Usefulness of serum C-reactive protein (CRP) level
for predicting flap complication
after performing free microvascular
head and neck reconstruction
by
Hyunsuk Song
Major in Medicine
Department of Medical Sciences
The Graduate School, Ajou University
Usefulness of serum C-reactive protein (CRP) level
for predicting flap complication
after performing free microvascular
head and neck reconstruction
by
Hyunsuk Song
A Dissertation Submitted to The Graduate School of
Ajou University in Partial Fulfillment of the Requirements for
the Degree of
Ph.D. in Medicine
Supervised by
Myong Chul Park, M.D., Ph.D.
Major in Medicine
Department of Medical Sciences
The Graduate School, Ajou University
This certifies that the dissertation
of Hyunsuk Song is approved.
SUPERVISORY COMMITTEE
Myong Chul Park
Yong Bae Kim
Kyung Suck Koh
Dong Ha Park
Il Jae Lee
The Graduate School, Ajou University
December, 19th, 2014
i
- ABSTRACT -
Usefulness of Serum C-reactive protein (CRP) Level for
Predicting Flap Complication after Performing Free
Microvascular Head and Neck Reconstruction
Free microvascular head and neck reconstruction requires minimal complication and safety. However, clinical observation of the wound in head and neck area is very difficult because of its narrow and inaccessible anatomy. Serum C-reactive protein (CRP) level is commonly used as a marker of acute inflammatory response and quantitative test that shows predictable kinetics. Therefore, awareness of natural CRP trend of free microvascular head and neck reconstruction may help in the early diagnosis of postoperative complications. The goal of this study is to describe the time course of serum CRP level and prove the usefulness of CRP as a predictor of postoperative flap wound complication after performing free microvascular reconstruction in head and neck area. Between June 2009 and November 2012, we retrospectively analyzed the data of 25 patients who received free microvascular tissue transfer for head and neck reconstruction at Ajou University Hospital. The characteristics of patients and surgical information were analyzed. From the first day after surgery, serum CRP levels were daily measured for two weeks. The average CRP values were daily calculated for the normal group and the complicated group and compared between each groups. The amount of time taken to reach the peak CRP level and to reach half of the peak was compared. A Total of 25 patients were included in this study. The amount of time taken to
reach the peak of the CRP level is significantly less in the normal group (2.88 days) than the complicated group (7 days) (p<0.001). Furthermore, the amount of time to reach half of the peak was significantly different between groups (7.19 days vs. 10.14 days, respectively, p<0.05). In the normal group (17/25), there were 14 cases which reached peak CRP level before postoperative day 4. However, in the complicated group (8/25), there was only 1 case which reached peak CRP level before postoperative day 4 (p< 0.05). The complication rate is 32.7 times higher when CRP value reaches peak on or after postoperative day 4 (95% Confidence interval, 30.26 - 35.14; p= 0.002). Patients in the complicated group showed significantly elevated CRP levels compared to those in the normal group at day 6 to 8 and day 12 (p< 0.05). In head and neck reconstructions, the high probability of flap wound complications are indicated through the result of having highest CRP values on or after postoperative day 4, slow normalization of serum CRP level and secondary rise in serial CRP values.
iii
TABLE OF CONTENTS
ABSTRACT ··· ⅰ, ⅱ TABLE OF CONTENTS ··· ⅲ LIST OF FIGURES ··· ⅳ LIST OF TABLES ··· v . Ⅰ INTRODUCTION ··· 1 . Ⅱ MATERALS AND METHODS ··· 3. Ⅲ RESULTS ··· 4 . Ⅳ CASE REVIEWS ··· 10 . Ⅴ DISCUSSION ··· 17 VI. CONCLUSION ··· 21 REFERENCES ··· 22 국문요약 ··· 25
List of Figures
Fig. 1. The number of patients reaching highest serum CRP value at each day and
statistical comparison ··· 8
Fig. 2. Postoperative serum CRP trends between normal and complicated group ··· 9
Fig. 3. Preoperative, intraoperative and postoperative views of case # 1 patient ··· 11
Fig. 4. Postoperative serum CRP trend in case #1 patient ··· 12
Fig. 5. The wound photograph of the patient in postoperative day 16 ··· 13
Fig. 6. Preoperative, intraopeartive and postoperative views of case # 2 patient ··· 14
Fig. 7. Postoperative serum CRP trend in case #2 patient ··· 15
v
List of Tables
Table 1. Patient’s characteristics, etiology, and location of surgery ··· 5
Table 2. Types of free flap ··· 6
Table 3. Postoperative complication ··· 6
Table 4. The average amount of time taken to reach peak and half of the peak
CRP level ··· 7
I. INTRODUCTION
