I TheJournal01Medicineand LifeSCience Vol. 7,No. 2,2010
The Obesity: Can it be the only factor of pulmonary aspiration
during the induction of general anesthesia?
- A
casereport-Hye .Jin Kim
,
Hye Young Shin,
Jong Cook Park,
and Sang Hyun Park Departrnent01Anesthesiologyand Pain Mediciney.Jeju NationalUniversilySCh∞
I 01Medicine,Jeμ KoreaAbstract
Ouring perioperativÐ period,pulmonary aspiralion is rare bul has significanl morbidily and mortality. Therefore. we Should keep in mind and Iry 10 prevent il
In this case that we rep
。
π even in Ihe patient fasting 12 hours,adequale fasling before elective surgery. the pa1ienl with n。
risk’
aclor except obesily (body mass index 34.9 kg/m2) underwenl pulmonary aspiralion. 1Isuggests lhat obesily can be the。미y independent faclor associa1ed wilh pulmonary aspiration. Thus,we sh。미d be aware of unexpecled as미ralion pneumonia and should be particularly cau1ion when performing induclion of anes1hesia in dealing with patients who are obese. (J Med U
’
e Sci 2010;7:48-51)Key Words : Airway managemenl,Aspira1ion pneumonia,Obesi1y
→→← ← →←←← →「
Introduction _j
Pulmonary aspiration is common in patients under general anesthesia. mosl frequenUy during induction. as compared to neuraxial 01' regional anesthesia1). During periopera
“
ve period. it is rare but it has significant morbidity and mortality. Associated factors for a잉:piration inc1udeafter-hours procedures ‘extremes of age‘gastrointestina! 01'
abdominal procedures. impaired consciousness. lithotomy position and obesity2)
Meanwhile. 0뾰sity appears to be a contributing factor in several studies for pulmonary aspiration of gasbic contenÍS Presumed increased intra-abdorninal pressure,hi영1 residual gastric volume,low pH,delayed gastric emptying and gastro-esophageal reflux disease increases the risk of aspiration pneumonitis in th.e obese pat.ient3).though recent sωdies have presented the da1a to disprove i씬-5)
We report a casc in which aspiration pneumonitis
。
ccurred during ma앙 fitting for intubation. although 1hispatient had no known risk factors for gastric content aspiration except obesiψ and had fasted for about 12 hOUI응‘
Address lor correspandence : Hye Jin Kim
Oepa이menl이Aneslhesiologyand Pain MedicineyJeju Nalional
UniversilySCh
。이。
f MecJicine,66 Jejudaehakno. 690-756‘Jeμ KoreaE-mail:[email protected]
Case Report ---
~~~'---j
A 22-year-old woman (height. 160 cm: weight. 89.4 kg body mass index,34.9 kg/m’)diagnosed with chronic tonsiJIitis was scheduled for a tonsillectomy under general anes1hesia. Her surgical history. medical history and phαsical examination were unremarkable. Her fasting time was fOl about 12 hours
On the day of surgery ,after appiication of routine mOIllωring. anesthesia was induced by lidocaine and propofol with rocuronium for neuromuscular blockade. Mask fi띠ng ventilation was performed for 60 seconds after injecting the rocuronium. When foam at the mouth was seen. her mouth was opened for suction π1en nearly c1ear f1uid was visible in her oral cavity. Her head was tumed to the side promptly and the oral cavity was suctioned sufficientiy. 11113trachea was intubated with a 7.5 mm oral RAE ωbe. Her oxygen saturation (SpÜ1) was 98%. QuickJy suction through the endotracheal tube was performed ln1Taoperative anesthesia was maintained with oxygen (2.0 Llmin),nitrous oxide (2.0 Llmin) and desOurane (6-7 vol%) During surgery. oxygen saturation was maint8ined between 98-99%
The surgery was completed within 1 hour. AnesLhetic management and recoverγ presented no complication π'e tracheal wbe
‘
I{as removed when she responded to verhal-η1e Obesity:Can it be the only factor of pu1monarγaspiration during the inductionof genera] anesthesia?
commands 밍ld showed sufficient spontaneous respiration
and neuromuscular function. She remained in post-anesthetic care unìt (PACU) for 25 minutes event free. Her vital signs were stable without any problems (Spα ) 99 %)
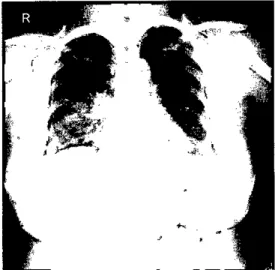
And she was then transferred to general ward. A postoperative posteroanterior chest X-ray was taken (Fig.l) Based on this imaging finding ,aspiration was highly suspected. 1n her room,she felt mild chillness. Fever set in a few hours later. She received ehanged empirical antibiotic treatment to fluoroqinolone. Pneumonia was under conσ
。
l and 야1e fever subsided gradu삶ly. After 3 days of medic밍treatment ,pneumonia was improved and she was discharged in a stable condition
Figure 1. The ehest X-ray showed patchy consolidation in the right middle lung zone due to aspiration
l----_---._.
