112
서 론
1991년 Parodi 등이 복부대동맥류(abdominal aortic aneurysm, AAA)의 치료로써 endovascular aneurysm repair (EVAR)를 처 음 발표한 이후로 혈관중재 기술의 발달과 더불어 EVAR은 꾸준히 연구되어 외국에서는 괄목할 만한 결과들이 보고되 고 있다.(1) 최근 결과로 보면 EVAR는 시술 후 30일 이내의 사망률과 시술 후 합병증이 개복 대동맥류 수술보다 적은 장점으로 수술의 고위험군 환자에게 유용하지만, 시술의 적응증에 제한이 있고, 시술과 관련된 또는 시술 후 관찰되 는 합병증 등(endoleak, 이동(migration), 기구의 파열(broken stent), 개복 대동맥류 수술로의 전환, AAA 크기 증가, AAA 파열, stent-graft 폐색)과 시술 후 경과관찰이 반드시 필요한 단점이 있다.(2-4) 국내에는 이에 대한 경험과 보고가 극히 적어 저자들이 경험한 자료를 분석하여 보고하는 바이 다.(5)
방 법
1996년부터 2004년까지 삼성서울병원에서 시행한 18예 의 대동맥 스텐트 그라프트 삽입술을 시행받은 환자 중 신 장동맥 하방의 복부대동맥류로 시술받은 11예를 대상으로 후향적 조사를 하였다. EVAR의 시술은 파열되지 않은 신 장동맥 하방의 AAA로서 Table 1과 같은 적응증을 사용하 였다. 즉, AAA의 직경이 5 cm 이상이거나 AAA 직경이 빨
복부대동맥류에 대한 Endovascular Aneursym Repair의 치료 경험
성균관대학교 의과대학 삼성서울병원 1혈관외과, 2영상의학과
김장용1․도영수2․신성욱2․김영욱1․김동익1
Experience of Endovascular Aneurysm Repair in Abdominal Aortic Aneurysm
Jang Yong Kim, M.D.
1, Young-Soo Do, M.D.2, Sung-WookShin, M.D.
2, Young-Wook Kim, M.D.1, and DongIk Kim, M.D., F.A.C.S.1Purpose: We report our experience of endovascular aneurysm
repair (EVAR) in Korea.Methods: The medical records of 11 EVARs between 1996
and 2004 in the Samsung Medical Center were reviewed retrospectively.Results: The abdominal aortic aneurysm (AAA)s were cla-
ssified into 6 type A, 2 type B, 1 type C, 1 type D and 1 type E according to the anatomy. The indication of EVAR were the patient’s choice (7) and the high surgical risk (4).The stent grafts used were Vanguard (4), AneuRX (3), Nitis-s (3), and the S&G (1). The mean time of the pro- cedure, intensive care unit and post-procedral hospital stay were 3.9±0.8 hours, 25.1±13.6 hours and 7.9±2.8 days.
There was no procedure related complications. After angio- graphy had been performed, 1 type I endoleak and 5 type II endoleaks were found. The type I endoleak was treated with an extension of the stent-graft. The 4 type II endoleaks disappeared while the 1 type II endoleak was treated with glue embolization. During the follow up, 1 type I, 3 type II, and 3 type III endoleak were found. The type I endoleak was treated with glue embolization and the 3 type II endo- leaks disappeared. The 2 type III endoleaks were treated with aortounilateral stent-graft insertion and a femorofemoral bypass, followed by a conversion to open repair. The 1 patient with the type III endoleak refused treatment. There was no 30-day mortality but 5 late mortalities. The causes of death were 2 myocardiac infarctions, 1 hepatoma, 1 pneu- monia and 1 sepsis.