Free microvascular tissue transfer is the last surgical option to save a limb and has become the choice of method for head and neck reconstruction. Therefore, having minimal complication and promoting safety is highly important. If there are any complications such as wound infection, wound breakdown, and partial necrosis, early recognition and treatment significantly results in better outcome. After performing microvascular reconstruction in the head and neck area, close clinical observation of the flap wound is very difficult because of its narrow anatomic space, postoperative intraoral tissue swelling and the patient’s poor cooperation. However, it is widely known that oral wounds have delayed healing because of an oral flora (Nooh and Graves, 2003). Therefore clinical or laboratory observation of the oral wound is more important than other surgical wound area. Serum C-reactive protein (CRP) level is synthesized by the liver and commonly used as a marker for acute inflammatory response. CRP is produced in response to inflammation, tissue destruction, infection and malignancy, and it has been reported that CRP level increases even before clinical infection or when systemic inflammatory response syndrome (SIRS) is apparent.(Boeken et al., 1998) Persistent increase of CRP level after its peak during postoperative course is known to be a warning signal.(Toman et al., 2008) The trends of the CRP level vary greatly among different operations and CRP is a quantitative test that exhibits predictable kinetics consisting of postoperative rise and a peak followed by a decrease toward its normal value.(Foglar and Lindsey, 1998) Therefore, the awareness of natural CRP trend of free microvascular head and neck reconstruction may help in the early diagnosis of
2
-postoperative flap complications. Herein, we discuss about the time course of serum CRP level after performing free microvascular reconstruction in the head and neck area. Furthermore, we sought to prove the usefulness of CRP as a predictor of postoperative flap complication, by comparing the kinetics of CRP between the normal group and the complicated group.
II. MATERALS AND METHODS
Between June 2009 and November 2012, we retrospectively analyzed the data of the
patients who received free microvascular tissue transfer for head and neck reconstructions at Ajou University Hospital. CRP is produced by various systemic conditions, such as inflammation, infection, trauma and malignancy, therefore to exclude systemic effect to serum CRP levels, patients who had systemic complications such as pulmonary embolism and pneumonia after the operation were excluded from this study. Also patients with deep vein thrombosis, liver disease or donor site complication who needs further surgery were excluded. A total of 25 patients were included in this study. All of these patients had no fever and other signs of infection at the day of the operation. The information about the patient’s age, medical co-morbidities, diagnosis, area of reconstruction and the type of free flap surgery was collected. Furthermore, flap complications such as flap loss (partial or total), wound breakdown, wound infection and further treatment were investigated. We divided the patients into normal group and complicated group. CRP levels were measured daily from the first day until 2 weeks after the surgery. Average CRP values were calculated daily for each group and compared between each groups. Furthermore, we evaluated the amount of time taken to reach the peak and half of the peak of the CRP level. Absolute CRP values were expressed as mg/dl. The unpaired t-test, Wilcoxon rank-sum test, and Fisher’s exact test were used for comparing the normal group and the complicated group, and p < 0.05 was considered significant.
4
-III. RESULTS
A Total of 25 patients met our inclusion criteria and the average age of the patients was 57 years (from 30 to 76). Patient characteristics, etiology and region of the surgery, and flap types used for reconstruction are shown in Table 1 and Table 2. Squamous cell carcinoma of the oral cavity represented 64% of all cases and anterolateral thigh fasciocutaneous free flap was performed most commonly (76%). There was no major flap wound complication, such as total flap necrosis, wrong positioning of the flap and hemorrhage which would need reoperation.
Table 1. Patient’s characteristics, etiology and location of surgery Age 57 years (30 -76) Gender Male 19 Female 6 Etiology
Squamous cell carcinoma 16(64%)
Tongue 4 Tonsil 3 Tongue base 2 Retromolar area 2 Mouth floor 1 Lower lip 1 Buccal area 1 Hypopharynx 1 Auricular area 1
Soft tissue defect and necrosis 4(16%) Temporal and occipital area 2 Lateral neck (mandible border) 1
Sternal area 1
Adenoid cystic carcinoma on sublingual gland 1(4%) Rhabdomyosarcoma on clavicular area 1(4%) Malignant melanoma on temporal area 1(4%) Pleomorphic adenoma in hard palate 1(4%) Meningioma on scalp 1(4%)
The age represents mean age. The number in gender and etiology category means the patient’s number.