DiscussionAspiration is defined as the inhalation of orophmγngeal or gastric contents into the larynx 밍ld 1
。、
iVer respiratory tractPulmonmγ aspiration was confinned in 1 in 8β00 anesthetic procedures in a recent revie
、
if;l and accormted for 4% of claims in the ASA Closed Claims Study7l. Risk factors for aspiration of gastric contents include pregnaney , acute gastrointestina1 disease (esophageal or gastric disease,small bowel obstrllction,and ileus),trauma,diabetes,and obes↓ty1naddition,recent ingestion of food is a risk factor. But fasting from the midnight before surgery to any time in the following day is thought to be excessive8l. Pulmonary aspiration can be classified into tw'O distinet clinical entities,
aspiration pneumonitis and aspiration pneumonia9). The differences between aspiration pneumonitis and aspiration pneumonia are summarized in Table 1. 1n this case,the aspirate was liquid,which is assoeiated with pneumonitis
Obesity is a medica1 condition in which excess body fat has accumulated to the extent that it may have an adverse effeet on health. Body mass index (BMI),defmed as the weight in 뻐。grams divided by the square of 며1e height in meters (kg/m~),is a simple index of body fat in adults. 1n 2006,according to WHü recommendatlon on the basis of the available data in Asia (Table 2),Korean Society for the Study of Obesity (KSSO) updated guideline for body weight classification in adults. Within this framework,Korean adults are considered overweight of their body mass index (B:MI, kg/rriι) is 23 or greater,and obese if their B:MI is 25 or greater. Obesity is further separated into 2 classes
Table 1. Comparison of Features of Aspiration Pneumonitis and Aspiration Pneumonia10l
Aspírationpneumonilis Aspírationpneumonia
Mechanism
Palhophysiologicprosess
Bacleriologicfíndings Mainpredispos↑ng faclors
Age group affecled Aspírationevenl
Typícalpresenlalíon
Clinìc헤fea1ures
Aspîrationof sterile gastric contents
Acute lung injury arising from acidic and particulate gastric mate끼al
Initially sterile,with subsequent bacterial infection possible
Markedly depressed level of consciousness All age groups,but usually young persons May be witnessed
Patient with a historγ
。
f a depressed level of consciousness in whom a pulmonary infiltrate and respiratory symptoms developNo symptoms or symptoms ranging from a nonproductive cough to tachypnea ,
bronchospasm,bloody or fJ때lY sp따um,and
res.[:σaloη clistress 2-5 hours와ter aspiration
49
Aspiration of colomzedorophaγngeal mate끼al
Acute pulmonarγ inflammatorγ response to bacteria and bacterial products
G,잉n-positive cocα,G,잉n-negative rods,and (rarely) anaerobic bacteria
Dysphagîaand gastric여잉notilîty Usually elderly persons
u잉lally not witnessed
lnstitutîon<õ니i7.edpatient with dysphagîa in whom clinical features of pne띠nonia and an infiltrate in a dependent
bronchopulmonarysegment develop
Hye Jin Kim.Hye YoungShin. Jong Cook Park,and Sang Hyun Park
Table 2. Proposed Classification of Weight by BMI in Adult Asianslll
Table 3. Methods to Reduce Risk of Regurgitation and P니1monarγ Aspiration13l
Class↑!ιatlon BMIIK91π') Risk of co-morbidities
UnderweiÇjht
<
18.5 tιother clinicalproblems)。
N" (but increased risk of Norηal range 18.5 - 22.9 Average。
verweight :::::23.0A↑risk 23.0 - 24.9 Increased
Obese 1 25.0 - 29.9 Moderate
。
bese I1 2': 30 Severe1. Minímizeintake
2. Increase gastric emptying
3. Reduce gastric volume and acidity
Adequate preoperative fasting Clear liquídsonly íf necessary Prokinetics(e.g.,
metoclopramide)
Non-partic니1ate antacid (e.g
sodilun citrate)
Hcreceptor antagonists '(e.g.,
fεunoti이ne)
Proton pump inhîbitors(e.g.,
lansoprazole)
2006:20:363-378
i:-
Rgf&rences9) Marik PE. Aspiration pneumonitis and aspiration pneurnonia. N Engl J Med 2001:344(9):665-71