책임저자:김동익, 서울시 강남구 일원동 50번지 ꂕ 135-710, 삼성서울병원 혈관외과 Tel: 02-3410-3467, Fax: 02-3410-0040 E-mail: [email protected]
접수일:2006년 1월 10일, 게재승인일:2006년 4월 10일
Conclusion: EVAR can be performed safely in high-risk
patients but additional procedures may be needed during the follow-up. EVAR can be alternative option for the treatment of AAA in Korea if the experience of EVAR increases and the results improve. (J Korean Surg Soc 2006;71:112-118)Key Words: Abdominal aortic aneurysm, Stent, Graft
중심 단어: 복부대동맥류, 스텐트, 그라프트 ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Division of 1Vascular Surgery and 2Radiology, Samsung Medi- cal Center, Sungkyunkwan University School of Medicine, Seoul, Koreaꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
리 증가하는 환자 중 EVAR 적응증이 되는 환자를 대상으로 시행하였다. 시술 전 CT angiography와 conventional an- giography를 시행하여 stent-graft의 직경과 길이를 측정하였 다. 시술은 전신마취 혹은 국소마취하에 혈관조영실에서 시행되었다. 시술 중 발생할 수 있는 응급상황에 대비하여 수술로의 전환이 가능하도록 수술준비를 하고 시행하였으며
EVAR 후에 completion angiography를 시행하여 endoleak 유무 를 확인하였다. 시술 후에 외과 집중치료실에서 경과관찰을 한 후에 일반병동으로 전원하였다. 시술 후 1개월, 3개월, 6개월, 12개월 그리고 매 1년마다 단순 복부 X선 촬영과 CT angiography를 시행하면서 경과관찰을 시행하였다.
Endoleak는 EVAR 후에 stent-graft와 동맥류 사이에 혈류가 지속되는 것으로 정의한바, type I endoleak는 seal failure 로 stent-graft의 근위접합부위 또는 원위접합부위에서 발생 한 것, type II endoleak는 retrograde flow로 열려있는 요추 동맥이나 하장간 동맥에서 발생한 것, type III endoleak는 stent-graft defect로 또는 stent-graft간의 연결부위에서 발생 한 것, type IV endoleak는 fabric porosity에 의해 발생한 것, type V endoleak는 endotension에 의해 발생한 것으로 정의하 였다.(6) Migration은 경과관찰 중 시행한 CT angiogrophy 소 견에서 이전 CT angiography와 비교하여 device가 신장동 맥을 기준으로 10 mm 이상 상하 이동한 것으로 정의하 였다.(7)
결 과
시술 전 환자 AAA의 해부학적인 분류, demographics, 그 리고 동반질환 EVAR를 시행받은 환자 11예 중 성별 분포 는 남자 9명, 여자 2명이고 환자의 나이는 평균 69.5세(55∼
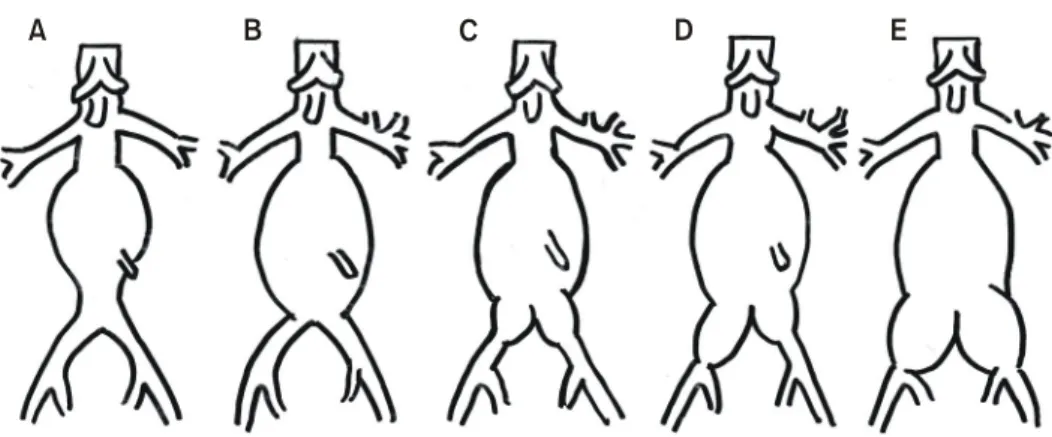
79)였다 복부대동맥류의 해부학적 모양에 따른 분류는 type A 6예, type B 2예, type C와 type D, type E가 각각 1예였다 (Fig. 1).(8) 본 시술의 적응증이 되는 환자 중 7예는 환자가 원하여서 시술되었으며, 4예는 고식적인 방법의 수술에 관 련된 고위험군으로 분류되어 저자들에 의해 선택되었다.