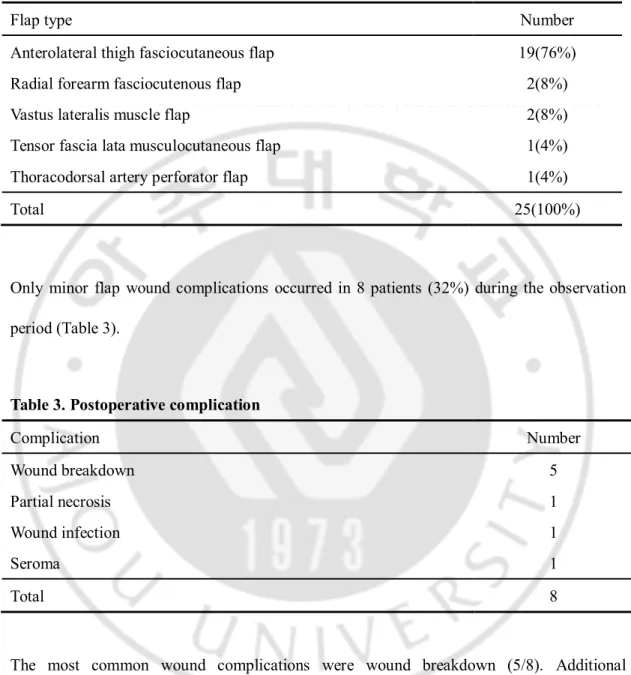
6 -Table 2. Types of free flap
Flap type Number
Anterolateral thigh fasciocutaneous flap 19(76%) Radial forearm fasciocutenous flap 2(8%) Vastus lateralis muscle flap 2(8%) Tensor fascia lata musculocutaneous flap 1(4%) Thoracodorsal artery perforator flap 1(4%)
Total 25(100%)
Only minor flap wound complications occurred in 8 patients (32%) during the observation period (Table 3).
Table 3. Postoperative complication
Complication Number Wound breakdown 5 Partial necrosis 1 Wound infection 1 Seroma 1 Total 8
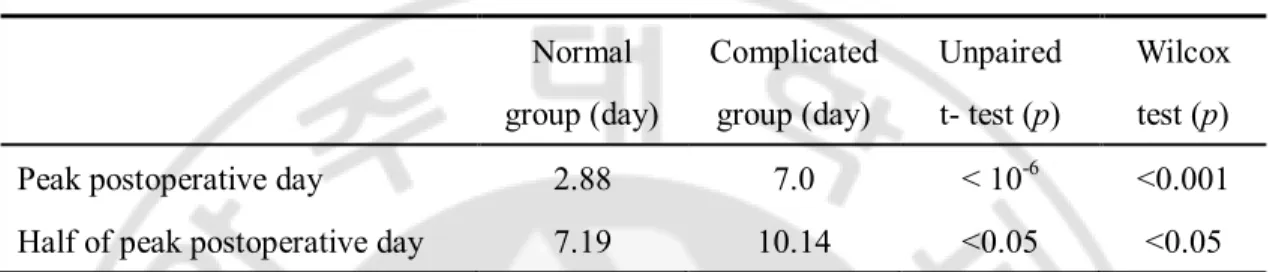
The most common wound complications were wound breakdown (5/8). Additional debridement and repair were done on all cases of wound breakdown (5/8), wound infection (1/8), partial necrosis (1/8) and seroma (1/8) after 2 weeks since surgery. The average amount of time taken to reach the peak CRP level was significantly less in the normal group (2.88 days) than the complicated group (7 days) (p<0.001). Furthermore, the amount of time
to reach half of the peak was significantly different between groups (7.19 days vs. 10.14 days, respectively, p<0.05) (Table 4).
Table 4. The average amount of time taken to reach peak and half of the peak CRP level Normal group (day) Complicated group (day) Unpaired t- test (p) Wilcox test (p) Peak postoperative day 2.88 7.0 < 10-6 <0.001 Half of peak postoperative day 7.19 10.14 <0.05 <0.05 In normal group the average amount of time taken to reach the peak and half of the peak CRP level was significantly less than the complicated group(2.88 days vs 7 days, 7.2 days vs. 10.1 days, respectively, p<0.05) (Table 4).
