5):303 308.
Janssens K, Vincze L, Vekemans B, Adams F, Haller M and Knoechel A. 1998. Use of leadglass capillaries for micro focusing of highlyenergetic(0~60keV) synchrotron radi
ation. J. Anal. Atom. Spectrom. 13(5):339350.
Kweon DC. 2017. Buildup characteristics of radiophotolumi nescent glass dosimeters with exposure time of Xray. J. Biomed. Eng. Res. 38(5):256263.
Kweon DC, Dong KR, Jung JE and Ryu YH. 2009. Comparison radiation dose with upper and lower Limbs of automated injection of contrast media with a bolus tracking system in pulmonary embolism MDCT. J. Radiat. Indt. 3(4):323328. Lee MS, Chung HS, Yin SP, Ahn DH, Kim KR, Lee SH, Paek
SW, Jung HS and Cho YG. 2003. A study on lead glass composition. Appl. Chem. 7(1):273276.
Park TS, Han JH, Jo SY, Lee EL, Jo KW and Kweon DC. 2017. Comparison of noise of doses of low dose and high resolution chest CT for automatic tube current modulation and fixed tube current technique using glass dosimetry. J. Radiat. Indt. 11(3):131137.
Rossi RP, Ritenour R and Christodoulou E. 2004. Broad beam transmission properties of some shielding materials for use in diagnostic radiology. Health Phys. 61(5):601608. Selmaier M, Stillkrieg W, Müller RG, Hahn EG and Ell C.
1994. Radiation burden in diagnostic and therapeutic endo scopic retrograde cholangiopancreatography. Z. Gastroen-terol. 32(12):671674.
Strzelczyk JJ, Damilakis J, Marx MV and Macura KJ. 2006. Facts and controversies about radiation exposure, part 1: controlling unnecessary radiation exposures. J. Am. Coll. Radiol. 3(12):924931.
Tuner JE. 1995. Atom, Radiation, and Radiation Protection, John Wiley & Sons, New York.
UNSEAR. 1988. Sources, Effects and Risks of Ionization Radiations, United Nations Scientific Committee on the Effects of Atomic Radiation, 1988 Report to the General Assembly, UN, New York.
Received: 29 January 2018 Revised: 27 February 2018 Revision accepted: 14 March 2018