고위험군는 항문암으로 mile's operation 예정인 환자 1예,
Fig. 1. Classification of AAA. (A) AAA without involvement of distal aorta, (B) AAA with involvement of distal aorta but without involvment of common iliac artery, (C) AAA with involvement of common iliac artery and capable of distal sealing of stent graft in both common iliac artery, (D) AAA with involvement of common iliac artery and capable of distal sealing of stent graft in one common iliac artery and one external iliac artery, (E) AAA with involvement of common iliac artery and capable of distal sealing of stent graft in both external iliac artery.
A B C D E
Table 1. Inclusion criteria
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ Candidate for AAA* treatment
Infrarenal AAA AAA diameter>5 cm Rapid growing AAA
Exclusion: pararenal, suprarenal, ruptured, AAA Candidate for endovascular treatment
Adequate iliac/femoral access (for each device introduction system) No aneurysmal infrarenal aortic segment (neck)
Length>15 mm, 18 mm<diameter<28 mm, angle<60
oto long axis of aneurysm angle<45
oto suprarenal aorta, no inverted funnel shape
Iliac artery distal fixation site
Length>10 mm, 7.5 mm<diameter<20 mm, not severe calci fication and tortuosity
No allergy to contrast agent Serum creatinine≤1.7 mg/dl Not pregnant
Willingness to comply with required follow-up No bleeding disorder
No current infection
No connective tissue disorder
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*abdominal aortic aneurysm.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
만성신부전으로 혈액투석을 받고 있고 심한 양쪽 경동맥협 착증이 있는 허혈성 심장질환 환자 1예, 중증의 만성 폐쇄 성 기관지염 환자 2예였다.
1) 시술방법, 추가적인 시술 시술 직후 결과
사용된 stent-graft의 종류는 Vanguard (Boston Scientific, Natick, Mass., USA) 4예, AneuRX (Medtronic/AVE Inc, Santa Rosa, Calif., USA) 3예, Nitis-S (태웅, 서울, 한국) 3예, aorto- unilateral stent-graft (S&G Biotech, 성남, 경기도, 한국) 1예였 다. 시술을 위한 동맥절개는 10예에서 양측 대퇴동맥, 1예 는 일측 대퇴동맥만을 절개하였다. 시술은 10예에서 전신 마취, 1예에서 국소마취하에서 시행되었고 시술에 걸린 시 간은 평균 3.9±0.8시간이었으며, 시술 후 중환자실에 머무 른 시간은 평균 25.1±13.6시간이었다. 시술 후 퇴원까지 걸 린 시간은 평균 7.9±2.8일이었다. 시술 전에 내장골 동맥에 대한 코일 색전술은 3예에서 시행되었다. Stent-graft 시술
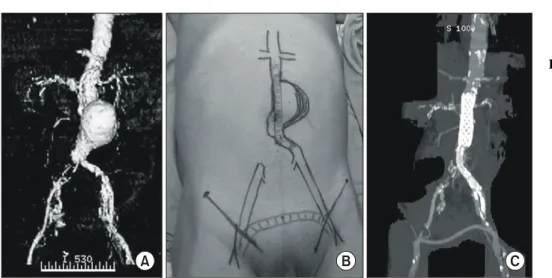
Fig. 2. EVAR with femorofemoral
bypass: Patient with AAA and right common iliac artery occlusion underwent aortomonoiliac stent-graft insertion and femorofem- oral bypass. (A) 3D recon- struction of preoperative CT angiography, (B) Gro- ss photography illustra- ting operative plan, (C) 3D reconstruction of postoper- ative CT angiography.
A B C
Table 2. Procedures and related findings
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ n (percent) ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Anesthesia
General 10 (90.9%)
Regional
Local 1 (9.1%)
Duration
Procedure (min) 234±487 (150∼318)
Duration of ICU stay (hours) 25.1±13.6 Duration of administration (days) 11.3±4.8 (6∼22) Arteriotomy
Femoral artery
11 (100%) Iliac artery
Additional procedure
Femoro-femoral bypass 1 (9.1%) Renal artery stent 1 (9.1%)
PTA* 2 (18.2%)
Endarterectomy Iliofemoral bypass
Uncovered stent crossing renal artery Embolisation of side branches
Internal iliac artery 3 (27.3%) (bilateral 2, left 1) IMA
†, IIA
‡, lumbar artery 0
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*percutaneous angioplasty;
†inferior mesenteric artery;
‡internal iliac artery.