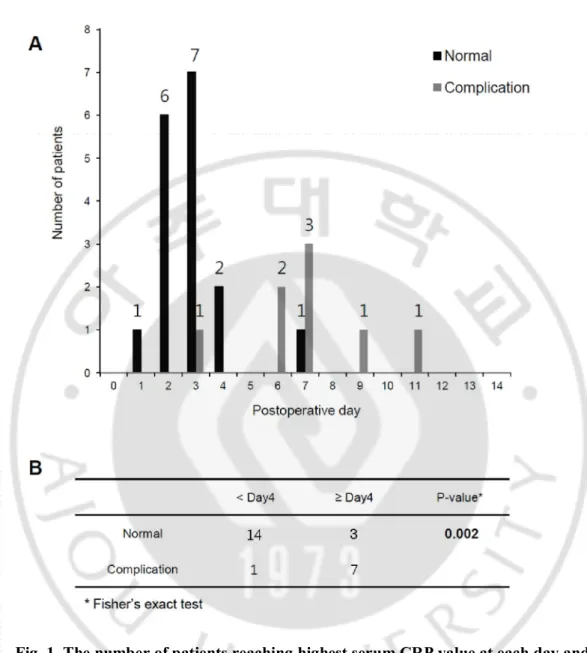
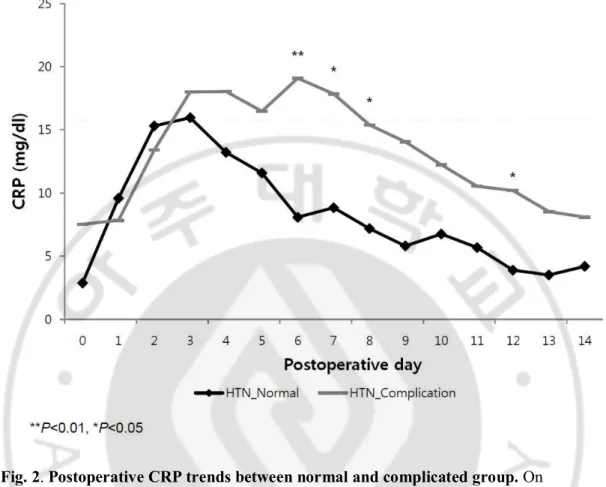
In the normal group, there were 14 cases (82%) which reached peak CRP before postoperative day 4. However in the complicated group, there was only 1 case (13%) which reached peak CRP before postoperative day 4 and this was statistically significant (p< 0.05) (Fig. 1). The rate of complication is 32.7 times higher when CRP value reaches peak on or after postoperative day 4 than peaks before postoperative day 4 (odds ratio = 32.7; 95% confidence interval = 30.26 to 35.14) (p= 0.002). In the comparison of CRP trends, patients in the complicated group showed significantly elevated CRP levels compared to those in the normal group at day 6 to 8 and day 12 (p< 0.05) (Fig. 2).
8
-Fig. 1. The number of patients reaching highest serum CRP value at each day and statistical comparison. The number of patients reaching highest serum CRP value at each
day is shown (A) and the number of the patient was categorized by whether the peaking date is on or after postoperative day 4 in each groups (B). Odds ratio of the flap complication in patients who have a peaking date on or after postoperative day 4 was 32.7( 95% confidence interval = 30.26 to 35.14) (p= 0.002).
Fig. 2. Postoperative CRP trends between normal and complicated group. On
postoperative day 6, 7, 8 the complicated group shows significantly elevated CRP levels compared to normal group (p< 0.05).
- 10 -
IV. CASE REVIEWS
1. Case # 1
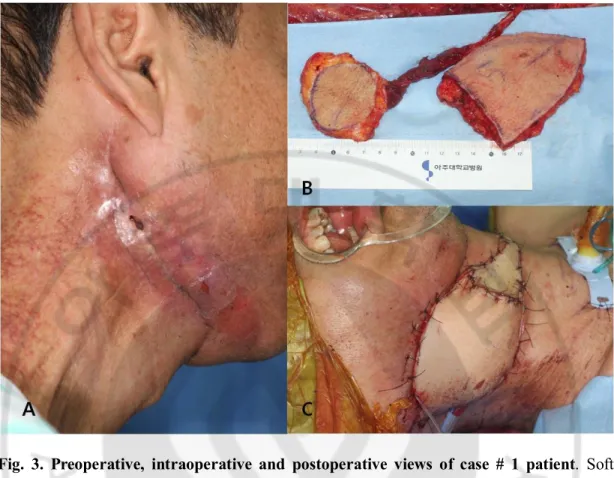
The patient was a 56-year-old man with soft tissue defect on right lateral neck and mandibular area (Fig. 3A). He had undergone a concurrent chemoradiotherapy for nasopharyngeal squamous cell carcinoma 10 years ago, selective neck dissection 2 years ago and segmental mandibulectomy of the necrotic bone with plate fixation 2 months ago. After the segmental mandibulectomy, the neck flap necrosis progressed and finally the bone and titanium plate were exposed. The debridement of the necrotic skin and bone was done and to cover the open wound, total 13 x 8cm2 sized chimeric type anterolateral thigh
fasciocutaneous flap was elevated (Fig. 3B). The vessel anastomosis was done with contralateral superior thyroidal artery and vein by end to end method. Initially the flap and recipient skin wound was stable, however the serum CRP level didn’t drop as expected (Fig. 3C).