10) Lai PJ,Chen FC ,Ho ST,Chemg CH,Liu ST,Hsu CH Unexpected p매monary aspiration during endoscopy lli1der intravenous anesthesia. Acta Anaesthesiol Taiwan 1) Cheney FW: Aspiration: a liability hazard for the
anesthesio1ogist? ASA Newsletter June 2000;64:1-3 2) Kalinowski CP,Kirsch JR: Stratiges for prophylaxis and
treatment for aspiration. Best Pract Res Clin Anes야1es101 2004 Dec:18(4):719-737
3) Vaughan RW,Bauer S,Wise 1: Volume and pH of gastric juice in obese patients. Anesthesiology 1975;43:686-689 4) H앙1:er R1,Kelly WB,Kramer MG,Perez CE,Dzwonczyk
RR: A comparison of the volume and pH of gastric contents of obese and 1ean surgicai patients ,Anesth
Analg 1998:86:147-152
5) Zacchi P,Mearin F. Humbert P,Formiguera X, Malagelada JR: Effect of obesity on gastroesophageal resistance to f10w in man,Dig Dis Sci 1991;36(10):1473
80
6) Neelakanta G, Chikyarappa A: A review of patients with pulmonary aspiration of gastric contents during anesthesia reported to the Departmental Quality Assurance Committee. J Cbn Anesth 2006:18:102←107
7) Lee LA. Dornino IζB: 111e closed claims project. Has it influenced anesthetic practice and outcome? Anesthesiol Clin North Am 2002:20:485-501
8) Maltby JR: Fasbng from midnight ← the historγ behind
the dogma. Best Pract Res Clin Anaesthesio1 Cricoid pressure
Cuffed endotracheal intubation Esophagea1-tracheal combitubE Proseal larγngea1ma하ι a미way
4. Airwaymanagement와,d
protection according to the increased health risk associated with
increasing BMl levels class 1 (BMI 25 - 29.9) and class II (BM! ;> 30). ln 야lÌs case. the patient (BMl 34.9 kg/m2) is
class II that is previous stage of morbid obesityll-12) η1e cut-offs are lower than the WHO criteria,Despite adequate
fasting before elective surgerγ (ni] per os [NPO] after midnight),the patient with no risk factor except obesity (BM!,34.92 kg/m') underwent p띠monmγ aspiration
Since unexpected aspiration may occur in the patient without obvious risk factor for pu때onarγ aspiration except obesity. we should endeavor to prevent it from occumng and minirnize the damage it causes should it OCCUf.In obese patients. we suggest
“
1at rapid sequence induction (RSI)13l and the technique of cricoid pressure should be routinely considered during induction2l. The patient lie supine with a slight head-down tilt to assist gravitational drainage of gastric contents away from the airway shou1d regurgitation occur,Once intubation has done ,45 head-e1evated position is better to preven( aspiration:잉Meanw비le,reducing gastric acidity may he1p avoid severe lIlJUIγ resulting from massive aspiration and can be achìeved by administrating proton pwnp inhibitors or histamine H2
receptor antagonists on the day of surgery. These medications can effectively increase the gastric pH and decrease the volume of gastric juice. lt is generally considered that a pH of 1ess than 2.5 and a volwne of gastric aspirates greater than 0.3 mL/Kg body weight (20 25m1 in adults) may lead to aspiration pneumonitis1이 까1e methods for preventing aspiration pneumonitis are knownltable 3)
In conclusion,this case reminds us that,even in the patient fasting 12 hours ,obesity can be the only independent factor associated with pulmonarγ aspiration Therefore ,we shou1d be aware of unexpected aspiration pneumonia and shou1d be particularly caution when penorming induction of anesthesia
-πle Obesity:Can it be the only factor of pulmonary aspiration during the înductionof general anesthesia?
2010:48(2):94-8
11) Steering Committee of the \iVl-IOWestem Pacific Region‘
lASO & IOTF. The Asian-Pacific Perspective: Redefining Obesity and Its 암'eatment. Australia,2000
12) WHO expert cons니lta미on: Appropriate body-mass index for Asian populations and its împlications for policy and
intervention strategies. Lancet 2004;363:157-63
13) TH Kang,KM Lee‘SE Lee,YW Kim,SH Lim,따i Lee,et al.: Aspiration pneumonitis after a lQ-hours fast in a patient who had undergone subtotal gastrecwmy. Korean J Anestheslol 2008:55:376-9