Table 3. Midterm results
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
Completion F/U
angiography (11) (mean 35 months) ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Type I endoleak 1* 1
†Type II endoleak 5 3
Type III endoleak 0 3
‡Type IV endoleak 0
Migration 0
Conversion
§0 1
AAA
∥rupture 0
AAA growth 0
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*proximal extension of stent-graft (Vanguard);
†glue embilization
(AneuRX);
‡conversion to open repair of AAA (Vanguard, 3.8
years), insertion of Aortomonoiliac stent-graft and femorofemoral
bypass (Taewoong, 4.7 years), treatment refusal and loss of follow
up (Vanguard, 6.9 months);
§conversion to open repair;
∥abdominal
aortic aneurysm.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
중 대퇴-대퇴동맥 우회술 1예, renal artery stent 1예, per- cutaneous angioplasty (PTA) 1예를 추가로 시행하였다(Table 2). 대퇴-대퇴동맥 우회술을 시행한 1예는 aortomonoiliac stent
(S&G Biotech)를 삽입하였다(Fig. 2). 시술 중 시술과 관련된 합병증으로 개복하여 대동맥류 수술로 전환된 예는 없었다.
Fig. 3.
Open repair of AAA with Type III endoleak: patient with type III endoleak af- ter 3.8 years of EVAR un- derwent open repair of AAA and aortobiiliac re- construction. (A) 3D re- construction of CT angio- graphy showing type III endoleak, (B) Gross pho- tography of intraoperati- ve finding showing stent- graft disconnection, (C) Gross photography after aortobiiliac reconstruction.
A B C
Fig. 4. Combined treatment of AAA with type III end- oleak: patient with type III endoleak after 4.7 years of EVAR under- went aortomonoiliac st- ent graft insertion and fe- morofemoral bypass. (A) Axial film of CT angio- graphy showing type III endoleak, (B) 3D re- construction of CT angi- ography showing type III endoleak, (C) 3D recon- struction of CT angio- graphy after aortomonoi- liac stent graft insertion and femorofemoral by- pass.
A
B C
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
2) 시술 직후와 경과관찰(합병증, 사망)
시술 직후 시행한 completion angiography에서 endoleak가 6예(type I endoleak 1예, type II endoleak 5예)에서 발견되었 는데, type I endoleak에 대해 stent graft extension 시행하였으 나 endoleak 지속되어 경과 관찰하던 중 48개월에 type III endoleak가 발생하여 개복하여 대동맥류 수술 후 aortobiiliac reconstruction을 시행하였다(Vanguard, Fig. 3). Type II endo- leak 5예 중 4예는 경과관찰 중(시술 4일 후 2예, 시술 7일 후 1예, 시술 5개월 후 1예)에 소실되었고, 1예는 endoleak가 지속되어 경과관찰 29개월에 glue를 사용하여 색전술(glue embolization)을 시행하였다. 시술 직후 시행한 completion angiography에서는 endoleak 없었으나 시술 후 경과관찰 중 type II endoleak가 3예에서 관찰되었는데(시술 후 3일, 4일, 4일) 경과관찰 중에 치료 없이 소실되었다. 시술 후 22개월 에 type I endoleak가 발생한 1예는 glue embolization으로 치 료하였다. 또한, 시술 후 경과관찰 중 type III가 3예에서 발 생하였는데 1예는 앞에 기술하였고 1예는 경과관찰 57개월 에 type III endoleak가 발생하여 aortomonoiliac stent graft를 삽입하고 femorofemoral bypass를 시행하여 치료하였다(Fig.
4). 나머지 1예는 치료를 거부하였다(Table 3). 전체 11명 중 5명은 생존하여 있으며 1예는 확인이 불가능하였다. 사망 한 5예의 원인으로는 심근경색 2예(시술 후 43개월, 60개월 사망), 간암 1예(시술 후 58개월 사망), 폐렴과 피부병에 의 한 폐혈증이 각각 1예(시술 후 59, 12개월 사망)였다(Table 4). 환자의 시술 후 경과관찰은 평균 35±20개월(7∼66개 월)이었다.