Fig. 3. Preoperative, intraoperative and postoperative views of case # 1 patient. Soft
tissue necrosis and bony exposure was observed in Rt. mandibular border (A). Chimeric type anterolateral thigh flap was elevated (B) and in postoperative view the flap was pinkish and wound was clear (C).
The peak CRP level was measured on postoperative day 6 (12.83 mg/dl) and progressive wound dehiscence was observed on upper border of the flap and partial necrosis was noted on the full thickness skin graft area which was used to cover the flap pedicle after postoperative day 7 (Fig. 4) .
- 12 -
Fig. 4. Postoperative serum CRP trend in case #1 patient. The CRP level newly peaked
on postoperative day 6 (12.83 mg/dl).
Finally additional debridement and repair were done on the wound breakdown area and split thickness skin graft on the pedicle area on postoperative day 16 (Fig. 5).
Fig. 5. The wound photograph of the patient in postoperative day 16. 4 x 2cm2 sized
wound breakdown was observed on upper border of the flap.
2. Case # 2
A 30-year-old woman was referred to our clinic by neurosurgery department for the exposed occipital cranium. The patient had been beaten in the head with a blunt object by her father and had undergone the operation for the skull fracture and epidural hematoma 1 month ago. However there was a progressive scalp wound necrosis and eventually skull was exposed on left occipitoparietal area (Fig. 6A). The debridement of the wound was done and final defect size of the exposed bone area was 9 x 7cm2. In the operation 11 x 8
cm2sized thoracodorsal artery perforator flap was elevated to cover the bony exposed area
and split thickness skin graft was performed on the other area (Fig. 6B). One arteriorrhaphy and two venorrhaphy were done with superficial temporal artery and venae commitantes,
- 14 -
respectively. After the operation the flap was stable and wound was clear (Fig. 6C).
Fig. 6. Preoperative, intraopeartive and postoperative views of case # 2 patient. Multiple
posterior scalp necrosis was observed and the cranium was exposed on Lt. occipital area (A). 11 x 8 cm2 sized thoracodorsal artery perforator flap was elevated (B) and the flap
wound was stable postoperatively (C).
The CRP level peaked on postoperative day 3 (14.37mg/dl) and decreased progressively as days went by. However on postoperative day 7, the CRP level reached to the highest level (22.21mg/dl) and wound dehiscence was noted on lower border of flap wound (Fig. 7 and Fig. 8). The wound dressing was done daily and debridement and repair were done on
postoperative day 15.
Fig. 7. Postoperative serum CRP trend in case #2 patient. Postoperative CRP trend of
the patient shows bimodal pattern and secondary peak (22.21mg/dl) is observed on postoperative day 7.
- 16 -
Fig. 8. The wound photograph of the patient on postoperative day 13. Wound
V. DISCUSSION
Immediate microvascular free flap reconstruction after the ablation of head and neck carcinoma is associated with improving the patient’s quality of life and increasing his or her survival rate.(Mucke et al., 2010) However major postoperative flap complications that prolong intensive care and hospitalization are associated with decreased survival rate.(Ch'ng et al., 2014) Therefore reducing complication and securing safety are highly important and if there is any complication, early recognition and proper treatment are critical to shorten hospitalization and increase survival rate. In one study of microsurgical head and reconstruction, major and minor flap complications rate were 11.9% and 19.1% in a total of 376 free flap transfers and in another study, a total of 19 patients (31.7%) experienced flap related complications.(Bianchi et al., 2009; Momeni et al., 2011) This result is comparable with our results (32% of total flap complication). However in our study, there was no major complication that would need urgent reoperation such as total flap necrosis, hemorrhage and wrong positioning of the flap. A wide variety of modes of monitoring, both invasive and non-invasive, exists for microsurgical head and neck reconstruction. The clinical assessment is the simplest and most reliable method, however it cannot be used for buried flap and it is very difficult to assess color, capillary refill and warmth due to the narrow anatomical space in intraoral reconstruction. Other non-invasive monitoring methods include surface temperature and Doppler monitoring, microlight guide spectrophometry, color Doppler sonography, and laser Doppler flowmeter.(Abdel-Galil and Mitchell, 2009b) Invasive modes of monitoring include implantable Doppler monitoring, the Cook venous monitoring system,
- 18 -
contrast- enhanced Doppler monitoring, invasive temperature monitoring, oxygen tension monitoring, tissue PH monitoring and microdialysis.(Abdel-Galil and Mitchell, 2009a) However, current methods of flap monitoring are neither ideal nor objective for all types of free flap, and those methods are only used for detecting acute vascular compromise.(Abdel-Galil and Mitchell, 2009b) Flap wound complication such as wound dehiscence and infection can occur after vascular stabilization of free flap. To find the subacute and late flap wound complication, other supplementary monitoring techniques or laboratory tests are needed besides clinical assessment. Erythrocyte sedimentation rate (ESR), which is widely used as an indicator of infection, has a reasonably high sensitivity and specificity to inflammation and malignancy.(Dinant et al., 1991) However the ESR is an indirect test of the albumin-globulin ratio and fibrinogen in plasma, and has been shown to be changed by age, nutrition, fluid status and time of day.(Foglar and Lindsey, 1998) Also the ESR increases rather arbitrarily and decreases so slowly that active inflammation and infection is likely to have resolved earlier than the time to reach ESR normalization.(Dich et al., 1975; Tetzlaff et al., 1978) Therefore early detection of complication in head and neck reconstruction using ESR value is limited. The CRP, in contrast to the ESR, is directly measured and the effect of the drug and diseases except for hepatic failure is minimal.(Pepys and Hirschfield, 2003) The plasma CRP was first isolated from the patient’s blood with a pneumococcal pneumonia infection and then CRP estimation became clinical practice as an early indicator of infection. (Tillett and Francis, 1930; Kallio et al., 1990) The CRP is produced by the liver in response to infection, inflammation, malignancy and trauma with relatively high response speed, and narrow normal range compared to other acute phase
reactants.(Mok et al., 2008) The plasma CRP increases even before clinical infection is apparent and an elevated CRP value is highly suggestive of acute infection or trauma.(Boeken et al., 1998; Gabay and Kushner, 1999) The plasma CRP value is known to reach its peak value after about 48 hours and drop sharply if the cause is treated.(Toman et al., 2008) Because the plasma CRP value is determined mainly by its production rather than clearance, elevated CRP level reflects presence and extent of current process. However, the kinetics of CRP in various operations is different.(Mok et al., 2008) The studies about normal kinetics of CRP in spinal, knee and cardiac surgery, describe a peak CRP value on postoperative day 2 or 3, followed by initial sharp decline and a gradual decrease with normalization in postoperative day 14 to 21.(Mok et al., 2008) In mammoplasty and abdominoplasty, the CRP peak values appeared throughout postoperative days 3 to 5 and no sharp decline of CRP after postoperative day 5 was a warning sign.(Toman et al., 2008) In the reconstruction of lower limb with local and free flap, CRP peaks were found on day 2 and peaks after postoperative day 4 indicated the complications.(Wright and Khan, 2010) However there is no study about the kinetics of CRP in microsurgical head and neck reconstruction. In our study, the peak CRP value appeared mainly at postoperative day 2 and 3 in the normal group and average amount of time taken to reach the peak of the CRP level is 2.9 days. This finding is comparable with other studies. In the complicated group, only 1 case (13%) reached the peak CRP value before postoperative day 4. Therefore if the peak CRP value sustains on or after postoperative day 4, it suggests the high probability of the flap wound complication (odds ratio = 32.7; 95% CI = 30.26 to 35.14) (p= 0.002). And it suggests that the effort to find the cause of elevated CRP is needed. The most postoperative
- 20 -
flap complications were wound breakdown and it is known that raw surface in oral wound has significant number of polymorphonuclear leukocytes and higher degree of inflammation because of an oral flora.(Nooh and Graves, 2003) Therefore we can assume that the elevated CRP level didn’t drop due to continuous inflammation. And the amount of time needed to reach half of the peak CRP shows clear distinction between normal and complicated groups (7.2 days vs. 10.1 days, respectively, p<0.05). It reflects the slower elevation and normalization of the plasma CRP level in the complicated group than the normal group. In the comparison of the CRP trends, in contrast to unimodal distribution of CRP level in the normal group, complicated group shows bimodal distribution of plasma CRP level and statistically postoperative day 6,7,8 and 12 shows difference (p< 0.05). It shows second rise of the CRP level indicates high probability of flap complication. Using serum CRP level, at least 4 days are needed to distinguish normal and complicated CRP response, it cannot be used as an acute vascular monitoring method. It only can be used as a supplement to the clinical examination for the flap wound. A limitation of our study includes the small number of patients who met inclusion criteria. Therefore we couldn’t subdivide the patients according to their medical co-morbidities which can alter serum CRP level. The correlation of serum CRP level to wound complication and medical co-morbidities would be important and it could be the aim of further studies. And also comparing CRP trend among flap types and surgical sites would be necessary to investigate more specified postoperative CRP kinetics.