고 찰
EVAR는 1991년 Parodi가 처음 시술한 이후 EVAR의 임상
연구들이 1995년 전후로 많이 시작되었다.(1) 초기의 stent- graft는 home-made tube device로 임상연구 이후 사라졌고, 이 후 EVAR 시술 초기에 시판된 stent-graft들은 임상에 사용되 면서 개량되었다. 현재에도 일부는 사라지고 일부는 새로 시 도되고 있다. 1999년 이후 미국 FDA에서 AnCure (Guidant, Menlo Park, Calif., USA), AneuRx (Medtronic/AVE Inc, Santa Rosa, Calif., USA), Excluder (W.L. Gore, Flagstaff, Ariz., USA), PowerLink (Endologix, Inc, Irvine, Calif., USA), Zenith (Cook Inc, Bloomington, Ind., USA)의 임상사용을 허가하였고(9) 이 후 미국에서는 신장동맥하방의 AAA의 치료로 시행되는 EVAR의 비율이 크게 증가하였다.(10) 그러나, 지금까지 국 내에서는 EVAR의 치료성적에 대한 보고는 미미하였다.
EVAR에 대한 치료결과를 분석하기 위한 항목으로 본 연구 에서는 EUROSTAR (European Collaborators on Stent/graft Techniques for aortic Aneurysm Repair) Registry에서 시도되 었던 항목을 중심으로 분석하고자 하였다.(8)
EUROSTAR Registry에서 대동맥류를 대동맥류와 동반되 어 있는 장골 동맥류의 해부학적인 위치에 따라 분류하였 다. Type A와 B는 대동맥에 국한된 대동맥류로 Type A는 대동맥 장골동맥 이행부 상방까지 포함된 경우, Type B는 대동맥 장골동맥 이행부를 포함한 경우로 bifurcated stent-graft가 필요하고 원위 접합부를 총 장골동맥에 할 수 있다. Type C, D, E는 장골 동맥류가 동반되어 있는 경우로 원위 접합부가 장골동맥류의 정도에 따라 달라질 수 있다.
Type 1 endoleak를 예방하기 위해 원위 접합부는 적어도 1 cm의 접합이 필요하다. Type C는 장골 동맥류가 총 장골동 맥의 일부에만 발생하여 양쪽 원위 접합부를 총 장골동맥 에 하는 것이 가능한 상태이고, Type D는 한쪽 장골 동맥류 는 장골 동맥 전체에 발생하여 원위 접합부를 외장골 동맥 에 위치시켜야 하고, Type E는 양쪽 장골 동맥류가 총 장골 동맥 전체에 발생하여 양쪽 원위 접합부를 외장골 동맥에 위치시켜야 한다. 시술 시 한쪽 내장골 동맥을 막는 것은 시술 후 합병증의 위험성이 높지 않지만, 양쪽 내장골 동맥 을 막게 되면 시술 후 합병증의 발생 가능성이 높아 주의가 필요하다.(11,12)
EVAR 시술에서 시술시간과 EVAR 시술 중 개복 대동맥 류 수술로의 전환은 learning curve를 반영하는데, 본 연구에 서 EVAR의 시술시간은 평균 234±487분이었으나 시술 중 개복 대동맥류 수술로의 전환은 없었다. 시술시간이 평균 144±67분인 EUROSTAR Registry 결과와 큰 차이를 보였지 만 대동맥류 수술로의 개복전환은 1.6%인 EUROSTAR Reg- istry 결과와 차이가 없었다.(8) 시술시간은 향후 향상될 것 으로 생각된다. 또한 본 연구에서는 시술 중에 시술과 관련 된 합병증은 없었지만 EUROSTAR Registry의 보고에서는 기구와 관련된 합병증으로 delivery sheath를 삽입하지 못한 경우(1.6%), 기구를 설치하지 못한 경우(1.2%), 기구 폐색 (0.1%), 기구의 한쪽 폐색(0.2%), 기구 협착(0.2%), 기구의
Table 4. Mortality
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
Cause n
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ All death (0∼30 days) 0/11
All death (>30 days) 5/11 AAA* related death 0 Non AAA related death 5/11 Cardiac 2 (MI, 43, 60 months)
Cancer 1 (hepatoma, 58 months)
Pulmonary 1 (pneumonia, 59 months) 1 (sepsis due to exfoliative Other