VI. CONCLUSION
Knowledge of the natural CRP response in free microvascular tissue reconstruction helps in the assessment of postoperative flap complications. And the measurement of plasma CRP level is useful supplement to the clinical examination of the flap wound. In head and neck reconstruction, the highest CRP values on or after postoperative day 4, slow normalization of plasma CRP level and secondary rise in serial CRP values indicate high probability of flap wound complications.
- 22 -
REFERENCES
1. Abdel-Galil K, Mitchell D: Postoperative monitoring of microsurgical free-tissue transfers for head and neck reconstruction: a systematic review of current
techniques--part II. Invasive techniques. Br J Oral Maxillofac Surg 47: 438-442, 2009a
2. Abdel-Galil K, Mitchell D: Postoperative monitoring of microsurgical free tissue transfers for head and neck reconstruction: a systematic review of current
techniques--part I. Non-invasive techniques. Br J Oral Maxillofac Surg 47: 351-355, 2009b
3. Bianchi B, Copelli C, Ferrari S, Ferri A, Sesenna E: Free flaps: outcomes and complications in head and neck reconstructions. J Craniomaxillofac Surg 37: 438-442, 2009
4. Boeken U, Feindt P, Zimmermann N, Kalweit G, Petzold T, Gams E: Increased preoperative C-reactive protein (CRP)-values without signs of an infection and complicated course after cardiopulmonary bypass (CPB)-operations. Eur J
Cardiothorac Surg 13: 541-545, 1998
5. Ch'ng S, Choi V, Elliott M, Clark JR: Relationship between postoperative
complications and survival after free flap reconstruction for oral cavity squamous cell carcinoma. Head Neck 36: 55-59, 2014
6. Dich VQ, Nelson JD, Haltalin KC: Osteomyelitis in infants and children. A review of 163 cases. Am J Dis Child 129: 1273-1278, 1975
7. Dinant GJ, Knottnerus A, Van Wersch J: Leucocyte count as an alternative to ESR in general practice? Scand J Prim Health Care 9: 281-284, 1991
8. Foglar C, Lindsey RW: C-reactive protein in orthopedics. Orthopedics 21: 687-691; quiz 692-683, 1998
9. Gabay C, Kushner I: Acute-phase proteins and other systemic responses to inflammation. N Engl J Med 340: 448-454, 1999
10. Kallio P, Michelsson JE, Lalla M, Holm T: C-reactive protein in tibial fractures. Natural response to the injury and operative treatment. J Bone Joint Surg Br 72: 615-617, 1990
11. Mok JM, Pekmezci M, Piper SL, Boyd E, Berven SH, Burch S, Deviren V, Tay B, Hu SS: Use of C-reactive protein after spinal surgery: comparison with erythrocyte sedimentation rate as predictor of early postoperative infectious complications. Spine
(Phila Pa 1976) 33: 415-421, 2008
12. Momeni A, Kim RY, Kattan A, Tennefoss J, Lee TH, Lee GK: The effect of preoperative radiotherapy on complication rate after microsurgical head and neck reconstruction. J Plast Reconstr Aesthet Surg 64: 1454-1459, 2011
13. Mucke T, Wolff KD, Wagenpfeil S, Mitchell DA, Holzle F: Immediate
microsurgical reconstruction after tumor ablation predicts survival among patients with head and neck carcinoma. Ann Surg Oncol 17: 287-295, 2010
14. Nooh N, Graves DT: Healing is delayed in oral compared to dermal excisional wounds. J Periodontol 74: 242-246, 2003
15. Pepys MB, Hirschfield GM: C-reactive protein: a critical update. J Clin Invest 111: 1805-1812, 2003
16. Tetzlaff TR, McCracken GH, Jr., Nelson JD: Oral antibiotic therapy for skeletal infections of children. II. Therapy of osteomyelitis and suppurative arthritis. J
Pediatr 92: 485-490, 1978
17. Tillett WS, Francis T: Serological Reactions in Pneumonia with a Non-Protein Somatic Fraction of Pneumococcus. J Exp Med 52: 561-571, 1930
- 24 -
18. Toman N, Buschmann A, Muehlberger T: Specific C-reactive protein measurements in plastic surgery. Scand J Plast Reconstr Surg Hand Surg 42: 138-144, 2008 19. Wright EH, Khan U: Serum complement-reactive protein (CRP) trends following
local and free-tissue reconstructions for traumatic injuries or chronic wounds of the lower limb. J Plast Reconstr Aesthet Surg 63: 1519-1522, 2010
- 국문요약 -
미세수술을
이용한 두경부 결손부 재건에 있어서 피판 합병증
발견을
위한 혈청 C-reactive protein(CRP) 측정의 유용성
아주대학교 대학원의학과 송 현 석 (지도교수: 박 명 철) 두경부 결손 재건에 있어서 미세수술을 통한 유리 피판술은 널리 사용되는 수술법으로서 안정성과 최소한의 합병증이 중요하다. 수술 후 중대한 합병증이 생길 경우 환자의 생존기간이 짧아진다는 보고가 있으며 만약 피판의 합병증이 발생할 경우 조기에 발견하고 적절한 치료를 하는 것이 중요하다. 수술 후 피판 모니터링 방법 중 임상적 관찰이 가장 간단하고 신뢰성이 있다고 알려져 있으나 두경부의 좁고 어두운 해부학적 특성으로 인하여 정확하고 세심한 판단에 어려움이 있다. 혈청 C-반응 단백질(CRP)은 급성 염증 반응에 대한 표지자로서 수치의 증감이 염증 정도에 따라서 빠르게 반응하며, 혈청 CRP 수치의 경향은 수술의 종류마다 다양한 동력학적 특성을 보인다. 이러한 혈청 CRP 값은 이미 척추, 무릎 그리고 심장 수술 후 감염 및 염증을 판단하는데 있어서 널리 사용되고 있다. 이번 연구는 두경부 미세 재건 이후 혈청 CRP 의 시간에 따른 변화를 측정하고 정상군과 합병증군 간의 차이를 알아봄으로써- 26 - 두경부 미세 재건 이후 혈청 CRP 의 측정이 유리 피판의 모니터링 방법으로서 유용하다는 것을 증명 하고자 하는 것이다. 2009 년 6 월부터 2012 년 11 월까지 유리 피판술로 두경부 재건술을 받은 환자 중 수술 후 혈청 CRP 값을 측정하였던 환자를 대상으로 하였으며, 수술 이외의 혈청 CRP 값의 변화를 배제하기 위하여 간질환 등의 기저 질환 및 수술 후 폐색전증, 폐렴 등의 전신적인 합병증을 가진 환자는 이번 연구에서 제외하였다. 연구 대상을 수술 후 합병증 유무에 따라서 정상군과 합병증 군으로 나누고 두 군간 통계적 비교를 하였다. 1. 두 군의 혈청 CRP 가 가장 높은 값(peak)을 이루는데 걸린 평균 시간 값은 정상군(2.88 일) 과 합병증군(7 일) 사이에 유의한 통계적 차이를 보였다 (p<0.001). 2. 두 군의 혈청 CRP peak 값의 절반이 되는데 걸리는 시간 역시 7.19 일과 10.14 일로서 정상군에서 통계적으로 유의하게 짧았다 (p<0.05). 3. 각 일별로 두 군의 혈청 CRP 값을 비교해본 결과 수술 후 6,7,8, 그리고 12 일에 합병증 군에서 혈청 CRP 값이 유의하게 높았으며 (p<0.05) 4. 수술 후 4 일째 및 그 이후에 혈청 CRP peak 값이 나타난 군이 수술 후 4 일 이전에 혈청 CRP peak 를 이룬 군보다 합병증의 확률이 32.7 배나 높은 것을 확인 할 수 있었다 (p<0.05). 이러한 결과를 보았을 때 두경부 미세 재건 수술 이후 혈청 CRP 값의 측정이 피판의 간접적 모니터링의 방법으로서 유용하게 사용될 수 있으며 미세재건 수술 후 3 일 이후에도 혈청 CRP 값이 높게 나타나는 경우, 혈청 CRP 값이 정상화 되는 속도가 느린 경우 그리고 혈청 CRP 그래프에서 두 번째 peak 가 보이는 경우 등에서는 피판 상처의 합병증 가능성이 높으므로 정밀한 검사 및 평가가 필요하다.