dermatitis, 12 months) Unknown 1/11 (follow-up loss, 7 months) ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*abdominal aortic aneurysm.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
한쪽 협착(0.2%), 기구의 이동(migration) (1.4%), 시술과 관 련된 합병증으로 개복 대동맥류 수술로의 전환(1.6%), ex- tra-anatomical bypass (0.4%), 그리고 동맥과 관련된 합병증 으로 지속되는 혈전증(0.3%), 지속되는 말단부 색전증 (0.2%), 신동맥 폐색(0.1%) 등을 보고하였다.(8)
본 연구에서 시술 후 30일 이내의 사망률은 0%였고 경과 관찰 중에 5예가 AAA와 관계없이 사망하였다(Table 4). 1예 는 시술 12개월 후 exfoliative dermatitis에 의한 패혈증, 2예 는 시술 후 43개월, 60개월에 발생한 심근경색증, 1예는 시 술 후 58개월에 시술 후 발견된 간암 그리고 1예는 시술 후 58개월에 만성 폐쇄성 기관지염의 합병증인 폐렴으로 사망 하였다. 이는 시술건수는 적지만 EVAR 시술 후 30일 이내 의 사망률이 0.8∼2.1%라는 보고와 유사한 결과로 생각된 다.(13-17)
(Table 5)
기구의 안정성(durability)을 나타내는 것으로 시술 후 동 맥류의 파열, 시술 후 AAA와 관련된 사망률, 경과관찰 중 개복 대동맥류 수술로의 전환, 경과관찰 중 추가되는 시술 을 고려할 수 있다. 본 연구에서 시술 후 동맥류의 파열, 시 술 후 AAA와 관련된 사망은 없었지만 경과 관찰 중 type III endoleak가 11예 중 3예(27.2%)에서 발생하였다. 총 3예의 type III endoleak 중 2예는 Vanguard에서 발생하였는데, Van- guard는 기구의 이동(migration)과 Type III endoleak의 여러 보 고 후에 1999년 시장에서 퇴출되었다.(18) 그 외 AneuRX, Nitis-S 그리고 S&G사의 stent-graft는 현재 임상에서 사용되 고 있다. 최근 stent-graft는 경과관찰 중 개복 대동맥류 수술 로의 전환을 2∼5%로 보고하고 있다(Table 5).(7,9,13-17) EVAR 시술과 관련하여 발생할 수 있는 합병증으로 end- oleak, 기구의 이동(migration), 기구의 파열(stent-graft fracture) 또는 분리(disconnection)가 있는데, 본 연구에서 type I endo- leak는 2예(18.2%), type II endoleak는 8예(72.7%)였고 기구 의 이동(migration)은 없었다. 기구의 파열(stent-graft frac- ture) 또는 분리(disconnection)로 인한 문제는 type III와 연관 된 문제로 앞에 기술하였다. Type II endoleak는 가장 흔한
endoleak로 자연 소실되는 경우가 많아 일정기간의 경과관 찰이 필요한 것으로 보고되었고,(6) 본 연구에서도 특별한 치료 없이 소실되었다. 하지만 type I endoleak는 치료를 요 하는 것으로 알려져 있는 데,(6) 2예 중 1예는 stent-graft를 추가로 삽입하였지만 실패 후 경과관찰 중 type III endoleak 로 수술을 시행받았고, 1예는 glue embolization으로 치료하 였다. 기구의 이동(migration)은 본 연구에서는 발생하지 않 았지만, 시술 후 1∼5% 발생한다고 보고되었다(Table 5).
(13-17)
EVAR는 시술 후 경과관찰 중 추가적인 시술이 필요한 경우가 많아 경과관찰이 필수적이다. 무작위 전향적 연구 로는 EVAR trial 1과 DREAM trial의 30일 유병률과 30일 사망률이 발표되었는데 이들의 결과는 EVAR가 개복 대동 맥류 수술보다 30일 사망률은 적지만 endoleak 등으로 추가 적인 시술은 더 많이 필요한 것으로 보고하였다.(2,3) 또한 초기에 개복 대동맥류 수술과 비교하여 초기에 EVAR의 시 술비용이 적게 든다고 보고되었지만 경과관찰의 비용과 추 가되는 시술의 비용을 고려하여 보면 오히려 비용이 더 필 요한 것으로 보고되었다.(4) 따라서 시술 전에 환자와 경과 관찰의 필요성에 대해 충분히 상의하고 환자의 이해가 반 드시 선행되어야 한다.
최근의 stent-graft는 기존의 결과보다 더 좋은 결과가 기 대되어 향후 더 많은 시술이 이루어질 것으로 생각된다.